
Abstract
Background:
It is challenging to identify the prevalence of lymph node metastasis (LNM) and residual tumor in patients with early gastric cancer (EGC) who underwent noncurative endoscopic resection (ER). This present meta-analysis was aimed to establish imperative potential predictive factors in order to select the optimal treatment method.
Methods:
A systematic literature search of PubMed, Embase, and Cochrane Library databases was performed through 1 February 2019 to identify relevant studies, which investigated risk factors for LNM and residual tumor in patients with EGC who underwent noncurative ER. Eligible data were systematically reviewed through a meta-analysis.
Results:
Overall, 12 studies investigating the risk factor of LNM were included, totaling 3015 patients, 7 of which also involved cancer residues. After the present meta-analysis, six predictors, including tumor size >30 mm, tumor invasion depth (⩾500 μm from the muscularis mucosae), macroscopic appearance, undifferentiated histopathological type, positive vertical margin, and presence of lymphovascular invasion (including lymphatic invasion and vascular invasion) were significantly associated with LNM, whereas tumor size >30 mm, positive horizontal margin, and positive vertical margin were identified as significant predictors for the risk of residual tumor. No evidence of publication bias was observed.
Conclusions:
Six and three variables were established as significant risk factors for LNM and residual tumor in patients with EGC who underwent noncurative ER, respectively. Patients with EGC who present these risk factors after noncurative ER are strongly suggested to receive additional surgery, while others might be suitable for strict follow-up. This might shed some new light on the selection of follow-up treatment for noncurative ER.
Keywords
Introduction
Gastric cancer has become the third most common cause of cancer death worldwide. 1 The National Central Cancer Registry of China identified gastric cancer, following lung cancer, as the second most incident cancer and leading cause of cancer mortality. 2 Early gastric cancer (EGC) is commonly defined when the depth of tumor invasion is confined to the mucosa or submucosa, regardless of lymph node metastasis (LNM). 3 EGC has been increasingly detected in Asia, especially in Japan, mainly attributed to a nationwide screening program and novel endoscopic technologies and equipment. 4 In addition to conventional radical gastrectomy, endoscopic resection (ER), including endoscopic mucosal resection (EMR) and endoscopic submucosal dissection (ESD), has become an effective treatment for EGC that intends to perform an en bloc resection and precise histopathological assessment of the lesion with the advantages of being less invasive and more economical.4–6
Based on the common recognition of the prevalence of LNM and residual tumor being the significant prognostic factor for patients with EGC,7,8 curability of ER for EGC has been classified into three groups: curative resection, expanded-indication curative resection, and noncurative resection, with additional surgical treatment being indicated for noncurative resection.9,10 However, as LNM is present in only 5–13% of patients who underwent noncurative ER,11–13 standard radical surgery might be overaggressive. Data on establishing risk factors for prevalence of LNM and residual tumor in patients with EGC who underwent noncurative endoscopic treatments is currently insufficient. This present article conducted a meta-analysis of risk factors for LNM and residual tumor in patients with noncurative ER in order to determine the certain patient population requiring additional gastrectomy, which might shed new light on the current definition of noncurative ER.
Methods
This systematic review was performed in accordance with the methodology proposed by the Meta-analysis Of Observational Studies in Epidemiology group 14 and the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement. 15
Search strategy
An online systematic literature search of PubMed, Embase, and Cochrane Library databases was conducted, using the following keywords: “early gastric cancer” AND (“endoscopic resection” OR “ER” OR “endoscopic submucosal dissection” OR “ESD” OR “endoscopic mucosal resection” OR “EMR”) AND (“gastrectomy” OR “surgery” OR “gastric resection”) AND (“lymph node metastasis” OR “lymph node involvement” OR “lymphatic metastasis” OR “lymphatic involvement”), from inception through 1 February 2019. Free-text and MeSH searches were performed as appropriate. In addition, manual search of the reference lists from available studies was conducted for potential articles. Two researchers implemented the selection process independently, and the divergences were resolved through discussion.
Eligibility criteria for study selection
Studies were deemed eligible according to the PICO approach.
P: Patients diagnosed with EGC and who underwent noncurative ER.
I: Additional surgery after noncurative ER with available data on LNM and residual tumor.
C: Comparison of patient subgroups with various potential risk factors related to LNM and residual tumor.
O: LNM and residual tumor.
The inclusion criteria for eligible studies were as follows: (1) study design (randomized controlled trial, cohort, or case–control); (2) articles published in English; (3) patients underwent noncurative ER for EGC, with noncurative resection defined by the Japanese gastric cancer treatment guidelines 2010 (version 3); 9 (4) patients underwent additional gastrectomy after noncurative ER; (5) adequate information about risk factors for LNM and residual tumor, with available data for extraction to calculate the pooled odds ratio (OR) or mean difference (MD). When dual (or multiple) studies were reported by the same authors and/or institution, study of higher quality or the most recent publication was included in the analysis. In addition, abstracts, case reports, reviews, letters to editor, editorials, expert opinions, conference abstracts, or meeting proceedings were excluded.
Data abstraction and quality assessment
Two researchers reviewed the title and abstract of each article searched independently. Full-text versions of the original articles were acquired and required information was prudently extracted in a standardized manner. A third researcher was asked to audit the study in case of any discrepancies. The following information was collected: first author, publication year, country of publication, data collection period, study design, number of patients, baseline and clinicopathological characteristics of patients, risk factors of LNM and residual tumor, relevant OR, MD, and 95% confidence interval (CI) (or provide sufficient data for calculation).
Two researchers independently evaluated the quality of the eligible studies using the modified Newcastle–Ottawa Quality Assessment Scales (NOS). 16 Quality categories were defined as high quality (score 7–9), medium quality (score 4–6) and low quality (score 0–3).
Statistics
Sensitivity analyses were performed using Review Manager version 5.3 to calculate the pooled OR with a 95% CI for dichotomous variables, and the MD with a 95% CI for continuous variables, which were reexamined by Stata version 15.0. Heterogeneity among included studies was measured using a Q test and I2 statistic. When the p value of Q test >0.1 and I2 < 50% indicated no evident heterogeneity, a fixed-effects model was used; otherwise, a random-effects model was carried out. A p value <0.05 was considered a statistically significant difference. Publication bias was evaluated with a funnel plot via Review Manager version 5.3, and Begg’s and Egger’s tests via Stata version 15.0.
Results
Eligible studies and study characteristics
The searching strategy initially identified 593 potentially relevant articles via PubMed (n = 211), Embase (n = 367), and Cochrane Library databases (n = 15), of which 173 studies were excluded for duplication. After scanning the titles and abstracts of the remaining articles, a total of 388 studies were excluded, owing to irrelevance and inaccurate article types, which leaves 32 studies for full-text evaluation. Among the remaining studies, 2 papers were excluded for study population overlap; 10 were removed due to inadequate data; 8 were removed for enrolled patients’ inconformity of noncurative ER criteria; eventually, 12 papers met the inclusion criteria and were subjected to further meta-analysis (Figure 1).11–13,17–25

Flow chart of study selection for the meta-analysis.
The baseline characteristics of the 12 studies included in the meta-analysis are presented (Table 1). All studies were performed in East Asian countries, including eight in Japan and four in South Korea, which enrolled a total number of 3015 patients. All the included studies were retrospective observational studies, which enrolled patients with EGC who underwent additional surgery after noncurative ESD or EMR, with the indications of noncurative resection following the Japanese gastric cancer treatment guidelines 2010 (version 3). 9 All the 12 observational studies reported the risk factors for postoperative pathological diagnosed LNM, and 7 of them also investigated risk factors for residual tumor as the outcome.13,19,21–25 Among the enrolled 12 studies, LNM was reported in 247 patients (8.2%), whereas residual tumor was presented in 141 patients (13.5%) from the 7 included studies. In terms of the NOS quality assessment, all the included studies were graded as high quality (score 7–9).
Characteristics of included articles studying risk factors for LNM and residual tumor in patients who underwent noncurative ER.

LNM, lymph node metastasis; EGC, early gastric cancer; ER, endoscopic resection; ESD, endoscopic submucosal dissection; NA, not available.
Risk factors for LNM
Tumor size
The relationship between tumor size and prevalence of LNM was evaluated in eight studies, of which six studies using the cutoff value of 30 mm. For the cutoff value of 30 mm subgroup, a fixed-effects model was used to assess the data (p = 0.96, I2 = 0%). The pooled analysis elucidated that the risk of LNM was significantly higher in patients with tumor size >30 mm than that of ⩽30 mm (pooled OR = 1.63, 95% CI = 1.20–2.22, p = 0.002) (Figure 2). In contrast, no statistical significance of a cutoff value of 20 mm was revealed (pooled OR = 1.15, 95% CI = 0.36–3.69, p = 0.82) through a fixed-effects model (p = 0.33, I2 = 0%).
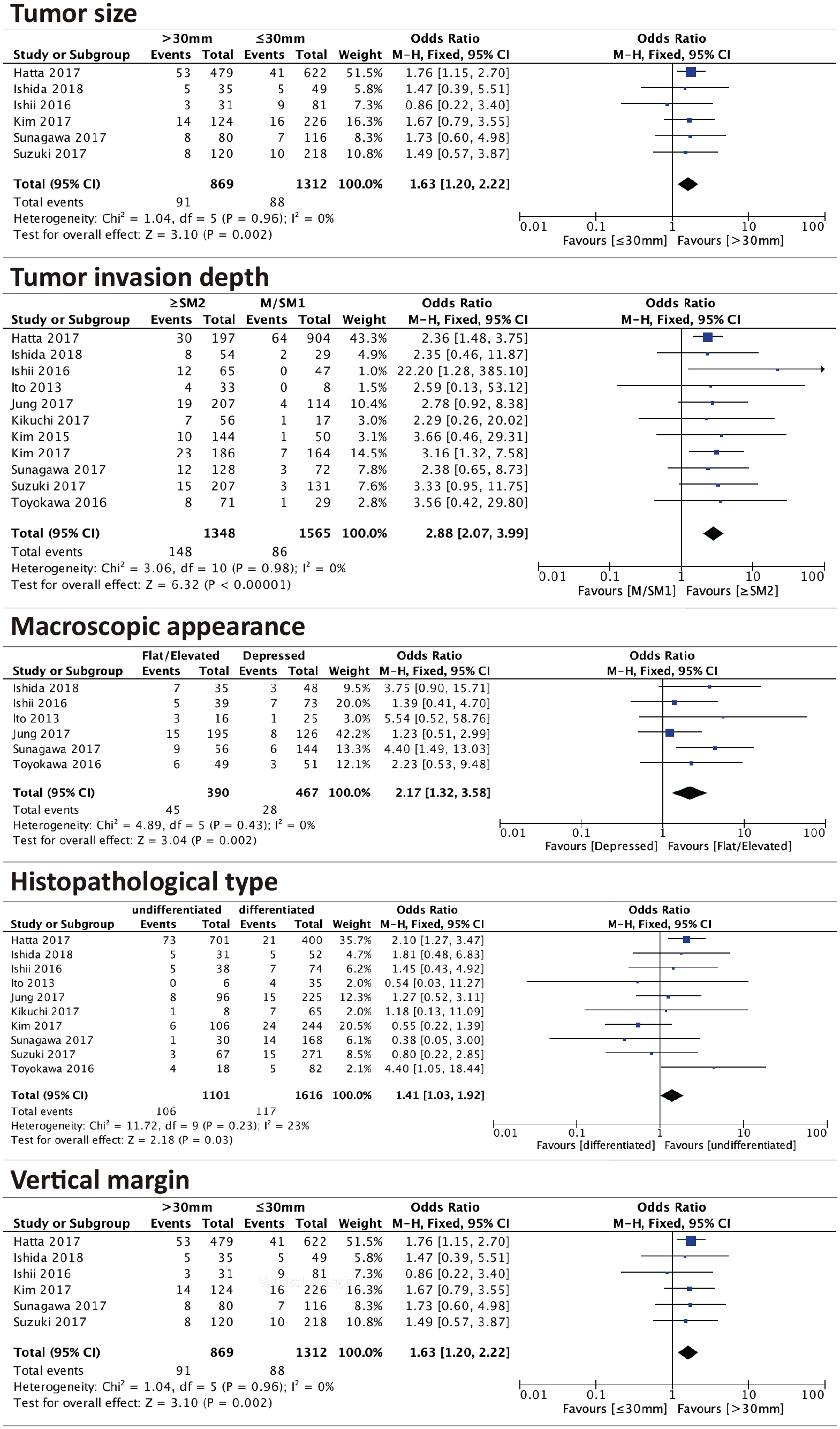
Forest plot for the relationship between LNM and tumor size, tumor invasion depth, macroscopic appearance, histopathological type and vertical margin, respectively.
Tumor invasion depth
The influence of tumor invasion depth on the risk of LNM was reported in 11 studies. Based on no statistically significant heterogeneity (p = 0.98, I2 = 0%), a fixed-effects model was applied to analyze the data. This pooled analysis suggested that patients with tumor invasion depth ⩾ SM2 (⩾500 μm from the muscularis mucosae) had significantly higher prevalence of LNM than patients with tumor invasion depth < SM2 (pooled OR = 2.88, 95% CI = 2.07–3.99, p < 0.00001) (Figure 2).
Macroscopic appearance
Six studies investigated the relationship between the prevalence of LNM and tumor macroscopic appearance. A fixed-effects model was adopted to analyze data for no statistically significant heterogeneity among studies (p = 0.43, I2 = 0%). This pooled analysis suggested that patients with flat or elevated tumor macroscopic appearance had significantly higher risk of LNM than patients with depressed tumor macroscopic appearance (pooled OR = 2.17, 95% CI = 1.32–3.58, p = 0.002) (Figure 2).
Histopathological type
Ten studies investigated the relationship between risk of LNM and tumor histopathological type. No statistically significant heterogeneity was detected (p = 0.23, I2 = 23%), and a fixed-effects model was applied to assess the data. The pooled analysis revealed that the prevalence of LNM was significantly higher in patients with histologically undifferentiated type than that of differentiated type (pooled OR = 1.41, 95% CI = 1.03–1.92, p = 0.03) (Figure 2).
Vertical margin
There were 10 studies that assessed the relationship between the risk of LNM and resection vertical margin. A fixed-effects model was applied to analyze data due to no statistically significant heterogeneity (p = 0.40, I2 = 4%). Findings from this pooled analysis revealed that the prevalence of LNM was significantly higher in patients with positive vertical margin than in patients with negative vertical margin (pooled OR = 2.02, 95% CI = 1.50–2.73, p < 0.00001) (Figure 2).
Lymphovascular invasion
There were four, seven, and six studies that reported the influence of tumor lymphovascular invasion (LVI), lymphatic invasion (LI), and vascular invasion (VI) on the risk of LNM, respectively. For the four studies providing data of lymphovascular invasion, a random-effects model was applied to analyze data for significant heterogeneity (p = 0.06, I2 = 59%). This pooled analysis revealed that patients with tumor lymphovascular invasion had significantly higher risk of LNM than patients without tumor lymphovascular invasion (pooled OR = 3.46, 95% CI = 1.35–8.87, p = 0.01) (Figure 3).

Forest plot for the relationship between LNM and lymphovascular invasion, lymphatic invasion, and vascular invasion, respectively.
For the LI subgroup, a fixed-effects model was used due to nonsignificant heterogeneity (p = 0.59, I2 = 0%). Results showed that patients with tumor LI had a statistically significant higher risk of LNM than patients without tumor LI (pooled OR = 5.60, 95% CI = 3.85–8.14, p < 0.00001) (Figure 3). Similarly for the vascular invasion subgroup, a statistically significant association was revealed between the prevalence of LNM and tumor vascular invasion (pooled OR = 2.42, 95% CI = 1.69–3.46, p < 0.00001) through a fixed-effects model (p = 0.59, I2 = 0%) (Figure 3).
Nonsignificant risk factors
In the present meta-analysis of the risk factors for the prevalence of LNM after noncurative ER, patient’s age over 70 years (pooled OR = 0.92, 95% CI = 0.48–1.78, p = 0.81), age (MD = −0.52, 95% CI = −5.71–4.67, p = 0.84), sex (pooled OR = 0.70, 95% CI = 0.44–1.12, p = 0.14), ulcerative findings (pooled OR = 0.85, 95% CI = 0.58–1.23, p = 0.39), tumor location (pooled OR = 1.03, 95% CI = 0.66–1.62, p = 0.88), tumor positive horizontal margin (pooled OR = 0.69, 95% CI = 0.39–1.23, p = 0.21), treatment options between EMR and ESD (pooled OR = 0.91, 95% CI = 0.26–3.15, p = 0.88) were revealed as nonsignificant risk factors (Table 2; Supplemental Figures 1 to 8).
Meta-analysis identified risk factors for LNM in patients with EGC who underwent noncurative ER.

Mean difference (95% CI).
CI, confidence interval; EGC, early gastric cancer; LNM, lymph node metastasis; ER, endoscopic resection; MD, mean difference; OR, odds ratio; SM2, invasion depth of 500 μm from the muscularis mucosae.
Risk factors for residual tumor
Tumor size
The relationship between tumor size and prevalence of residual tumor was evaluated in three studies, which applied the tumor size with 30 mm as a cutoff value. A fixed-effects model was used to assess the data (p = 0.55, I2 = 0%). The pooled analysis exhibited that the risk of residual tumor was significantly higher in patients with tumor size ⩾30 mm than in patients with tumor size <30 mm (pooled OR = 2.89, 95% CI = 1.89–4.43, p < 0.00001) (Figure 4).

Forrest plot for the relationship between residual tumor and tumor size, horizontal margin, and vertical margin, respectively.
Horizontal margin
The influence of ER horizontal margin on the risk of residual tumor was investigated in six studies. Based on nonsignificant heterogeneity (p = 0.60, I2 = 0%), a fixed-effects model was applied to analyze data. Findings from this meta-analysis suggested a significant difference for the prevalence of residual tumor between patients with positive horizontal margin and patients with negative horizontal margin (pooled OR = 12.70, 95% CI = 8.20–19.66, p < 0.00001) (Figure 4).
Vertical margin
Six studies assessed the relationship of the risk of residual tumor and the resection vertical margin. A random-effects model was applied to analyze data due to statistically significant heterogeneity (p = 0.05, I2 = 54%). Results from this meta-analysis revealed that the prevalence of residual tumor was significantly higher in patients with positive vertical margin than in patients with negative vertical margin (pooled OR = 2.37, 95% CI = 1.14–4.92, p = 0.02) (Figure 4).
Nonsignificant risk factors
In the present meta-analysis of the risk factors for residual cancer cells in the remnant stomach after noncurative ER, patient’s age over 70 years (pooled OR = 1.52, 95% CI = 0.67–3.43, p = 0.32), sex (pooled OR = 0.75, 95% CI = 0.28–2.03, p = 0.57), histopathological type (pooled OR = 1.30, 95% CI = 0.85–1.97, p = 0.22), tumor invasion depth of SM2 or deeper (pooled OR = 0.67, 95% CI = 0.23–1.92, p = 0.46), ulcerative findings (pooled OR = 1.12, 95% CI = 0.62–2.01, p = 0.72), macroscopic appearance (pooled OR = 1.20, 95% CI = 0.63–2.28, p = 0.57), tumor LVI (pooled OR = 0.55, 95% CI = 0.11–2.68, p = 0.46), LI (pooled OR = 1.31, 95% CI = 0.71–2.40, p = 0.39), and VI (pooled OR = 1.51, 95% CI = 0.79–2.89, p = 0.21) were revealed as nonsignificant risk factors (Table 3; Supplemental Figures 9 to 17).
Meta-analysis identified risk factors for residual tumor in patients with EGC who underwent noncurative ER.

CI, confidence interval; EGC, early gastric cancer; ER, endoscopic resection; OR, odds ratio; SM2, invasion depth of 500 μm from the muscularis mucosae.
Publication bias
Funnel plot, Begg’s test, and Egger’s test were applied to evaluate the possibility of publication bias for each risk factors via Review Manager version 5.3 and Stata version 15.0 (Tables 2 and 3). No substantial publication bias was identified in all pooled analyses (p > 0.05).
Discussion
The diagnosis of EGC is generally made when the depth of tumor invasion is confined to the mucosa or submucosa, irrespective of lymph node status, 3 which was adopted by the Japanese Gastric Cancer Association in the 1998 edition 26 and remains the accepted definition to this day. 27 However, the prevalence of LNM and residual tumor has been generally consented as the significant prognostic factor for patients with EGC.7,8 The attempt to update the definition of EGC has been carried out in order to improve the ability to determine the risk factors for the prevalence of LNM and residual tumor. 28
Even though the advent of endoscopic ultrasound (EUS) and EUS-guided fine-needle aspiration intended to advance preoperative lymph node staging of early cancer, 29 the accuracy of detection from several studies’ data appeared to be unpromising,30,31 which leaves them out of the staging algorithm of presumed EGC. In addition, the identification efficacy of 18F-fluorodeoxy-glucose positron emission tomography and 18F-deoxyfluorothymidine positron emission tomography has also turned out to be unsatisfied due to relative high false negative rate related to tumor differentiation.32–34 Since ER, including EMR and ESD, became one of the main methods for treating EGC, capable of performing a precise histopathological staging after an en bloc resection of the lesion,4–6,35,36 the Japanese Gastric Cancer Association (JGCA) and the Japan Gastroenterological Endoscopy Society has classified the curability of ER into three potential groups. The lesion meeting none of the absolute or expanded indications is considered as noncurative resection.9,10 Surgical treatment is recommended in the patients with EGC who underwent noncurative resection, due to potential risk of LNM and cancer residue.7–9 Nevertheless, approximately 8.2% and 13.5% of patients with EGC who underwent noncurative ER presented with LNM and residual tumor, respectively.11–13,17–25,37 Thus, the potential risk of developing recurrence needs to be weighed against surgical trauma. 38 Latent risk factors for the prevalence of LNM and residual tumor in patients with EGC who underwent noncurative endoscopic treatments are imperative to be assessed and established. Therefore, a meta-analysis of 12 relative studies has been carried out.
In the present meta-anlaysis, tumor size with a cutoff value of 30 mm was identified as a significant predictor for both LNM (p = 0.002) and residual tumor (p < 0.00001). In fact, Maehara et al. suggested that tumor size was a reliable predictor in inspecting the tumor behavior of EGC, 39 while Saito et al. asserted that tumor size serves as a predictor of survival in patients with gastric cancer. 40 Regarding the depth of tumor invasion, our pooled analysis elucidated that patients with tumor invasion depth ⩾ SM2 had significantly higher prevalence of LNM (p < 0.00001). One of the reasons might be attributed to the lymphatic drainage of the gastric wall. Listrom et al. revealed that the gastric lymphatics normally develop as a plexus of vessels near the muscularis mucosae, while the upper two-thirds of the gastric lamina propria is normally devoid of lymphatics, irrespective of gastric location and tissue pathohistology. 41 Park et al. reported a LNM rate of M, SM1, and SM2/3, with 3.4%, 0%, and 30%, repectively, 42 while Hölscher et al. reported a LNM rate of 40% for SM2. 43 In addition, a previous study elucidated that an undifferentiated component in submucosal invasion was an independent predictor for LNM. 44 Although Ishigami et al. revealed that there was no evident asscociation between tumor size and the depth of submucosal infiltration (p = 0.1), both submucosal layer invasion and horizontal tumor expansion were significantly correlated with LNM (p < 0.05). 45
For the assessment of the impact of macroscopic appearance on LNM, Sunagawa et al. elucidated that the difference for the prevalence of LNM between patients with flat or elevated tumor macroscopic type and patients with depressed tumor macroscopic type was found statistically significant not only in univariate analysis (p = 0.004), but in multivariate analysis as well (p = 0.011), 24 which is consistent with the result of our present pooled analysis (p = 0.002). It is currently unclear why the flat or elevated type was associated with LNM, although several studies have reported similar results. Jung et al. presumed that there might be difficulties to estimate the invasion depth during diagnostic endoscopy in EGC cases with the elevated type tumor. 46 Sekiguchi et al. reported that patients with EGC with a papillary adenocarcinoma component were more likely suggestive of lymphatic invasion and showed a higher risk of positive LNM. 47 In fact, in the Sunagawa et al. study, a papillary adenocarcinoma component was found more frequently in patients with a flat or elevated type (19.6%) than in patients with a depressed type (6.9%) (p = 0.012). Nevertheless, Baba et al. illustrated a low prevalence of LNM associated with lesions of elevated types of I and IIa, and the flat type of IIb, whereas macroscopic types consisting of depressed portion such as IIc and III were more susceptible to perigastric and extra-perigastric lymph node involvement. 48 Further investigations have to be implemented to determine the genuine relationship between macroscopic appearance of EGC and LNM.
In terms of tumor histopathological type, our pooled analysis revealed that the prevalence of LNM was significantly higher in patients with histologically undifferentiated type (p = 0.03), despite 8 of the 10 eligible studies involved yielding no statistical significance between the two subgroups. The discrepancies might be ascribed to the relatively small sample size of each study, which undermined the statistical power and disqualified the final results. In fact, Miyahara et al. reported that an undifferentiated component in submucosal invasion was the independent predictor for LNM, and the incidence of LNM increased significantly for a predominant undifferentiated type (p = 0.005) and undifferentiated component (p < 0.001) in submucosal invasion as the deeper the tumor invading into submucosa. 44
In this meta-analysis, LVI, LI, and VI were identified as the significant risk factor of LNM, which was consistent with the previous study with LVI being the strongest predictor for LNM (OR = 21.41). 49 Among our included studies, Toyokawa et al., Kikuchi et al., and Sunagawa et al. reported the highest OR for LVI (OR = 10.20), LI (OR = 18.62), and VI (OR = 4.01), respectively.21,24,25 A LNM rate of 56.8% was revealed in patients with LVI submucosal EGC. 50 A multivariate analysis conducted by Nasu et al. suggested that LVI was the only significant predictor of LNM in patients with undifferentiated EGC (OR 7.4, 95% CI = 2.9–19.0). 51 In addition, Dicken et al. identified LVI as an independent risk factor of survival in gastric cancer, with a 5-year survival of 13.9% in patients presenting with LVI. 52
Positive vertical margin of EGC was revealed as a significant predictor of LNM, whereas none of the eight included studies suggested a significant association between LNM and tumor horizontal margin, which might be explained by the location depth of lymphatic vessels. 41 Nevertheless, both positive horizontal margin and vertical margin were identified as the evident risk factor of cancer residue in this present meta-analysis. In fact, positive horizontal margin was revealed as an evident predictor for residual tumor in all of the six eligible studies. Hwang et al. established a scoring system based on number of involved directions, rate and total length of lateral resection margin involvement, which showed 100% sensitivity and 49% specificity for residual or recurrent tumors. 53 Interestingly, Noh et al. suggested that close surveillance might be a feasible strategy for patients with EGC who present positive vertical margin without LVI or deep submucosa invasion, especially for whom surgery might be risky. 54
A scoring system, named as eCura, was established to categorize patients into three risk groups in order to address the risk of LNM in Japan. In its validation stage, noncurative ESD followed by additional surgery was recommended for patients in the high LNM risk group, whose 5-year cancer-specific survival appeared to be 90.1%. 17 Furthermore, after bringing the Hatta et al. study above into the eligible studies for our meta-analysis, two novel additional predictors emerged, which were histopathological type and macroscopic appearance. That is, patients with EGC whose pathology results after noncurative ER present histologically undifferentiated type or flat or elevated tumor macroscopic appearance should also be recommended with additional surgery in case of LNM. In fact, the eCura scoring system did not take the residual tumor after ESD into consideration. Although ESD has a burning effect that sometimes leads to no remnant cancer after ESD even if there is a positive lateral margin, the risk of cancer residue should still be under vigilance when R0 resection is not achieved. For this reason, our pooled analysis also investigated the potential predictors for residual tumor, which identified positive horizontal margin as a significant risk factor apart from the indicators mentioned above. Therefore, patients meeting the noncurative resection criteria solely for the presence of ulcerative findings might avoid excessive additional surgery.
In the cases that patients with EGC who have undergone noncurative ER and appear to harbor the risk factors indicated in this present meta-analysis, additional surgical treatment should be strongly recommended. Yamanouchi et al. reported that the incidence of hypertension was significantly higher in the follow-up group compared with the additional surgery group (51.0% versus 25.9%; p = 0.03). 55 The Li et al. meta-analysis, which enrolled 4225 patients, revealed that additional surgery significantly provided better 5-year overall survival (pooled OR = 3.50, 95% CI = 2.89–4.24, p < 0.001) and disease-specific survival (pooled OR = 3.99, 95% CI = 2.50–6.36, p < 0.001) than observation. 56 In terms of surgical method, Katsube et al. reported that 15 patients underwent additional surgery with lymphadectomy (D1+) (laparoscopy-assisted distal gastrectomy, n = 7; distal gastrectomy, n = 2; total gastrectomy; and proximal gastrectomy, n = 2) and 2 patients underwent local resection. The 5-year survival rate was 93% and no gastric cancer-specific death was documented, which might substantially shed light on the possiblity of a less radical procedure. 57 As regards the specific surgical methods and the scope of lymph node dissection of additional gastrectomy after noncurative ER, no particular prospective study has been designed to investigate the difference of therapeutic effect, complication and prognosis among various surgical procedures after noncurative resection. 58 In addition, overall survival in patients who underwent additional surgery after noncurative ESD was significantly higher in the nonelderly (<70 years) and elderly groups (70–79 years) (p < 0.001), whereas the difference was not significant in patients ⩾80 years (p = 0.23). 59 Therefore, elderly patients with high risk of LNM and high performance status should undergo additional surgery, and establishment of criteria for selecting treatment methods after noncurative ESD in elderly patients is required. In fact, regarding patients with impaired physical conditions or no personal consent for additional surgery, sentinel lymph node biopsy with subserosal or submucosal injection of blue dye or radioactive tracer might serve as a further promising strategy for detection of lymph node involvement, with an accuracy rate range from 75% to 100%60–63 due to various lymphatic drainage of the gastric region. In addition, repeated ESD, endoscopic coagulation, and close observation are also recommended by JGCA as alternatives for this patient population. 9 Together, the combination of the risk factor for LNM and cancer residue and sentinel lymph node biopsy might advance the detection of lymph node status and prediction of cancer recurrence. These findings might alter the definition of noncurative ER to some extent, especially when patients habouring these nonsignificant predictors might avoid radical additional surgery.
Conclusion
The available results from the present meta-analysis exhibited that tumor size >30 mm, tumor invasion depth ⩾ SM2, macroscopic appearance, undifferentiated histopathological type, positive vertical margin, and LVI (including LI and VI) were statistically significant risk factor for the prevalence of LNM. Meanwhile tumor size >30 mm, positive horizontal margin, and positive vertical margin were identified as significant predictors for residual tumor. All of the 12 included studies were conducted in Japan or South Korea, which might neglect the impact of ethnicity. Prospective cohort study is essential to be conducted in order to construct an optimal combined predictive model for the prevalence of LNM and residual tumor in patients with EGC who underwent noncurative ER, which might allow surgeons to identify the population that would benefit the most from strict follow-up or additional surgery.
Supplemental Material
supplemental_figures – Supplemental material for Predictors of lymph node metastasis and residual tumor in early gastric cancer patients after noncurative endoscopic resection: a systematic review and meta-analysis
Supplemental material, supplemental_figures for Predictors of lymph node metastasis and residual tumor in early gastric cancer patients after noncurative endoscopic resection: a systematic review and meta-analysis by Bolun Jiang, Li Zhou, Jun Lu, Yizhi Wang and Junchao Guo in Therapeutic Advances in Gastroenterology
Footnotes
Acknowledgements
Our deepest gratitude goes to the Managing Editor, Alessandro Baliani, the Associate Editor, Robert Benamouzig, the Peer Review Supervisor, Kanika Kamboj, and the reviewers for their careful work and thoughtful suggestions that have helped improve this paper substantially.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article. The present study was supported by the National Natural Science Foundation of China (grant number 81972324), the China Academy of Medical Sciences Innovation Fund for Medical Sciences (grant number 2016-I2M-3-019).
Conflict of interest statement
The authors declare that there is no conflict of interest.
Ethics approval statement
Ethics approval was not required for this study.
Informed consent statement
Informed consent was not required for this study.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.