
Abstract
Despite significant advances in medical therapy in the management of Crohn’s disease (CD), surgery is still required in a significant proportion of patients and constitutes an important tool in treatment algorithms. Recently, more options of biological agents have been made available, and most patients with CD undergoing surgical procedures have been previously exposed to this class of drugs. There is controversy in the literature as to whether anti-tumor necrosis factor (TNF) agents, anti-integrins, or anti-interleukins (ILs) have a direct relationship with increased postoperative complications.
In this narrative review, the authors summarize the most important data regarding the effect of biologics on postoperative outcomes in CD.
Most studies (with different designs) are based on the experience with anti-TNF agents, mostly with infliximab. Some studies outlined the relationship between vedolizumab and postoperative complications, and there is a lack of data with ustekinumab in this scenario. Most studies are retrospective, but few prospective data are available. A cause–effect (proof of concept) direct relationship between biologics and an increase in postoperative morbidity has not been demonstrated to date. Several confounding factors such as previous use of steroids, malnutrition, and unfavorable abdominal conditions have a definitely effect on postoperative complications in CD.
Biologics seem safe to be used in the perioperative period, but available data are still controversial. Multidisciplinary individualized decisions should be made on a case-to-case basis, adapting the surgical strategy according to risk factors involved.
Keywords
Introduction
The development of biological agents from different classes over the last two decades was a landmark in the management of Crohn’s disease (CD).1–4 These agents can induce and maintain clinical remission, heal the mucosa, and change the natural course of the disease, if used in a timely fashion, avoiding disease progression towards stenosis and fistula formation. 5 In the biological era, surgical rates have decreased over time. 6 However, even with the remarkable improvement in therapeutic algorithms, surgery is still required in a significant proportion of patients with CD. 7
Most patients with surgical indication in the management of CD in the 21st century have been previously exposed or are currently being treated with biological agents. 7 Systemic immune suppression can theoretically affect postoperative outcomes. As an example, tumor necrosis factor (TNF)-α has an important role in angiogenesis, collagenous synthesis, and anastomotic or wound healing. 8 Thus, TNF inhibition could be implicated in an increase in infectious and/or surgical complications after a surgical procedure. 9 This leads to controversy if patients previously exposed to anti-TNF agents or other biologics need to stop therapy before surgery. Several studies have been published with agents with different mechanisms of action, and significant controversy in this field is described.
Postoperative complication rates are greater in patients with CD in comparison with other benign or malignant diseases in colorectal surgery. 10 Confounding factors such as previous use of steroids, malnutrition, as well as the severity of the disease at the moment of surgery have a definite effect on postoperative outcomes.7,11 This increase in complication rates in CD probably has to be observed in a broader scenario, where the use of biologics is a coincidental factor of more severe patients and exhaustive medical therapy. The delay in surgical indication due to a broad panel of medical therapeutic options also contributes to significant postoperative complications in CD. 12
Several previous publications have demonstrated the controversy over the relationship between biological agents and postoperative outcomes in CD surgery.13–15 Most of these studies are retrospective case series16–19 and some meta-analyses have also been published.20–23 Few prospective studies have been performed.24–27 To date, a direct cause–effect relationship between previous use of biologics and an increase in complication rates has never been demonstrated, and there is no consensus as to whether biologics affect postoperative outcomes.
The aim of this narrative review was to describe in detail the main studies regarding the relationship between preoperative use of biologics and postoperative complications after abdominal surgery in CD. Data on anti-TNF agents, vedolizumab and ustekinumab are summarized, and possible reasons for this important controversy are discussed.
Anti-TNF therapy
TNF-α is an important pro-inflammatory cytokine involved in the pathogenesis of CD. 8 Its inhibition leads to apoptosis of inflammatory cells, making anti-TNF agents an important therapy for immune-mediated diseases. There are three different anti-TNF agents approved for the management of CD: infliximab (IFX), adalimumab (ADA), and certolizumab pegol (CER). The studies with anti-TNFs comprise most of the available data in the literature, regarding the relationship between biological agents and postoperative outcomes. IFX is the most frequently studied agent in this field. Few data exclusively based on ADA have been published, 28 and some studies included two or more agents in the same database, suggesting a class effect. 16 In this section, we focus on multiple methods used in different studies (retrospective, meta-analysis or prospective designs) over the topic.
Retrospective studies
Here we discuss most of the studies published in the literature. The intention of this narrative review is not to detail every single result of all studies published, due to a high number of publications, mostly with similar methodology and limitations. This is published elsewhere. 13 We focus on the most important studies, with larger samples and better analyses, or with special situations such as elective procedures or laparoscopy. We classified the publications as positive studies (those with a significant impact of anti-TNFs on postoperative complications) or negative studies (those with no relationship between these agents and postoperative morbidity).
Positive studies
Despite an initial study from Colombel et al. 29 in 2005, which did not demonstrate any effect of IFX on postoperative complications, the first study that outlined this possibility was published in 2008, by Appau et al., 17 from the Cleveland Clinic, Ohio, United States. Patients with previous exposure to IFX up to 12 weeks before resections for CD were studied and postoperative outcomes were compared with those with no exposure to the drug, before and after approval of the agent. From 389 patients, 70 were exposed to IFX before surgery. The authors concluded that IFX increased the risk of abdominal sepsis, abscesses, and readmissions, and suggested that diverting stomas should be indicated in patients with previous use of this anti-TNF agent.
Syed et al., in 2013, 30 published the results not only related to intestinal operations due to CD, but also to other abdominal procedures in patients previously exposed to anti-TNF agents. From July 2004 to May 2011, 325 abdominal procedures were performed in a tertiary center (150/46% with previous exposure to anti-TNF agents up to 8 weeks before the operations). Patients in the anti-TNF group had more overall infections (36% versus 25%, p = 0.05) and a trend towards surgical site complications (36% versus 25%; p = 0.10). Preoperative anti-TNFs were an independent predictor of overall infections [odds ratio (OR) 2.43, 95% confidence interval (CI) 1.18–5.03] and surgical site complications (OR 1.96, 95% CI 1.02–3.77).
Jouvin et al. 31 analyzed postoperative outcomes of 360 patients with CD submitted to ileocolic resections from 2002 to 2013. Laparoscopic procedures were performed in 110 cases (31%), with primary anastomoses in 301 patients. Overall morbidity was 24.2%, with 0.8% mortality. Preoperative use of anti-TNF agents was identified as an independent risk factor for overall morbidity (OR 2.05, 95% CI 1.08–3.82; p = 0.027) and septic complications (OR 2.14, 95% CI 1.03–4.29; p = 0.04). In subgroup analysis of patients with primary anastomoses, previous anti-TNF exposure was not associated with higher complication rates.
Negative studies
Regarding the relationship between anti-TNF agents and postoperative complications, most of the retrospective studies concluded that no effect exists. Overall, these studies are more robust and comprise larger samples of patients.
Nasir et al. 16 demonstrated the experience from the Mayo Clinic in patients previously exposed to three types of anti-TNF agents (n = 119) in CD and compared the outcomes with patients with preoperative conventional therapy (n = 251). Postoperative complications were identified in 27.9% in the anti-TNF group as compared with 30.1% in controls (p = 0.63). Infections were described in 5% versus 7.2% in these groups, respectively (p = 0.44). Univariate analysis identified only age and penetrating disease as risk factors for intra-abdominal infections.
Waterman et al., 32 from Toronto, described similar results. After reviewing 473 procedures (195 in patients under previous anti-TNFs and 278 in matched controls), there was no significant difference in the length of stay, and the rates of urinary tract infections, pneumonia, bacteremia, readmissions, reoperations, and mortality. On univariate analysis, previous exposure to anti-TNF agents led to more wound infections as compared with controls (19% versus 11%, p = 0.008), which was not confirmed in multivariate analysis. For the first time, detection of serum levels was studied regarding postoperative complications, and detectable IFX levels did not increase rates of wound infections (p = 0.21), despite the levels that were measured in a small number of patients from the sample.
Norgard et al. 18 analyzed postoperative outcomes from a national database in Denmark in a 10-year period, in 2293 patients with CD. Patients were allocated to one of two groups regarding preoperative use of anti-TNF agents up to 12 weeks before the procedures. From the total sample, 214 were previously exposed to these agents and 2079 were not. The authors did not find higher mortality or increased rates of abdominal abscess drainage in the biologics group after 30 or 60 days. Anti-TNF exposed patients had a 7.5% 30-day reoperation rate versus 8.6% in non-exposed patients (adjusted OR 0.92, 95% CI 0.52–1.63). Patients with previous use of anti-TNFs had a 3.8% leak rate as compared with 2.8% in those without (adjusted OR 1.33, 95% CI 0.59–3.02). Additional analyses did not demonstrate an increased risk of bacteremia after 30 days or any increased risk when anti-TNF administration was performed less than 2 weeks before surgery.
Krane et al. 33 demonstrated results exclusively in laparoscopic surgery in patients with CD exposed or not to IFX preoperatively. From 518 patients studied from 2004 to 2011, 142 had previous exposure to IFX. Conversion rates to open surgery were similar between patients in the IFX groups as compared with controls (6.3% versus 9.35, p = 0.36). There was no difference in the rate of overall early morbidity (p = 0.93) or mortality (p = 0.61). Similar rates were also described between the groups in terms of anastomotic leaks (2.1% versus 1.8%, p = 0.81), infections (12% versus 11.2%, p = 0.92) and thromboembolic complications (3.5% versus 5.6%, p = 0.46).
Kotze et al. 19 demonstrated the results in 123 patients, exclusively in elective abdominal surgical procedures in CD. Emergency operations (an important bias most of the studies) were excluded from the analysis. There was no significant difference between the groups regarding overall surgical complications (32.69% in conventional therapy versus 39.44% in anti-TNF patients, p = 0.457) or overall medical complications (21.15 versus 21.13%, respectively, p = 1.000). Previous use of steroids and hypoalbuminemia were considered risk factors for medical and surgical complications. Previous use of IFX or ADA was not associated with increased postoperative morbidity.
A propensity-score matched analysis performed exclusively in patients with preoperative ADA demonstrated similar results. 28 Patients with preoperative ADA were matched according to age at surgery, CD location, and phenotype, to controls. There was no significant difference regarding the incidence of overall surgical complications (36% in ADA group versus 40% in controls, p = 1.00) or overall medical complications (12% versus 36% respectively, p = 0.095). Preoperative ADA was not considered a risk factor for postoperative complications in univariate analysis.
Meta-analyses
Since 2006, in a full literature search, a total of 18 meta-analyses and systematic reviews were identified. From those, 13 included exclusively patients with CD, with 5 analyzing inflammatory bowel disease (IBD) overall [CD and ulcerative colitis (UC) patients]. Similarly, to what was explored in the retrospective studies session, we describe separately the meta-analyses with significant effect (positive) and those without significant difference (negative) regarding the possible effect of anti-TNF agents on postoperative outcomes.
Positive meta-analyses
Kopylov et al. 34 demonstrated that previous use of anti-TNFs significantly increased the risk of overall postoperative complications 1 month after surgery (primary outcome). Secondary outcomes included infectious and non-infectious complications. A total of 8 studies were included with 1641 patients. Previous use of IFX was associated with an increase in overall complication rates (OR 1.72, 95% CI 0.93–3.19). A modest increase in infectious complications was observed (OR 1.50, 95% CI 1.08–2.08).
El-Hussuna et al. 8 performed a meta-analysis to investigate the effect of anti-TNF agents on surgical complications, such as anastomotic leaks, abdominal abscesses, and enteric fistulas. A total of 14 studies were included, with 679 patients with previous exposure to anti-TNFs being compared with 2363 controls. There was clear heterogeneity among the studies. After quality assessment, previous use of anti-TNFs was associated with increased anastomotic complications in less-biased studies [relative risk (RR) 1.63, 95% CI 1.03–2.60]. In studies with higher risk of bias, such association was not described (RR 0.17, 95% CI 0.05–0.60). Authors additionally stated that inadequate bias control in included studies could underestimate the possible risk of previous anti-TNFs in surgical postoperative morbidity. The same group in another publication with more studies included, reached the same conclusions regarding risks of anastomotic complications in patients with previous use of anti-TNF agents. 10
Two other reviews, one with a meta-analysis, reached similar conclusions, with a larger number of patients.21,35 The authors stated that preoperative IFX modestly increased the risk of overall and infections complications in CD patients after abdominal procedures. Ahmed Ali et al. stated that steroids and anti-TNF agents increase the risk of infections and septic shock, and recommend a washout period of these agents before surgical resections in patients with CD. 35
Waterland et al. 36 described results of a meta-analysis with 14 studies and 5425 patients under anti-TNF therapy and 4401 with previous conventional treatment. Anti-TNFs increased the risk of infectious postoperative complications in CD abdominal surgery, particularly surgical site infections (SSIs).
More recently, Lin et al. 37 demonstrated results of another larger sample, with 7115 patients. Similarly, the authors suggested that previous use of anti-TNFs is an independent risk factor for postoperative complications, and recommend delay of surgery aiming for drug washout whenever possible, in order to decrease the risk.
Table 1 summarizes the results of the positive meta-analyses identified.
Main characteristics and outcomes of positive meta-analyses (those with significant impact of anti-TNFs in postoperative outcomes).

Clinical review important article.
IFX, infliximab; NS, non-specified; TNF, tumor necrosis factor.
Negative meta-analyses
Rosenfeld et al. 22 included 6 studies with 1159 patients with CD, and 413 complications were identified (most commonly SSIs, anastomotic leaks, and sepsis). There was no significant difference in the rates of major complications (OR 1.59, 95% CI 0.89–2.86; p = 0.15), minor complications (OR 1.80, 95% CI 0.87–3.71; p = 0.11), reoperation (OR 1.33, 95% CI 0.55–3.20; p = 0.52), or mortality (OR 3.74, 95% CI 0.56–25.16; p = 0.13) between patients under IFX therapy and controls. This was the first meta-analysis that concluded that IFX use could be safe in the perioperative period with no increase in complication rates. Papaconstantinou et al. 23 stated that despite no increased complication rates were observed, no definitive conclusions could be made, in a careful interpretation of the results of included studies.
Huang et al. 39 included 15 studies in a total of 3807 patients submitted to 4189 surgical procedures. Results demonstrated that low albumin levels, preoperative use of steroids, preoperative abscess formation and previous surgery are risk factors for intra-abdominal septic complications. The type of anastomosis, previous use of immunomodulators or anti-TNF agents did not increase the complication rates.
Xu et al., 40 in a recent meta-analysis, investigated 18 studies with 1407 patients with previous IFX therapy in comparison with 4589 patients with conventional therapy. Different complication rates were identified in 9.38–60.56% in the IFX group versus 12.73–53.85% in controls. There was no significant difference between the groups regarding the rates of overall complications (p > 0.05), reoperations (p = 0.70), readmission (p = 0.22), and mortality (p = 0.86). No difference was identified between different countries where the studies were performed.
Table 2 summarizes the findings of the negative meta-analyses discussed in this session.
Main characteristics and outcomes of negative meta-analyses (those with no significant impact of anti-TNFs in postoperative outcomes).

IFX, infliximab; NS, non-specified; TNF, tumor necrosis factor.
Critical view of meta-analyses
As seen in this section, 12 meta-analyses from different groups have had different conclusions regarding the effects of preoperative biologic therapies on postoperative outcomes in CD. This is probably owing to different primary outcomes measured and patient populations included in different meta-analyses. Most of the studies included overall postoperative complications as the main outcome of interest (n = 8). Infectious complications comprised the primary aim in three publications and surgical anastomotic-related complications (dehiscences and intra-abdominal sepsis) were the primary outcome in three studies. Some analyses included composite outcomes (n = 4). Another important point is that definitions of these complications were also not consistent across studies. For these reasons, controversy regarding the precise influence of anti-TNF agents in postoperative complications in CD is still present in this specific type of pooled evidence.
Prospective studies
Few prospective studies have been published in the literature to date, and again, controversy in the results was identified, similarly to what was observed in retrospective cohort studies and different meta-analyses. Two studies demonstrated a possible relationship between the use of biologics and worsen postoperative outcomes. Lau et al. 24 described the very first prospective data in patients undergoing surgery for IBD with preoperative measurement of serum levels of IFX and analyzed postoperative outcomes. From the whole sample of patients, 123 had CD and were submitted to abdominal operations. IFX levels above 3 ug/ml were considered as detectable, and were associated with an increase in the rates of overall infectious complications (OR 2.5, p = 0.03) and infectious complications (OR 3.0, p = 0.03). The increase in overall complications and readmissions rates was more significant in patients with supra-therapeutic levels (above 8 ug/ml). This was the first study to demonstrate a possible cause-effect relationship between the serum levels of an anti-TNF agent and impaired postoperative outcomes.
Brouquet et al., 25 in the GETAID study, demonstrated results of 592 consecutive patients submitted to ileocecal resections from 19 French referral centers. Overall, 143 patients (24.1% of the sample) were previously exposed to an anti-TNF agent up to 12 weeks before surgery. Preoperative exposure to anti-TNF was considered an independent risk factor for postoperative complications (OR 1.99, 95% CI 1.17–3.39; p = 0.011).
Another four prospective studies did not find significant association between previous use of anti-TNFs and postoperative outcomes. Uchino et al., 41 from Japan, demonstrated that in 405 patients submitted to abdominal surgery for CD (20% with previous IFX), the use of anti-TNF agents was not a significant risk factor for SSI. 41 Another prospective study from France (REMIND group), analyzed postoperative outcomes in 205 patients (93 with previous anti-TNF). 26 Neither previous exposure to anti-TNF agents nor detectable levels of the drugs were associated with the incidence of postoperative complications. In multivariate analysis, previous use of corticosteroids was associated with higher complication rates (OR 2.69, 95% CI 1.15–6.29; p = 0.022). El-Hussuna et al. 9 described results with a similar methodology, applied in 46 patients (18 with previous anti-TNFs). The authors measured the levels of several inflammatory cytokines (TNF-α, IL-6, IL-10, IL-8, IL-17, CRP, among others) after surgery and compared the levels of these cytokines between patients with and without preoperative exposure to these agents in different postoperative periods. No differences in surgical stress were noted between the groups regarding immune, endocrine, and hematologic biomarkers, ruling out a possible cause–effect relationship between exposure to the agents and postoperative complication rates.
The PUCCINI trial, the largest prospective multicentric trial over the topic to date, was presented at the Digestive Disease Week (DDW) 2019. 27 Data from 17 centers were prospectively collected from patients submitted to abdominal operations for both CD and UC, with a total of 955 procedures (573 with no previous use of anti-TNFs and 382 with previous use of this medications up to 12 weeks before surgery). The most common surgical procedures included were ileocolonic resections (n = 410), small bowel or colonic segmental resections (n = 185), and subtotal colectomy with ileostomy (n = 168). The rates of overall infectious complications did not differ between patients with previous exposure to anti-TNFs and controls (20% versus 19.4%, p = 0.801) or detectable serum levels of the drugs (19.7% versus 19.6%, p = 0.985). Similarly, no differences in the rates of SSIs were noted in patients with and without previous exposure to the agents (12.4% versus 11.5%, p = 0.692) or detectable preoperative levels of the drugs (10.3% versus 12.1%, p = 0.513). Neither previous exposure to anti-agents nor detectable level, in multivariate analysis, was significantly associated with the risk of overall infectious complications or SSIs. This is the highest level of evidence with the larger sample of patients ever studied to date, and details of the final publication are awaited. Table 3 describes in detail the main results of the prospective studies from the literature.
Main characteristics and outcomes analyzed of prospective studies that outlined the possible effect of anti-TNF agents and an increase in postoperative complications after major abdominal surgery in CD.

ADA, adalimumab; CD, Crohn’s disease; CER, certolizumab pegol; IFX, infliximab; TNF, tumor necrosis factor; UC, ulcerative colitis; VDZ, vedolizumab.
Vedolizumab
Vedolizumab (VDZ) is an anti-integrin agent that blocks leucocyte integrin α4-β7, preventing its binding with addressin MADCAM-1 in the endothelial wall. 42 The mechanism of action blocks leucocyte trafficking from the endothelium towards intestinal layers. VDZ is the first gut-selective biological agent approved for the management of CD and UC, and its use has been increased globally. 43 Once leucocyte trafficking is needed for healing in intestinal layers, controversy as to whether preoperative VDZ could impair anastomotic healing in abdominal operations in CD is a natural query.
Lightner et al. 14 initially presented intriguing data from the Mayo Clinic, with 94 patients with previous use of VDZ who were matched to patients with anti-TNF therapy and conventional treatment, in a retrospective comparison of postoperative complications. Patients in the VDZ group had more postoperative infections and SSI as compared with the other groups. Preoperative VDZ was a significant predictor for SSI (p < 0.001). These results raised the question if VDZ could be safely used in the perioperative period, but the cases were more severe, with less primary anastomoses and laparoscopic approaches in the VDZ group, in a refractory population of patients with CD. 44
A study from the University of Chicago demonstrated opposite results in 64 patients with previous VDZ in a comparison with 129 patients with anti-TNF therapy and 250 with conventional treatment. 45 In a propensity score matching, there was no difference in postoperative rates of complications between patients with VDZ as compared with the other two groups (p = 0.35). Preoperative steroid use and anemia were significant factors for increased complications in multivariate analysis. Park et al., 46 with the same methodology, demonstrated similar results, with no increased risk for complications in patients treated with VDZ. No differences in SSI between the two groups (12% with anti-TNFs and 14.9% with VDZ) was observed. VDZ was considered safe to be used perioperatively according to these results.
Other cohort descriptions and some systematic reviews with meta-analyses were also published after these initial studies, and no difference in patients with preoperative use of VDZ was observed with regards to an increase in postoperative complications. A summary of these studies is described in more detail in Table 4.
Main characteristics and different outcomes of the studies which analyzed the impact of vedolizumab in postoperative complications after abdominal surgical procedures in CD. All studies analyzed CD and UC in the same populations.

CD, Crohn’s disease; IBD, inflammatory bowel disease; TNF, tumor necrosis factor; UC, ulcerative colitis; VDZ, vedolizumab.
Ustekinumab
Ustekinumab (UST) is an anti-IL agent which blocks the p40 subunit from the receptors of both IL-12 and IL-23, consequently reducing production of several proinflammatory cytokines with significant impact in IBD. 51 It was first approved for the management of CD, and more recently for UC.4,52
There are only three studies published to date which investigated a possible effect of the preoperative use of UST on postoperative outcomes in patients with CD (Table 5). The first study by Lightner et al. 53 was a multicentric experience from the US, Italy, and Belgium that described retrospectively postoperative complication rates of 44 patients submitted to major abdominal surgeries in CD, and compared them with a control cohort with previous use of anti-TNF. There were no significant differences between the groups regarding the incidence of SSIs (13% in UST versus 20% in anti-TNFs, p = 0.61) and readmissions (18% versus 10% respectively, p = 0.14). Reoperation rates were higher in the UST group as compared with controls (16% versus 5%, p = 0.01). The authors concluded that the use of UST in the perioperative period can be safe in patients with CD.
Main characteristics and different outcomes of the studies which analyzed the impact of UST in postoperative complications after abdominal surgical procedures in CD.
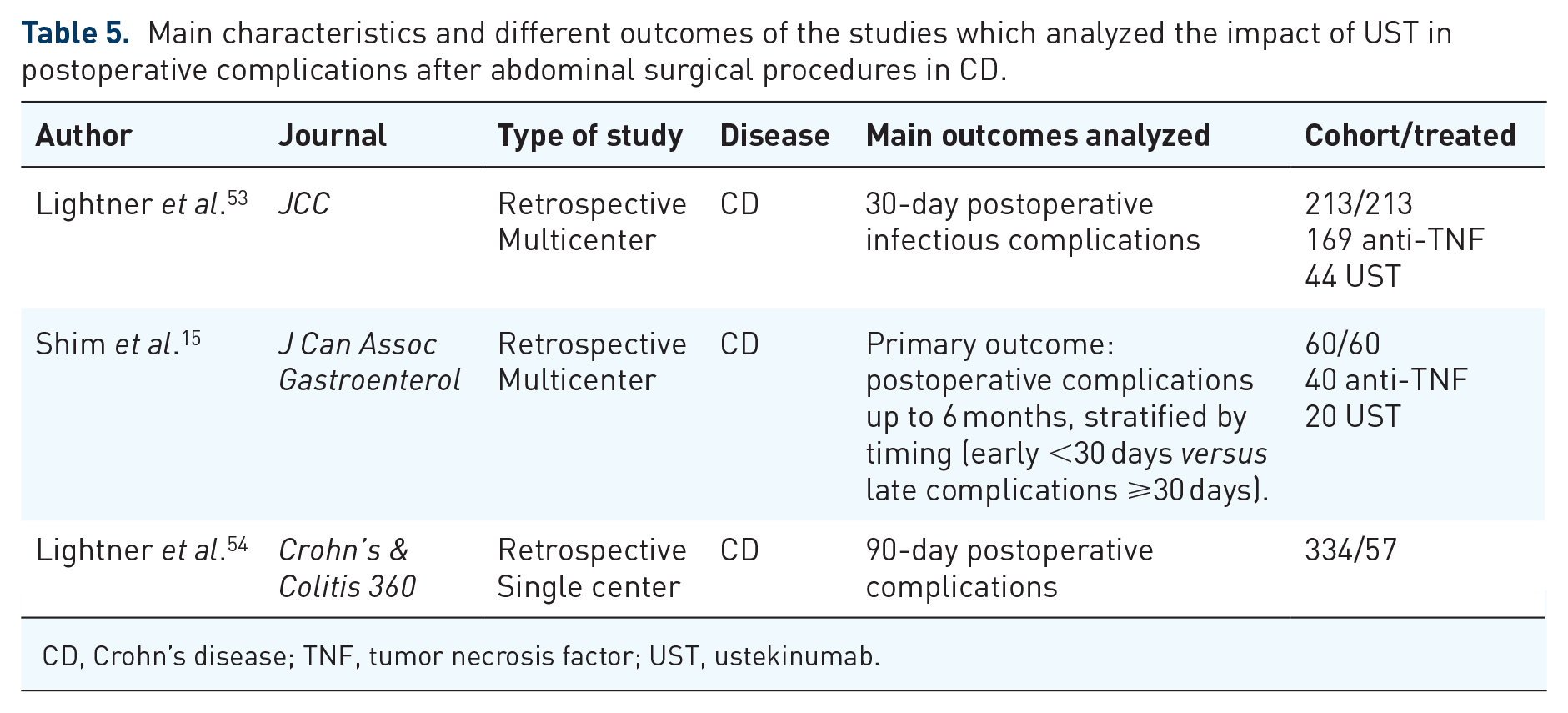
CD, Crohn’s disease; TNF, tumor necrosis factor; UST, ustekinumab.
Similar results were described by a case-control study from Canada. Overall, 20 patients with previous use of UST (median period of treatment of 6.5 months) from the University of Calgary and University of Alberta, who underwent abdominal operations for CD, were matched in a 1:2 ratio with 40 controls, with previous use of anti-TNF agents (median treatment period of 18 months). 15 UST-treated patients had higher rates of ostomy creation (70% versus 12.5%, p < 0.001) and combination therapy (25% versus 2.5%, p = 0.01). However, there was no difference between the groups regarding the risk of SSI (5% in both groups, p = 1.00) and anastomotic leaks (0/20 in UST versus 4/40 in anti-TNFs, p = 0.54).
More recently, results from the retrospective single center cohort from the Mayo Clinic regarding the impact of UST on postoperative outcomes were published. 54 A total of 57 patients submitted to abdominal operations with previous UST were compared with 277 without any biological therapy 12 weeks before the operations. Abdominal sepsis occurred in 14% of UST treated patients as compared with only 5% in the patients without biologic therapy. Preoperative use of ustekinumab was an independent risk factor for intra-abdominal sepsis in logistic regression multivariate analysis (OR, 2.93; 95% CI, 1.16–7.40; p = 0.02). These results with the larger sample of patients in the literature, again input controversy if UST increase the risk of postoperative complications.
Discussion
As seen in this narrative review, the real impact of preoperative biological agents in postoperative complications (medical or surgical) in abdominal procedures in CD remains controversial. 55 Most studies published to date are based on data with anti-TNF agents, clearly due to the early approval of these agents in the management of CD and the larger experience with IFX and ADA in clinical practice as compared with other monoclonal antibodies. Most of the studies included patients with IFX only. Some studies included patients with previous exposure to IFX, ADA, and CER,16,32 suggesting a possible class effect of TNF inhibition in this relationship with surgery. Only one study exclusively included ADA patients, with a limited sample of patients, but with similar conclusions than larger cohorts. 28
Despite the different methodologies used in the studies (most being retrospective single-center or multicenter cohorts), the influence of anti-TNF agents in the postoperative course in CD presents conflicting results. This can be illustrated with the different meta-analyses, which included mostly the same retrospective cohort studies, and came to opposite results.20–22,34,35,37,39,40 This can be explained by different methods of performing meta-analyses, but mostly for the different outcomes from each publication. Some analyzed infectious complications, others analyzed anastomotic leaks, overall complications, among other outcomes. This heterogeneity of results is a consequence of these different approaches from publications. 13
Few prospective studies were published to date regarding the relationship between the exposure to anti-TNFs and postoperative outcomes. The PUCCINI trial is probably based on the best level of evidence presented to date, as data came from American referral centers, prospectively collected in a strict protocol. 27 Its results demonstrated what was found in most of retrospective studies from the literature: no effect of anti-TNFs on postoperative complications. The results of this trial are solid, mostly due to the measurement of serum levels before surgery in the included patients. It is noteworthy that PUCCINI included CD and UC patients in the same group, and the final publication is awaited in order to a more detailed analysis of the results. Other prospective studies, such as the Cedars Sinai cohort 24 and the REMIND French experience 26 also analyzed serum levels, but with a limited sample of patients which could bias the results.
To date, a clear proof of concept demonstrating the impact of biologicals on the postoperative course of CD was not clearly demonstrated. The cause–effect relationship that could be demonstrated by serum levels of the drugs, as an example, was not evidenced in the largest prospective study to date. Moreover, studies that could describe tissue penetration of these agents in surgical specimens are also lacking.
The data including biologicals with different mechanisms of action are still in the early years in the international literature, due to the relatively recent approval of VDZ and UST in clinical practice. As seen in this review, despite the initial alarm study from the Mayo Clinic, 14 which described a possible increase in complications with previous use of VDZ, most studies published more recently described opposite results, positioning VDZ as a safe therapy in the perioperative period.45,46 It is also important to state that a study from Germany demonstrated that a reduction in classical monocytes (M2 macrophages) in systemic circulation is noted with the inhibition of the integrin α4-β7, caused by VDZ, what could impact wound healing. 56 Therefore, owing to this important basic science concept, added to the fact that no prospective studies with VDZ were published to date, decisions should be individualized with caution in clinical practice.
A similar issue is observed with UST. Only three studies were published to date, and the latest that described a possible impact on intra-abdominal septic complication rates after abdominal operations in patients with CD with preoperative use of UST was possibly biased by including a population of severely refractory patients. 54 This could mean a similar bias to what was observed with VDZ in a study from the same institution. Despite the adequate safety profile of UST from clinical trials, more studies are awaited, with improved methodology, to better assess the effect of UST in the perioperative period.
Several other confounding factors can affect postoperative complications in intestinal resections in patients with CD. The most important ones are previous use of steroids, 19 impaired nutritional status, 11 and an unfavorable abdominal environment. Usually, most patients with surgical indication for CD are already using biological agents, and more than one of these factors can also be present. This is illustrated in Figure 1. Therefore, in malnourished patients, with previous steroids and/or anemia, the surgical approach can be affected. More importantly, when unfavorable abdominal conditions are found at surgery, such as abscesses, bowel dilatation, and intestinal partial or total obstruction, the surgical strategy needs to be better defined. Indeed, a change in the surgical approach towards stoma creations instead of primary anastomoses may be the rule in patients under these conditions, not because of the use of the biological agent per se, but for more severe cases with higher risk for complications by definition.

Biological agents approved for the management of Crohn’s disease (CD) and other factors that are involved in an increase in postoperative complications after abdominal surgical procedures in CD. Despite biological agents not directly affecting complications, their use is usually associated with more severe cases with the described confounding factors.
How we do it?
Practical tips are important for the application of evidence to clinical practice. The authors believe that in the perioperative scenario in CD patients under biologics, biological agents are not the single factor involved in decision making, as no cause–effect relationship was demonstrated to date. Is it extremely important to check concomitant use of steroids, phenotype of the disease, and current nutritional status, in order to individualize the surgical plan.
If patients present with elective surgical indication, usually we proceed to surgery in the middle of the cycle of the drug (between the doses). In patients using IFX, VDZ, or UST this is usually done 4 weeks after the last infusion/injection. Patients tend to recover after 4 weeks, when the next dose is administered and no treatment interruption occurs, which can reduce the risk of flares. Patients using ADA usually miss a dose or two, as the period between injections is short (1 or 2 weeks). The decision between an anastomosis versus a diverting stoma is based on the presence of confounding factors such as impaired nutritional conditions, previous steroids, and the presence of perforating disease. If one of these factors are present, a tendency towards diverting stomas can be considered. In emergency situations more conservative procedures are usually undertaken, and a tendency for diverting stomas is based not in the drug per se, but in the broad scenario of infection and intra-abdominal conditions.
Final messages
Controversy as to whether biological agents increase postoperative complication rates after abdominal surgical procedures for CD persists. Most studies included patients with anti-TNF agents, with different results, variation in outcome definition, sample of patients, and severity of cases. The PUCCINI trial described with the better level of evidence to date that anti-TNF agents are probably safe in the perioperative period. Data with vedolizumab suggest the same, despite safety signs in systemic healing in some studies. The safety profile of ustekinumab needs to be better defined with more studies in the future.
When analyzing risk factors for postoperative complications in patients with CD, a broader scenario needs to be considered. Confounding factors such as previous use of steroids, malnutrition, and unfavorable abdominal conditions are usually encountered in surgical procedures in patients with CD under biological therapy. A direct cause–effect relationship of biologics leading to increased rates of complications was never demonstrated. These drugs are commonly used in more severe patients. An individualized multidisciplinary approach with surgeons and gastroenterologists can lead to the best surgical strategy for each patient in the biological era, in surgical management of CD.
Footnotes
Author contributions
Quaresma AB, Yamamoto T and Kotze PG contributed to review conception, literature review, data compilation, critical analysis of data, manuscript draft, and final review.
Conflict of interest statement
ABQ: Abbvie, Janssen, and Apsen. PGK: Abbvie, Janssen, Takeda, Pfizer, and UCB. TY has no conflicts of interest.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed consent statement
The informed consent for this study was not needed according to Brazilian regulations by the IRB review, as a descriptive review with data from the literature included.
Institutional review board statement
Not needed as it is a narrative review.