
Abstract
Cholestatic liver diseases result from gradual destruction of bile ducts, accumulation of bile acids and self-perpetuation of the inflammatory process leading to damage to cholangiocytes and hepatocytes. If left untreated, cholestasis will lead to fibrosis, biliary cirrhosis, and ultimately end-stage liver disease. Primary biliary cholangitis (PBC) and primary sclerosing cholangitis (PSC) are the two most common chronic cholestatic liver diseases affecting adults, and their etiologies remain puzzling. While treatment with ursodeoxycholic acid (UDCA) has significantly improved outcomes and prolonged transplant-free survival for patients with PBC, treatment options for UDCA nonresponders remain limited. Furthermore, there is no available medical therapy for PSC. With recent advances in molecular biochemistry specifically related to bile acid regulation and understanding of immunologic pathways, novel pharmacologic treatments have emerged. In this review, we discuss the standard of care and emphasize the various emerging treatments for PBC and PSC.
Keywords
Introduction
Primary biliary cholangitis (PBC), previously known as primary biliary cirrhosis, is characterized by immune-mediated injury to intrahepatic biliary epithelial cells leading to cholestasis, fibrosis, and biliary cirrhosis.1–4 The exact underlying etiology for this cascade of events remains unclear but is most likely multifactorial, involving genetic predisposition and exposure to environmental factors. 5 Current guidelines recommend 13–15 mg/kg/day ursodeoxycholic acid (UDCA) as first-line treatment for PBC. 1 UDCA is hepatoprotective: it has choleretic and immunomodulatory properties and stimulates biliary bicarbonate secretion. 6 While UDCA is very well tolerated and can ultimately improve survival free of liver transplantation,7–15 approximately 40% of patients do not respond to UDCA and are at risk for progression.7,11,12,16,17 Indeed, the 10-year cumulative incidence of hepatic complications among UDCA nonresponders is >30%. 18 These patients must be identified early and considered for adjuvant therapies. Figure 1 illustrates the various classes of drugs currently under evaluation for cholestatic diseases. In 2016, obeticholic acid (OCA) received accelerated approval by the US Food and Drug Administration (FDA) for use in PBC after demonstrating beneficial effects on liver biochemistries in roughly 50% of patients with inadequate response to UDCA. 19 The benefits and overall effects of OCA in PBC will be described in detail in the next section. Despite the advent of UDCA and OCA, a subset of PBC patients continue to progress to end-stage liver disease and hepatocellular carcinoma.
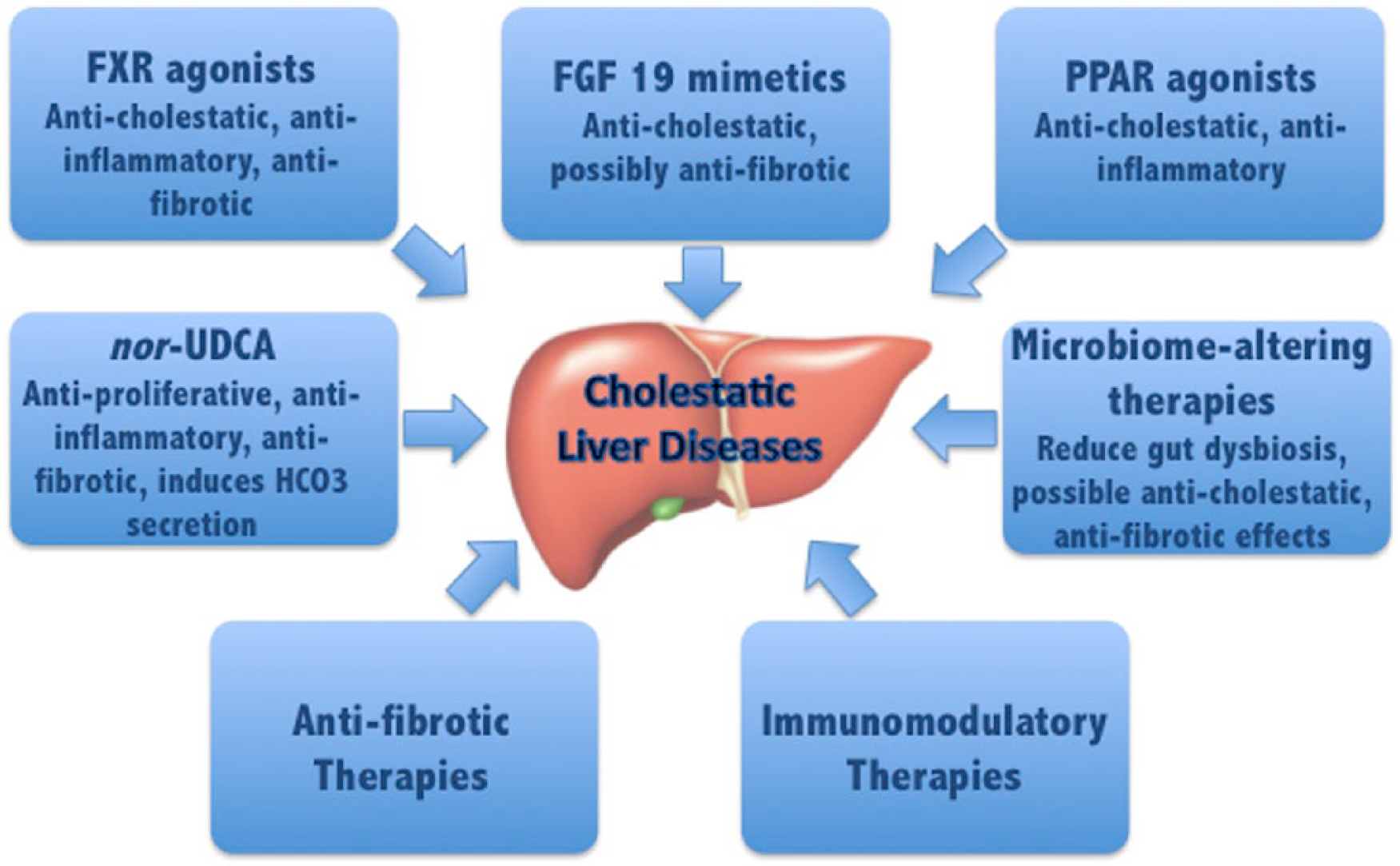
Novel classes of therapies for cholestatic liver diseases.
Primary sclerosing cholangitis (PSC) is a challenging, idiopathic cholestatic liver disease marked by chronic and progressive biliary inflammation, bile duct stricturing and fibrosis. Inflammatory bowel disease (IBD) is present in approximately two thirds of the affected population, and patients have a substantially increased lifetime risk for cholangiocarcinoma, gallbladder adenocarcinoma and colorectal cancer.20,21 In contrast to PBC, the efficacy of UDCA for PSC is still uncertain and guidelines provide conflicting recommendations. 22 Previous studies showed biochemical improvement with UDCA 13–15 mg/kg/day, but failed to demonstrate significant benefit on important outcomes, such as death or transplant-free survival.23,24 Subsequently, a randomized placebo-controlled study of 219 patients compared medium doses of UDCA (17–23 mg/kg/day) versus placebo for 5 years and showed a trend toward improved survival among UDCA-treated patients. 25 However, doses of 28–30 mg/kg/day were clearly associated with more frequent serious adverse events: patients receiving higher doses of UDCA were more likely to reach an endpoint, including cirrhosis, esophageal varices, cholangiocarcinoma, liver transplantation and death compared with those receiving placebo. 26 Furthermore, a subanalysis including patients with PSC and ulcerative colitis (UC) reported an increased risk of colorectal neoplasia among those receiving the high dose UDCA. 27 Multiple meta-analyses examining large numbers of PSC patients have also failed to show any survival benefit with UDCA.14,28–31 Importantly, all trials were judged to be at high risk of bias and the overall quality of evidence was very low. As of today, treatment for PSC is limited and liver transplantation is the only intervention shown to prolong survival.
Novel therapies
Farnesoid X receptor agonists
The farnesoid X receptor (FXR) is a nuclear hormone receptor involved in the regulation of bile acid homeostasis. FXR activation leads to downregulation of bile acid synthesis, increase in bile acid clearance, and reduction in liver and intestinal bile acid reabsorption.6,32 Ligand-activated FXR binds to promoter regions on its target genes, including the short heterodimer partner (SHP), fibroblast growth factor 19 (FGF 19) and several transporters such as the bile salt export pump and organic solute transporter α/β. In turn, SHP suppresses the production of cholesterol 7-alpha-hydroxylase (CYP7A1) in the liver, the rate-determining enzyme in bile acid synthesis. 6 In addition to bile acid regulation, FXR plays an important role in lipid and glucose homeostasis and protects against pathogen recognition and inflammatory signaling (PAMP)-induced inflammation via downregulation of NF-kB pathways. 33 Therefore, activation of FXR results in an anti-inflammatory and anticholestatic environment that reduces exposure of the liver to toxic bile acids. 34 Interestingly, FXR activation has also shown antifibrotic properties in multiple animal models.35,36
OCA has very strong affinity for FXR. The POISE trial randomized 216 PBC patients to receive placebo, OCA 5–10 mg (initial dose of 5 mg with ability to titrate to 10 mg if tolerated), or OCA 10 mg daily. This study demonstrated that 12 months of OCA treatment was associated with a significant improvement in alkaline phosphatase (ALP) and total bilirubin when compared with placebo, and this effect was sustained for 2 years. 19 The primary endpoint of the study was lowering the alkaline phosphatase to <1.67 times the upper limit of normal, with a reduction of at least 15% from baseline, while maintaining a normal total bilirubin level. The percentage of patients that met the primary endpoint was 46% in the 5–10 mg group and 47% in the 10 mg group, as opposed to 10% in the placebo group (p < 0.001 for both comparisons). Furthermore, an incremental benefit was observed with adjustment from 5 mg to 10 mg daily dosing. Table 1 summarizes findings of clinical trials with OCA and other novel therapies in cholestatic diseases.
Main findings related to the novel drugs in PBC and PSC.

ALP, alkaline phosphatase; ALT, alanine aminotransferase; AST, aspartate aminotransferase; ATRA, all-trans retinoic acid; C4, complement 4; CRP, C-reactive protein; FGF 19, fibroblast growth factor 19; FMT, fecal microbiota transplantation; FXR, farnesoid X receptor; GGT, gamma-glutamyltransferase; GI, gastrointestinal; HDL, high-density lipoprotein; IBD, inflammatory bowel disease; IgA, immunoglobulin A; IgG, immunoglobulin G; IgM, immunoglobulin M; IL-12, interleukin 12; IL-23, interleukin 23; LOXL2, lysyl oxidase-like 2; norUDCA, 24-norursodeoxycholic acid; OCA, obeticholic acid; PBC, primary biliary cholangitis; PPAR, peroxisome proliferator-activated receptor; PSC, primary sclerosing cholangitis; RCT, randomized clinical trial; RXR, retinoid X receptor; TNF-α, tumor necrosis factor alpha; UDCA, ursodeoxycholic acid.
In the POISE trial, serum markers of liver fibrosis did not differ significantly between the treatment groups and placebo. In addition, treatment with OCA resulted in a decrease in the high-density lipoprotein (HDL) cholesterol and triglyceride levels, and an initial mild increase in the low-density lipoprotein (LDL) cholesterol levels. Although patients with PBC typically have baseline elevation of HDL and are not at an increased risk for cardiovascular events, the long-term consequences of such OCA-induced changes in the lipid profile are yet to be determined.
Despite the demonstrated biochemical improvement, the incidence and intensity of pruritus were significantly increased in the treatment arms as compared with placebo, potentially limiting OCA use in some patients. Discontinuation rate due to pruritus was much higher in the 10 mg/day group compared with the 5–10 mg/day group, indicating that titration strategy successfully mitigated pruritus. Based on the POISE results, OCA was granted accelerated approval for treatment of PBC patients with incomplete response to UDCA or who are intolerant to UDCA. However, continued FDA approval of OCA is contingent on completion of a phase IIIb trial assessing hard clinical endpoints [ClinicalTrials.gov identifier: NCT01473524].
Use of OCA as monotherapy was also evaluated in another study comparing OCA 10 mg/day, OCA 50 mg/day and placebo in 59 patients with PBC. The study demonstrated similar biochemical effects: ALP was reduced by 53.9% and 37.2% in the OCA 10 mg and 50 mg groups, compared with 0.8% in the placebo group. 37 As expected, lower drug discontinuation rate and better tolerability were observed with 10 mg/day dosing compared with 50 mg/day.
After reports of hepatic decompensation, liver failure and deaths in 19 OCA-treated patients, an investigation determined that patients with Child B and C cirrhosis had been prescribed a higher than recommended dosage of OCA. As a result, in February 2018, the FDA issued a black box warning to the OCA label. 58 The Child-Pugh score must be calculated in patients with suspected liver cirrhosis; Child B and C patients should be started at 5 mg/week (as opposed to daily) and may be titrated up to 5 mg twice a week after 3 months if needed, and if drug is well tolerated.
To date, there is no definite evidence of improvement in long-term clinical outcomes with OCA use. However, a simulation study estimated that OCA in combination with UDCA as a second-line treatment for PBC could reduce the 15-year cumulative incidences of decompensated cirrhosis from 12.2% to 4.5%, hepatocellular carcinoma from 9.1% to 4.0%, liver transplants from 4.5% to 1.2%, and liver-related deaths from 16.2% to 5.7%. 59 Despite the expected substantial clinical benefit, OCA use is currently not cost effective and a significant cost reduction would be necessary to render its widespread use more feasible. 59
OCA is also being investigated for use in PSC. Specifically, a 24-week placebo-controlled randomized dose-ranging trial evaluated the efficacy and safety of OCA compared with placebo in 77 patients with PSC [ClinicalTrials.gov identifier: NCT02177136]. Patients were randomized to one of three treatment arms: placebo, OCA 1.5–3 mg and OCA 5–10 mg, with dose titration occurring at 12 weeks. Patients receiving 1.5 mg OCA with the option to titrate to 3 mg and patients in the OCA 5–10 mg group achieved a statistically significant reduction in serum ALP as compared with placebo at week 24, with ALP decreasing by 22% in both OCA groups and increasing by 1% in the placebo group. 38 As was the case with PBC, pruritus was the most common adverse event, occurring in 46%, 60% and 67% of patients in the placebo, OCA 1.5–3 mg and OCA 5–10 mg groups, respectively. An open label 2-year extension phase is ongoing.
Currently, three other FXR agonists are under evaluation for PBC. These novel molecules differ from OCA by being nonsteroidal, nonbile-acid derivatives. They include: GS9674, LJN452 and EDP-305 [ClinicalTrials.gov identifiers: NCT02943447, NCT02516605, and NCT03394924, respectively], all undergoing phase II testing. GS9674 is also in clinical development for PSC [ClinicalTrials.gov identifier: NCT02943460].
All-trans retinoic acid
Another potential target to treat cholestasis is the retinoid X receptor (RXR), a heterodimer of FXR. All-trans retinoic acid (ATRA) is a permissive activator of the nuclear receptor FXR/RXR and several in vitro and animal models have demonstrated treatment with ATRA decreased hepatic inflammation, fibrosis, bile duct proliferation, and bile acid pool size. Interestingly, a recent pilot study of ATRA combined with moderate-dose UDCA was performed in PSC patients and showed improvement in ALT and complement-4 levels, but unfortunately its effect on ALP did not reach statistical significance. 39
Fibroblast growth factor 19 mimetics
As mentioned, one of the many downstream effects of FXR activation is increased gene transcription of FGF 19, an enteral hormone known to repress bile acid synthesis via downregulation of CYP7A1.1,34 FGF 19’s anticholestatic benefit may be limited by its proproliferative and procarcinogenic properties, which in mouse models have been implicated in the development of hepatocellular carcinoma. 32 However, new molecules were developed with alterations to FGF 19’s amino acid sequence that may limit its procarcinogenic properties and promote its anticholestatic effect. 32 NGM282 is one such nontumorigenic FGF 19 derivative. In a phase II multicenter, randomized, double-blinded, placebo-controlled trial enrolling 45 patients with PBC who were inadequate responders to UDCA, NGM282 was administered as a daily subcutaneous injection of 0.3 mg or 3 mg versus placebo for 28 days. 40 Treated patients showed statistically significant reductions in ALP levels and other liver biochemistries. NGM282 was safe and well tolerated, with only mild adverse events reported, including diarrhea, nausea and headache.
NGM282 was also evaluated in a phase II trial for PSC [ClinicalTrials.gov identifier: NCT02704364]. Although results were not published, a press release statement from NGM Bio reported that NGM282 did not meet the primary study endpoint of lowering serum ALP (http://www.ngmbio.com/media/press-releases/020518/). However, the drug did reduce levels of serum bile acids, aminotransferases and markers of fibrosis; it is unclear whether it will be examined further in PSC.
Peroxisome proliferator-activated receptor agonists
Another key player in the regulation of bile acid homeostasis is the peroxisome proliferator-activated receptor, specifically the alpha and delta isoforms (PPARα, PPARδ).1,6 PPARα acts on nuclear transcription factors to reduce inflammation and promote bile acid excretion through stimulation of multidrug resistance protein 3. 34 Fibrates are the most well-known class of drug to activate PPARα. 6 While published clinical trials examining fibrates in PBC are small, most patients had a significant biochemical response.43,60–66 Of significance, a large randomized controlled trial including 100 patients with PBC treated for 2 years with either UDCA/placebo or UDCA/bezafibrate (the BEZURSO trial) was presented at the International Liver Congress in 2017. Combination therapy with bezafibrate was associated with marked biochemical improvement, including 67% of patients normalizing their ALP and 30% normalizing all liver biochemistries, improvement in markers of fibrosis, and also symptomatic improvement in pruritus. 41 Similarly, an open-label study of 48 PBC patients treated with combination therapy of UDCA (13–16 mg/kg/day) and bezafibrate (400 mg/day) demonstrated an ALP decrease in all patients and normalization in 54%. Older patients with milder amounts of fibrosis (liver stiffness scores < 7.3 kPa) were more likely to normalize ALP. In addition, the study showed marked relief in pruritus among treated patients. 42 A meta-analysis on bezafibrate for PBC confirmed that the addition of bezafibrate improves liver biochemistries and can potentially improve prognosis, given the significant reduction in the Mayo risk score. 67 With the caveat that the meta-analysis was conducted prior to publication of the French and Spanish studies, it did not show a benefit on survival rate or pruritus.
In the US, an open-label study of 20 patients with PBC who had incomplete response to UDCA showed that combination therapy of UDCA and fenofibrate for 48 weeks led to a ⩾40% reduction in ALP in 55% of study subjects. 43 A recent meta-analysis of six studies of fenofibrate for PBC, including a total of 102 patients, found that 69% of patients with no or incomplete response to UDCA achieved a complete response when fenofibrate (100–200 mg/day) was added. 68 Pooled analysis showed that use of fenofibrate led to a significant decrease in ALP, gamma-glutamyltransferase (GGT), total bilirubin and immunoglobulin M levels.
Adverse events associated with fibrates include myalgias, arthritis, leg edema, polydipsia, hepatotoxicity and gastrointestinal upset (especially esophageal reflux and nausea).43,67 Studies have reported elevations of serum creatinine phosphokinase and serum creatinine levels, which should be monitored especially with long-term use, although a significant reduction in glomerular filtration rate has not been observed.62,69
The selective PPARδ agonist seladelpar was recently investigated in a 12-week randomized controlled trial of patients who did not respond adequately to UDCA. Seladelpar was associated with significant increases in liver aminotransferases in three patients and therefore the study was terminated early. Despite the early termination, however, all five patients who completed the 12 weeks of treatment with seladelpar had complete normalization of ALP. 46 As a result, an open-label study was initiated evaluating lower doses of 5 mg/day and 10 mg/day for 26 weeks [ClinicalTrials.gov identifier: NCT02955602]. Planned interim analysis conducted at 12 weeks demonstrated no safety concerns. ALP normalized in 18% and 45% of patients on 5 mg/day and 10 mg/day, respectively. 47 As a result, an even lower dose of 2 mg/day is currently under evaluation.
Elafibranor is a potent PPARα, δ agonist and is currently undergoing investigation in a phase II clinical trial involving 45 patients with PBC [ClinicalTrials.gov identifier: NCT03124108]. Another dual PPARα and γ agonist, saroglitazar, is under investigation in a phase II study examining its safety, tolerability and efficacy in treating PBC [ClinicalTrials.gov identifier: NCT03112681].
PPAR agonists have also been investigated for their potential usefulness in PSC, albeit only in a couple of small studies. Collective experience from a total of 25 patients treated with bezafibrate70,71 and 21 patients treated with fenofibrate44,45 for 3–12 months indicate that use of fibrates can lead to significant improvement of ALP, GGT and ALT. In addition, a systematic analysis including the 25 Japanese patients suggests that preserved liver function may predict biochemical response to bezafibrate. 72
24-norursodeoxycholic acid
One of the many scientific breakthroughs for understanding cholestasis stems from a belief that a hydrophilic environment combined with the production of bicarbonate protects cholangiocytes and hepatocytes from bile acid toxicity. 6 norUDCA (24-norursodeoxycholic acid) is a novel agent that lacks a methylene group compared with its relative, UDCA. 73 This missing methylene group allows norUDCA to be passively absorbed from cholangiocytes, through a process termed ‘cholehepatic shunting.’ 6 This results in the production of bicarbonate, creating a more hydrophilic and less toxic environment to hepatocytes and cholangiocytes.74–76 Experimental mouse models of cholangiopathies have shown promising results when treated with norUDCA, which demonstrated antiproliferative, antifibrotic and anti-inflammatory properties.77–80 A recent phase II clinical trial of 159 PSC patients randomized to various doses of norUDCA versus placebo demonstrated statistically significant dose-dependent reductions in ALP levels in treated patients compared with placebo as well as a favorable safety profile. 48 Such biochemical response was independent of prior response to UDCA and of disease stage. Therefore, use of norUDCA may play a significant role in the treatment of cholestasis. It is possible that norUDCA would have synergistic effects with UDCA, although this remains to be examined. A larger phase III study expected to enroll 300 patients with PSC is ongoing in Europe to further evaluate the safety and efficacy of norUDCA [EudraCT no.: 2016-003367-19].
Immunomodulatory treatments
The PBC liver is infiltrated with both T and B cells, leading to mass production of cytokines and chemokines that ultimately play a role in the pathogenesis of the disease.81,82 Rituximab, a monoclonal antibody targeting the CD20 antigen on the B cell, is used in a wide array of diseases including IBD, rheumatologic diseases, and various hematologic malignancies. Rituximab has been investigated for potential benefits in PBC as well. In one open-label study, six PBC patients with inadequate response to UDCA were treated with rituximab infusions and showed improvement in ALP levels. However, in another open-label study of 14 PBC patients, reductions in liver biochemistries were not as pronounced despite improvement in pruritus.49,50 Of interest, a phase II trial of rituximab versus placebo is underway for 78 PBC patients with complaints of fatigue to examine the potential benefit on these patients’ quality of life. 83 As of today, the evidence for rituximab’s efficacy in treating PBC is insufficient. Results of the RITPBC trial for fatigue are awaited.
Increased expression of interleukin 23 (IL-23) was observed in peripheral blood cells of patients with PBC, and IL-23 levels correlated with clinical disease stages.51,84–86 Furthermore, genes associated with the production of IL-12 were upregulated in genome-wide association studies and have been implicated in the pathogenesis of PBC.51,87 For these reasons, ustekinumab, a monoclonal antibody against IL-12 and IL-23, was examined in PBC patients who did not respond to UDCA; however, it failed to meet the primary endpoint of improvement in serum ALP after 28 weeks of therapy.1,51 The study has been criticized for enrolling patients with more advanced disease stages, which may not be expected to respond well to immunomodulatory therapies.
Abatacept is a monoclonal antibody that targets CD80 and CD86 on antigen-presenting cells and interferes with T-cell activation. As was the case with ustekinumab, abatacept also failed to meet the primary endpoint in a small study for PBC. 52
Evaluating the role of immunomodulatory therapy in cholestatic liver diseases is a challenging undertaking. The timing of therapy initiation is a major issue, as it is expected that patients in earlier disease stages are more likely to benefit from immunomodulation. However, currently, patients are selected for clinical trial participation based on nonresponse to UDCA, thus in a more advanced cholestatic phase already beyond that initial immune attack. Identifying patients at the very early disease stages is difficult and it is likely that we would need combination therapy targeting different disease processes at the same time, using, for instance, immunomodulatory drugs combined with anticholestatic agents. Furthermore, the appropriate study endpoint may not be serum levels of ALP, which is the marker of cholestasis currently used as primary endpoint in most clinical trials, and may involve obtaining serial liver biopsies for immunohistochemistry testing.
Immunomodulatory therapy has also been investigated in patients with PSC. Infliximab, a monoclonal antibody against tumor necrosis factor-α, used commonly in IBD, was investigated in a small number of PSC patients, without any clinical or histological benefit. 53 Other trials have examined the effects of methotrexate, mycophenolate mofetil, and etanercept, with no efficacy observed.88–90
Antifibrotic therapies
Fibrosis in PBC is believed to stem from T-cell-mediated damage and cholestasis-induced injury to biliary epithelial cells, with release of fibrogenic mediators that activate neighboring fibroblasts to secrete collagen, including transforming growth factor β1, platelet-derived growth factor BB and endothelin-1.73,91 In animal models, the FXR agonist OCA also has antifibrotic properties.92–94 While this has not yet been demonstrated in humans, the fact that OCA-treated patients in the POISE trial had improvement in the AST/platelet ratio index (APRI) scores hints at this possibility. Future studies looking at changes in liver stiffness, enhanced liver fibrosis scores and the APRI score will clarify this issue.
Of interest is the role of the vitamin D receptor (VDR) as the downward effects of this receptor are implicated in interfering with T-cell immune response. 6 Not only have VDR agonists shown playing a role in bile acid detoxification but, in mouse models, they have also demonstrated the ability to modulate fibrogenesis. 6 For these reasons, the VDR and its ligands are of interest in the treatment of fibrosis and further investigation in human trials is needed.
Other cellular targets are under investigation for their role in preventing fibrosis or inducing its regression, such as lysyl oxidase-like 2 (LOXL2). Simtuzumab is a monoclonal antibody directed against LOXL-2 which was evaluated in a 2-year study including 234 PSC patients [ClinicalTrials.gov identifier: NCT01672853]. Unfortunately, use of simtuzumab was not associated with a reduction in hepatic collagen concentration. 54
Manipulation of gut microbiome
The gut microbiome plays an important role in the regulation of both innate and adaptive immune systems through the gut–liver–immune-system axis. The gut microbiome composition is altered in several chronic liver diseases and has been implicated in the pathogenesis of alcoholic and nonalcoholic fatty liver disease, as well as in PBC and PSC. This dysbiosis generates an imbalance in production of cytoprotective versus injurious metabolites and may lead to abnormal immunological development. Important abnormalities may result, such as an increase in lipopolysaccharide in the portal circulation, a decrease in seven alpha-dehydroxylation by gut bacteria, and a subsequent accumulation of primary bile acids that leads to stimulation of FXR and downregulation of CYP7A1 in the liver.55,95 As a result, a bile-acid–intestinal-microbiota–cholestasis triangle has been postulated in the pathogenesis of PBC and PSC, suggesting a multidirectional interaction of these factors. Bile acids can modulate the gut microbiota by decreasing the pool of some bile-sensitive bacteria and facilitating proliferation of other species. Conversely, the microbiome can shape the bile acid pool and bile acid receptors. This disturbance in bile acid metabolism leads to the development and progression of cholestasis, which can further alter gut microbiota and exacerbate cholestasis in this interactive cycle. 96
Gut dysbiosis and reduced bacterial diversity is consistently found in patients with PSC. 95 Kummen and colleagues found that patients with PSC had a gut microbial signature distinct from both healthy controls and patients with UC without liver disease. 97 Interestingly, the microbiota of PSC patients with and without IBD was similar, however PSC-IBD patients were noted to have decreased diversity compared with patients with UC without biliary disease, and healthy controls. Over-representation of the Veillonella genus was noted only in PSC patients and, interestingly, enrichment with Veillonella has been linked to increased rates of fibrosis, not only in PSC but also in other fibrosing diseases such as idiopathic pulmonary fibrosis. Therefore, manipulation of the microbiota via antimicrobials, probiotics, or fecal microbiota transplantation (FMT) might offer new therapeutic options.
Several antibiotics have been examined in PSC, including vancomycin, metronidazole, minocycline, tetracycline and rifaximin.98–101 Despite modest improvements in liver biochemistries with most antimicrobials, evidence for long-term clinical benefit is lacking. Vancomycin is the most studied antibiotic and its use has been extensively reviewed. 102 Vancomycin use is consistently associated with a significant decline in ALP levels and PSC Mayo risk score.55,56 Interestingly, a trial that studied different dosing options for vancomycin and metronidazole demonstrated a significant decrease in total bilirubin levels with low-dose metronidazole and a decrease in pruritus with the high-dose metronidazole, but without improvement in ALP; only vancomycin met the primary endpoint of reduction in ALP. 55 A phase III study is now being conducted to assess the benefit of oral vancomycin for PSC in IBD patients [ClinicalTrials.gov identifier: NCT01802073]. In contrast, an open-label pilot study of oral rifaximin did not show significant changes in ALP levels and seemed inefficacious for the treatment of PSC. 57
Altering the gut microbiota without using pharmacological drugs is another promising approach. This can be achieved with probiotics and FMT. An open-label pilot study is evaluating the microbiological and clinical effects of FMT in 10 patients with PSC. Preliminary results showed that post-FMT patients had a ⩾50% decrease in ALP by week 26 and no adverse events were observed [ClinicalTrials.gov identifier: NCT02424175]. On the other hand, probiotics were studied in a crossover study of PSC patients with IBD, and no beneficial effects were demonstrated on biochemistries. 103 The use of various microbiome-altering modalities may play a role in the treatment of PSC, but further trials are needed.
Conclusion
New promising targets for the treatment of cholestatic liver diseases have emerged, with the recent advances in the knowledge of molecular mechanisms implicated in these diseases. FXR agonists represent an interesting option for treating cholestasis, with established benefits in PBC and possibly in PSC. Fibrates have been associated with significant biochemical improvement and have the added benefit of ameliorating pruritus. Fibrates appear to have greater efficacy in patients with lower fibrosis scores. Early identification of PBC patients who are nonresponders to UDCA and candidates for adjuvant therapy is paramount. Innovative treatments for PSC include norUDCA and microbiome-related therapies such as vancomycin and FMT. norUDCA in particular has antifibrotic, anticholestatic and anti-inflammatory properties and results of the proof-of-concept study were very encouraging. Furthermore, combination therapy affecting multiple pharmacologic targets with different mechanisms of action is an attractive approach for both PBC and PSC.
Footnotes
Acknowledgements
Priscila Santiago: literature review and drafting of manuscript.
Andrew R. Scheinberg: literature review and drafting of manuscript.
Cynthia Levy: literature review, drafting of manuscript, critical revision of manuscript for important intellectual content, expert supervision.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
PS and AS do not have any conflicts of interest to disclose.
CL is a consultant for Intercept, GSK and Novartis, receives research grants from Gilead, Genfit, Intercept, CymaBay, HighTide, Durect, Alnylan, NGM, Novartis, Enanta and Genkyotek, and is on the editorial board for Liver Transplantation.