
Abstract
On 31 December 2019, the WHO China Country Office was informed of cases of pneumonia of unknown etiology detected in Wuhan (Hubei Province of China). In January 2020, a new coronavirus named SARS-CoV2 was isolated and, since that time, SARS-CoV2 related disease (COVID-19) rapidly spread all over the world becoming pandemic in March 2020. The COVID-19 outbreak dramatically affected the public-health and the health-care facilities organization. Bilio-pancreatic endoscopy is considered a high-risk procedure for cross-contamination and, even though it is not directly involved in COVID-19 diagnosis and management, its reorganization is crucial to guarantee high standards of care minimizing the risk of SARS-CoV2 transmission among patients and health-care providers. Bilio-pancreatic endoscopic procedures often require a short physical distance between the endoscopist and the patient for a long period of time, a frequent exchange of devices, the involvement of a large number of personnel, the use of complex endoscopes difficult to reprocess. On this basis, endoscopic units should take precautions with adjusted management of bilio-pancreatic endoscopy. The aim of this article is to discuss the approach to bilio-pancreatic endoscopy in the COVID-19 era with focus on diagnostic algorithms, indications, management of the endoscopic room, proper use of Personal Protective Equipment and correct reprocessing of instrumentation.
Keywords
Introduction
In December 2019 clusters of patients with pneumonia of unknown origin epidemiologically linked to a local seafood market were reported in Wuhan, Hubei Province, China. Bronchoalveolar-lavage fluid samples, collected from patients with pneumonia of unknown origin, were inoculated in human airway epithelial and Vero-E6 and Huh-7 cell lines leading to the description of a novel betacoronavirus, initially named 2019-nCoV, now worldwide known as SARS-CoV-2. 1
Coronaviruses are enveloped, non-segmented positive sense RNA viruses. 2 Although those coronaviruses associated with human illness generally induce only mild upper respiratory diseases, SARS-CoV2, SARS-CoV and MERS-CoV can cause severe respiratory syndrome also in immunocompetent hosts.1,3,4 SARS-CoV2 related disease, named COVID-19, can present several clinical scenarios, ranging from asymptomatic to severe respiratory syndrome. Typically, the patients present a bilateral interstitial pneumonia that can lead to organ function damage, including Acute Respiratory Distress Sybdrome (ARDS), acute respiratory injury, acute renal injury and septic shock requiring for Intensive Care.5,6
The World Health Organization (WHO) declared COVID-19 as pandemic in March 2020. 7 The general reorganization of endoscopic units after COVID-19 outbreak has been described elsewhere 8 and it includes also the reorganization of bilio-pancreatic endoscopic units.
We reviewed the most relevant guidelines and recommendations published by international gastrointestinal endoscopy societies to examine the new organization of bilio-pancreatic endoscopy with focus on appropriate indications for Endoscopic Retrograde Cholangio-Pancreatography (ERCP) and Endoscopic Ultrasound (EUS), new diagnostic algorithms for bilio-pancreatic diseases, the proper use of personal protective equipment (PPE) and the correct reprocessing of instrumentation.
Methods
A literature search was done on PubMed, Web of Science, Embase and Scopus with the terms ‘Guidelines Covid19 AND Endoscopy’, ‘Covid19 AND Bilio-pancreatic Endoscopy’, ‘Covid19 AND ERCP/EUS’ and ‘Covid19 epidemiology AND pathogenesis’. The COVID-19 section of the WHO online website was used for the official definitions and data regarding the pandemic. The inclusion criteria were: original articles about endoscopy after COVID-19 outbreak, international guidelines, full text available. The exclusion criteria were: language other than English, abstract form only, case reports and small case series. About 90 papers and reports were found; of these 51 were chosen for analysis. Two authors, VB and TS, reviewed the selected papers.
SARS-CoV2 transmission and biological risk in endoscopy
The main route of diffusion of SARS-CoV2 is human-to-human transmission via droplets or via fomites, nevertheless other routes cannot be excluded. 9 Even though the risk of infection transmission is in the immediate vicinity of a SARS-CoV2 positive patient, droplets can be spread 1–2 m from the patient. 10 Endoscopy should be considered a high-risk technique; although no definitive data are available on whether endoscopy can be considered aerosol-generating, positive insufflation during the endoscopic procedures and the manipulation of accessories can increase the risk of aerosolizing the patients’ biological fluids. 11 Infectious disease exposure during endoscopy is a potential risk for both endoscopic personnel and patients. 12 It has been shown that the endoscopist’s face is exposed to potentially infectious biologic samples, in fact several studies indicate that Helicobacter Pylory infection is more common in endoscopic personnel, suggesting an exposure to microscopic droplets of gastric juice from infected patients. 13
As such, SARS-CoV2 transmission during bilio-pancreatic endoscopy could be particularly high. In fact, patients often require orotracheal intubation with high risk of generating aerosol; 14 procedures are frequently complex and may require a short physical distance between endoscopist and patients for a period of time that is generally longer than in standard gastroscopy and colonoscopy; the use of several accessories and the need of frequent exchange of devices, such as forceps, snares, nets, guidewires, balloons, may increase the risk of spreading biological fluids and raise the exposure rate; 15 during bilio-pancreatic endoscopy a large number of personnel is involved in the endoscopic procedure. After the COVID-19 outbreak all guidelines suggested to reduce this number to the minimum; however, at least four personnel are present in the endoscopy room: one expert endoscopist, two nurses and the anesthesiologist, increasing the risk of concomitant contamination. 11 The complex design of duodenoscopes and EUS-scopes makes them difficult to clean and makes possible a biofilm formation promoting microorganism overgrowth. 16
Before the endoscopic procedure, all patients should be carefully triaged and screened to assess a risk stratification. According to the WHO, 7 patients can be defined as confirmed case if a patient has laboratory confirmation of COVID-19 infection, irrespective of clinical signs and symptoms, probable case if in a suspect case tests for COVID-19 are inconclusive or cannot be performed or suspect case if: (a) a patient with acute respiratory illness (fever and at least one sign/symptom of respiratory disease, e.g. cough, shortness of breath), AND a history of travel to or residence in a location reporting community transmission of COVID-19 disease during the 14 days prior to symptom onset; (b) a patient with any acute respiratory illness AND having been in contact with a confirmed or probable COVID-19 case in the last 14 days prior to symptom onset; or (c) a patient with severe acute respiratory illness in the absence of an alternative diagnosis that fully explains the clinical presentation.
All patients referred to the endoscopic unit should be asked to fill in a questionnaire including the following issues: presence of fever, cough, sore throat or shortness of breath in the last 14 days; close contact with confirmed, probable or suspect cases; recent hospitalization; provenance from COVID-19 confirmed clusters.
Risk assessment for patients undergoing ERCP or EUS
Patients with bilio-pancreatic disease have often a rapid onset of symptoms and refer to the Emergency Room. In this clinical setting, it would be useful to perform a laboratory test for the research of SARS-CoV2 (polymerase chain reaction on pharyngeal and nasal samples) and a chest X-ray to carefully assess their risk of infection.
Patients can finally be classified as confirmed case (according to the WHO definition), high-risk case (presence of symptoms, contact with a confirmed, probable or suspect case or computed tomography (CT) scan suggestive hallmarks) and low risk (no symptoms and no contact with SARS-CoV2 positive cases), as summarized in Table 1. However, risk assessment with evaluation of signs, symptoms and history of travel or contact with suspected COVID-19 is inadequate to exclude SARS-CoV2 infection, given that transmission from asymptomatic carriers has been documented and that the prevalence of the disease is likely to be underestimated. On this basis, all patients elected for ERCP or EUS should be considered at high-risk of SARS-CoV2 transmission until proven otherwise.
Patient classification.

CT: computed tomography
Indications for ERCP and EUS
Bilio-pancreatic diseases are burdened with not negligible morbidity and mortality and endoscopy plays a significant role in their management. After the COVID-19 outbreak, in order to balance the patients’ health-care and the safety of health-care providers, indications for ERCP and EUS needed a remodulation as summarized in Table 2. Clinical cases should be divided into three groups: ‘emergency/urgency’, ‘deferrable’ and ‘need for discussion’.
Indications for Endoscopic Retrograde Cholangio-Pancreatography (ERCP) and Endoscopic Ultrasound (EUS) during the COVID-19 outbreak.
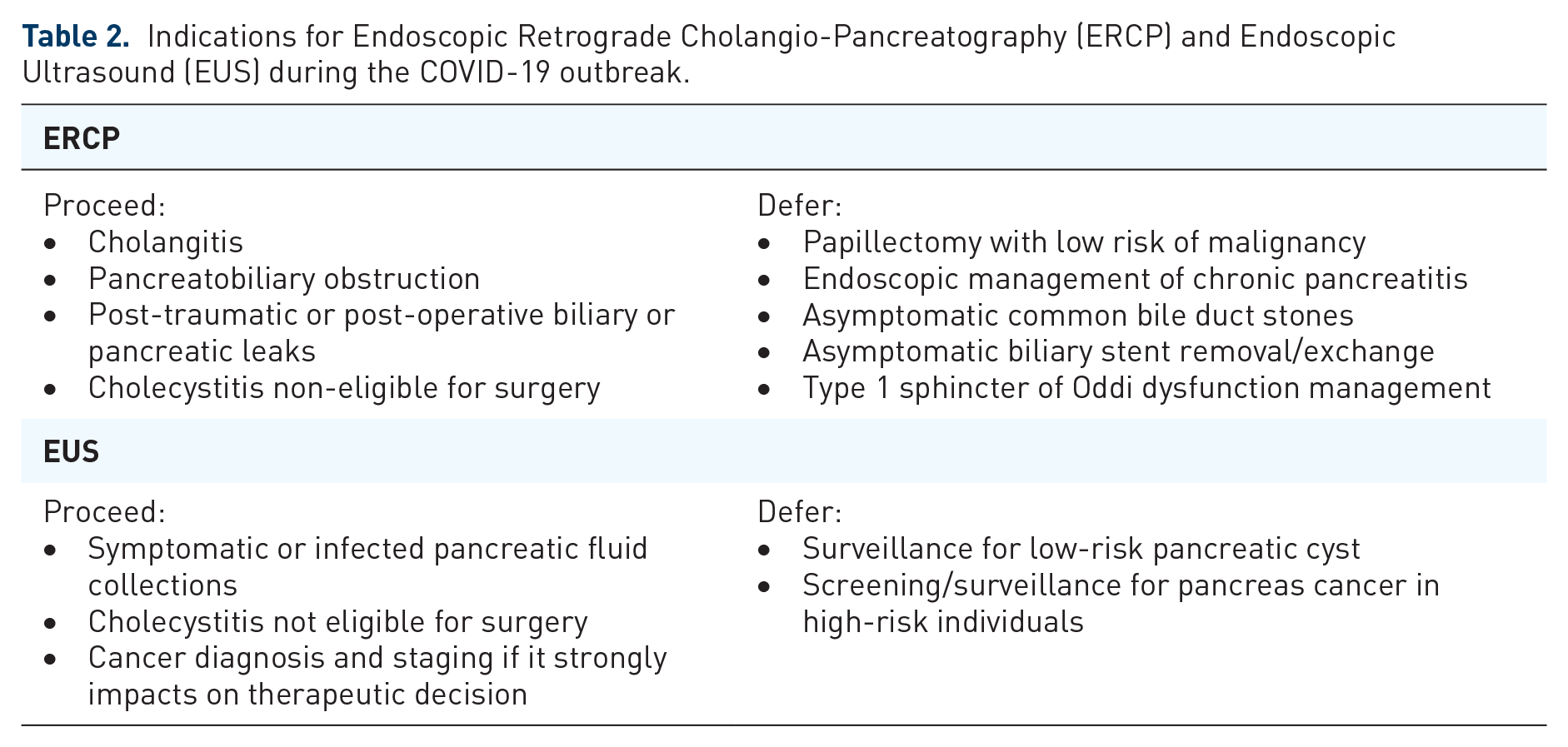
There is agreement between international endoscopic societies (Table 3) to defer elective procedures, such as EUS surveillance for low-risk pancreatic cyst and screening/surveillance for pancreas cancer in high-risk individuals, papillectomy, endoscopic management of recurrent acute pancreatitis or chronic pancreatitis, treatment of asymptomatic common bile duct stones, management of type 1 sphincter of Oddi dysfunction, stent exchange. 17
Endoscopic guidelines during the COVID-19 outbreak.
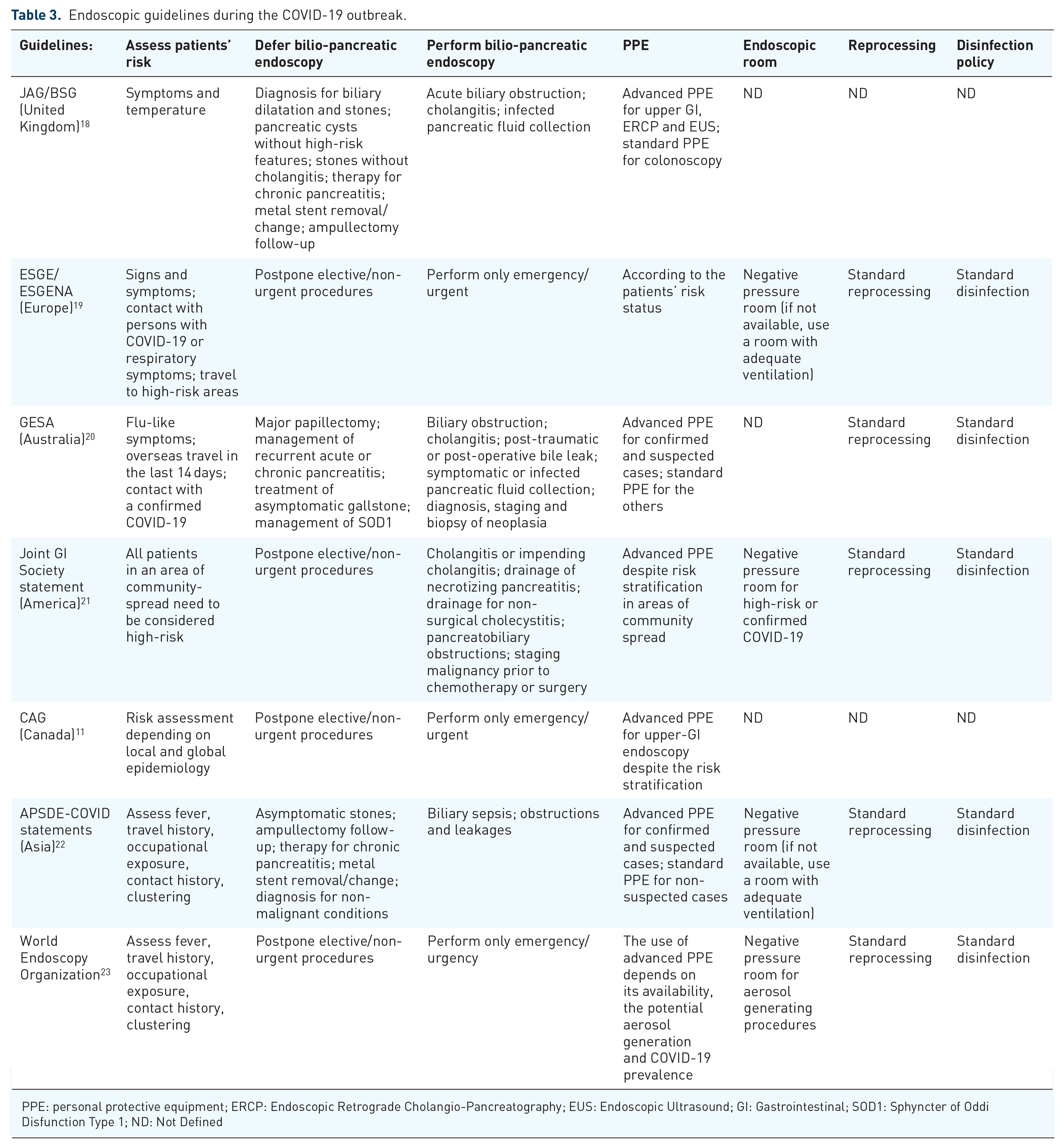
PPE: personal protective equipment; ERCP: Endoscopic Retrograde Cholangio-Pancreatography; EUS: Endoscopic Ultrasound; GI: Gastrointestinal; SOD1: Sphyncter of Oddi Disfunction Type 1; ND: Not Defined
The endoscopy center should keep a record of patients with deferred endoscopy to rearrange the procedures according to the pandemic situation. Moreover, patients should be included in a follow-up program with periodic telephonic interviews for early identification of possible worsening of clinical conditions.
Bilio-pancreatic endoscopy should not be procrastinated in life-threatening conditions. In the case of cholangitis, pancreatobiliary obstruction, post-traumatic or post-operative biliary or pancreatic leaks, cholecystitis non-eligible for surgery and symptomatic or infected pancreatic fluid collections, the morbidity and mortality risks are too high and endoscopy should be carried out with special precautions.
Performing EUS for cancer diagnosis and staging is controversial and a case-by-case decision should be adopted. In general, EUS should be performed if it strongly impacts on therapeutic decision, for example biopsy prior to chemotherapy or surgery, otherwise for diagnosis and surveillance a less invasive technique should be preferred (e.g. magnetic resonance imaging; MRI).
Exceptional cases should be discussed in multidisciplinary teams to find the best health solution for patients, minimizing the risk of SARS-CoV2 transmission.
PPE
To reduce the risk of SARS-CoV2 transmission, the endoscopic unit personnel should receive training in hygiene procedures and proper use of PPE. SARS-CoV2 is an enveloped RNA virus that is rapidly inactivated by ethanol (62–71% concentration), 2% glutaraldehyde and 0.1–0.5% sodium hypoclorite. 24 It has been shown that a proper hand hygiene with soap and water or with hand sanitizer containing 70% alcohol is effective in reducing the risk of enveloped viruses’ transmission.25,26 Proper hand hygiene is strongly recommended and should be performed before and after all endoscopic procedures, direct or indirect contact with patients, contact with potentially contaminated surfaces and when entering or leaving the endoscopic room.
The objective of PPE is to create a barrier between the potential hazardous material and the health-care worker. The use of PPE is mandatory for all the endoscopic unit personnel. The most important international endoscopic societies advise the use of PPE according to risk stratification (Table 3). Considering that the transmission of COVID-19 through asymptomatic carriers via person-to-person contact was observed in many reports27–30 and that bilio-pancreatic endoscopy is a high-risk procedure with potential aerosol generation, we suggest the use of advanced PPE despite the risk stratification.
Advanced PPE includes face mask, double pair of gloves, eye protection (goggles or face shield), hair cover, shoe-covers and isolation gown with water resistance or coverall 31 (Figure 1). Face masks represent the cornerstone of PPE. Several types of face masks are available on the market and they provide different levels of personal protection depending on their design. Standard surgical facemasks create a physical barrier between the mouth and nose of the wearer and the environment, they reduce the spreading of the wearer’s droplets through the environment but those people wearing standard surgical facemasks are at risk for droplet exposure via the lateral, unsealed portions of the face mask. 32 Differently, N95 (FFP2) and N99 (FFP3) respirators provide a filtration of 95% and 99%, respectively, for particles 100–300 nm in size (Coronaviruses’ virion spherical diameter is roughly 125 nm).33–36 All patients and personnel not in close contact with patients should wear surgical masks while staying in the hospital. Personnel should wear N95 or N99 respirator when performing a high-risk procedure such as endoscopy.37,38

The correct personal protection equipment for the endoscopy room in COVID-19 patients.
Endoscopic room management
During the COVID-19 pandemic, the endoscopic room facilities should be revaluated in order to reduce the risk of SARS-CoV2 transmission, maintaining high standards of care. Several gastrointestinal endoscopy societies suggest performing endoscopic procedures in a negative-pressure room (Table 3); when that is not available the procedures can be carried out outside the endoscopic unit (e.g. operation theatre) or in a dedicated room with proper ventilation before and after the procedures. ERCP and EUS should be performed in the same dedicated room to minimize the contamination of the endoscopic unit. In fact, it may be required to perform both ERCP and EUS in the same patient for diagnosis and treatment of bilio-pancreatic diseases. Figure 2 summarizes a proposal of the re-organization of the ‘bilio-pancreatic’ endoscopy room in order to reduce the risk of virus transmission, providing high standards of care. It is essential to create three different spaces inside the room: (a) a clean zone where the personnel wear PPE, this zone is forbidden for patients and for contaminated personnel; (b) a contaminated zone where are located the patient and the personnel during the procedure: this space is considered at high risk of SARS-CoV2 transmission and only the personnel with advanced PPE is allowed to enter; (c) a decontamination zone where the personnel removes PPE when the endoscopic procedure is over. The advantage of this arrangement is to differentiate various levels of security within the endoscopic room, providing a zone where the personnel can wear and remove PPE in a safe environment. On the other side, the disadvantage is that the personnel must follow strict protocols to reduce the risk of mistakes and occult contaminations.

A proposal for the re-organization of the ‘bilio-pancreatic’ endoscopy room during the COVID-19 outbreak.
The endoscopic room staff should be reduced as much as possible to minimize concomitant exposure, preferring the presence of one expert endoscopist, two nurses and one anesthesiologist. The whole endoscopic session should be completed by the same staff.
When the endoscopic procedure is completed, the patient should be referred to a dedicated recovery room. Two different recovery rooms should be set up to separate confirmed or suspected COVID-19 cases from other patients.
To reduce the risk of fomite transmission, a detailed predefined protocol should be followed for disinfection and decontamination of the endoscopic room and all facilities potentially contaminated. Disinfection with ethanol (62–71% concentration), 2% glutaraldehyde and 0.1–0.5% sodium hypochlorite is reported to be effective.24,39 At the end of each procedure an in-depth cleaning process followed by disinfection is mandatory including the floor, furnitures and all surfaces in potential contact with patients or personnel. Since endoscopy can generate aerosol, after the procedure it is suggested to leave the endoscopic room empty for at least 30 min if the procedure is performed in a negative pressure room or to properly ventilate the room for at least 1 h if it is performed in a standard endoscopic room. 40
‘Bilio-pancreatic’ endoscopes and accessories
Differently from standard endoscopes, duodenoscopes and EUS-scopes present a recessed space containing an elevator, elevator cable and channel. This complex design makes them, particularly the duodenoscopes, difficult to clean and makes possible a biofilm formation which protects microorganisms from disinfection and promotes their overgrowth.41,42 In fact, several studies reported the association between duodenoscopes and Pseudomonas aeruginosa, Klebsiella pneumoniae and carbapenem-resistant Enterobacteriaceae infections.43–45 The risk of contamination has been shown also for echoendoscopes, though it is significantly lower in comparison with duodenoscopes.46,47
Recently, duodenoscopes with disposable caps which house the elevator mechanism have been developed: this design might decrease the risk of biofilm formation and might reduce contamination and infection transmission. 48 Moreover, entirely disposable duodenoscopes are nowadays available, giving the opportunity of a single use instrument. This new technology could eliminate the need for reprocessing, and it could potentially eradicate the risk for infectious diseases transmission. 49 During the COVID-19 pandemic the use of disposable duodenoscopes or those with disposable caps could dramatically reduce the risk of patient-to-patient transmission or superinfection in COVID-19 patients and the exposure of personnel during reprocessing. However – in the real world – it would significantly increase the costs 50 and seems not to be affordable in this economic downturn. In fact, the main endoscopy societies suggest a standard reprocessing of endoscopes considering that SARS-CoV2 is an enveloped RNA virus inactivated by commonly used disinfectant24,39 and that the SARS-CoV2 duodenoscope contamination and the role of biofilm in its overgrowth are unknown.
Many accessories are currently used to perform interventional endoscopy such as ERCP or EUS. Accessories can be disposable or reusable after disinfection and reprocessing: after the COVID-19 outbreak, reuse of any device is strongly discouraged and disposable accessories should be preferred.
Discussion
The COVID-19 outbreak dramatically affected the public-health and the health-care facilities organization. In these challenging times, bilio-pancreatic endoscopy needs a wide reorganization to ensure high standards of care minimizing the contamination risks. Several strategies to reduce the virus transmission during bilio-pancreatic endoscopy can be adopted: redefinition of indications for bilio-pancreatic endoscopy, patient’s risk assessment, proper use of PPE, correct use and reprocessing of endoscopes, and reorganization of the endoscopic room.
After the COVID-19 outbreak, the diagnostic process for bilio-pancreatic diseases changed. Generally, when a patient presents signs or symptoms consistent with a bilio-pancreatic disorder, MRI or EUS are the gold standards for a proper diagnosis. Nowadays, hospitals reorganize the radiological services in order to dedicate some radiological facilities only for suspected or confirmed COVID-19 to reduce the risk of patient-to-patient transmission. Most of the hospitals cannot afford the use of a MRI machine only for COVID-19 patients, so its use should be reduced to essentials. The majority of patients with suspected or confirmed COVID-19 disease undergo a chest-CT-scan to verify the presence of lung injuries. Given that a CT-scan machine is already reserved for suspected or confirmed COVID-19 cases, we suggest that it could be used for a first evaluation in patients with suspicion of bilio-pancreatic disorders. Moreover, we suggest the endoscopic units set up a hybrid room for performing both ERCP and EUS, so when a patient with a bilio-pancreatic disease has not a clear diagnosis, EUS can be used as the diagnostic technique, followed by ECRP for the interventional procedure. Having a hybrid room could reduce the risk of contamination of the endoscopic unit facilities and the number of personnel exposed.
There is agreement between various guidelines (Table 3) in performing only emergency/urgent endoscopy and deferring the elective and not urgent procedures. In some clinical scenarios, the definition of urgency is not always clear. In fact, when deferring an endoscopic procedure, the risk for medium-time morbidity and mortality should be evaluated. For example, an asymptomatic patient with suspicion for pancreatic cancer is not at risk of life in the short-term and the endoscopic evaluation could be ideally postponed; obviously, in the lack of histologic diagnosis, it would exclude the patient from a therapeutic approach and it would dramatically affect the patient’s health outcomes. In this setting, even though the patient is not at imminent risk of life, the bilio-pancreatic endoscopy should be performed, considering the high medium-term morbidity and mortality risk.
Bilio-pancreatic endoscopy is often tightly linked to bilio-pancreatic surgery (e.g. in pancreatic cancer). Since the COVID-19 outbreak the reduction of operating rooms available and the long waiting list for surgery can change the indication for endoscopy: for example, a patient with pancreatic cancer eligible for surgery without cholangitis or incoercible pruritus is generally referred directly to surgery. At these times, since the surgery could be significantly delayed, a preoperative endoscopic drainage is indicated while waiting for surgery.
A multidisciplinary team should be arranged to discuss all exceptional and controversial cases, aiming to take the best decision for patients.
The endoscopic unit has the role to follow strictly its patients to avoid sudden changing of their health conditions. On one hand, those deferred patients should be scheduled for a new appointment as soon as possible and they should be included in a follow-up program for early identification of worsening of their diseases; on the other hand, patients that underwent an endoscopic procedure during the COVID-19 pandemic should be considered at risk for SARS-CoV2 infection and their clinical conditions should be checked at 7 and 14 days from the procedure to exclude signs and symptoms consistent with COVID-19.
In conclusion, the COVID-19 outbreak strongly influenced our clinical practice. Acute bilio-pancreatic diseases are burdened by high mortality and morbidity and endoscopy is often not deferrable for their management. At these challenging times, it is crucial to clarify the proper indications for ERCP and therapeutic EUS, the re-organization of the endoscopic unit and the correct use of PPE in order to guarantee appropriate treatments and health-care provider safety.