
Abstract
Gastric cancer is a leading cause of cancer-related death worldwide. Recent evidence suggests that gastric cancer is a complex and heterogenous disease with emerging subtypes shown to affect response to treatment and survival. Immunotherapy is an advancing field and immune checkpoint inhibitors have become standard treatment options in numerous tumor types. In this review, we discuss the current and evolving use of checkpoint blockade, focusing on the anti-PD-1 inhibitor, pembrolizumab, for use in advanced gastric and gastroesophageal cancers.
Introduction
Gastric cancer is the fifth most common cancer worldwide and the third leading cause of cancer-related death. 1 In the United States, gastric cancer is relatively uncommon, comprising 1.5% of all new cancer cases. 2 Specifically, there were 26,240 estimated cases diagnosed and 10,800 deaths in 2018. 3 Gastric cancer is commonly detected at an advanced stage, and most patients diagnosed with the disease will ultimately die from it. Improvements in palliative systemic therapy using a combination of active chemotherapy agents has been shown to increase survival and improve quality of life.2,4–11 The addition of targeted therapy, including trastuzumab, which targets human epidermal growth factor receptor-2 (HER2) overexpression, and ramucirumab, which targets angiogenesis, has also shown modest improvements in survival.12–15 However, the prognosis remains poor with a 5-year overall survival of less than 10%, and for patients that have developed metastases, median survival is still less than 1 year. 2
Gastric cancer encompasses cancers of the stomach and the gastroesophageal junction (GEJ) extending from the distal esophagus to the gastric cardia. It is a heterogeneous disease with diffuse and intestinal histologies and epidemiological differences in tumors arising from GEJ to the antrum. 16 Recent evidence suggests molecular and histological tumor characteristics vary across gastric cancer subtypes and influence prognosis, supporting that gastric cancer is a complex disease. 17 Specifically, gastric cancer can be divided into four subgroups: genome stable (GS); chromosomal instability (CIN); Epstein–Barr virus (EBV); and microsatellite instability (MSI).18,19 Although these subtypes have different clinical and biologic characteristics, we have historically not been able to capitalize on this knowledge in optimizing treatment choices for our patients. However, that is changing, for example, targeting HER2 in tumors that express high overexpression can result in median survival of 16 months, which is well over the expected survival. 12
Immunotherapy, also known as immune checkpoint inhibition, is an emerging novel treatment option in a variety of solid tumors, and has shown promise in patients with gastric cancer. Interestingly, the MSI subtype of gastric cancer is more responsive to immune checkpoint inhibitors. Similarly, across all malignancies, tumors that have defects in the mismatch repair (MMR) system, caused by germline or somatic alterations, are also sensitive to immune checkpoint blockade. These tumors accumulate hundreds to thousands of mutations in the microsatellite regions of DNA during replication, mutations that would normally be repaired if the MMR system was intact. MSI is caused by inactivation of at least one of the MMR genes, which include MLH1, MSH2, MSH6, and PMS2. 20 MSI can also occur by hypermethylation of the MLH1 promoter, leading to functional loss of the protein. 20 The frequency of MSI-high (MSI-H) positivity in gastric cancers ranges from 10% to 22%.18,21 MSI-H positive tumors have increased PD-L1 expression, which has been shown to be a predictor of response to checkpoint blockade.22–24 This is attributable to the inflammatory microenvironment and immune response seen in MSI-H tumors.25–27 The most compelling and transformative aspect of immunotherapy is that the few patients who do respond have durable responses, often greater than 1 year, generally with minimal side effects. Based on modest efficacy, pembrolizumab, which targets the programmed cell death-1 (PD-1) receptor, is now an approved immunotherapy treatment in gastric cancer. Herein, we discuss the current and evolving immunotherapy treatment approaches for gastric cancer, focusing on the anti-PD-1 monoclonal antibody, pembrolizumab.
Pembrolizumab in gastric cancer
Pembrolizumab is a high-affinity anti-PD-1 humanized monoclonal antibody which inhibits programmed cell death-1 activity by binding to the PD-1 receptor on T cells. T cells are normally activated when major histocompatibility complex (MHC) presented peptide antigens bind to the T-cell receptor (TCR). Costimulation by binding of the TCR CD28 to its ligands, CD80 (B7-1) or CD86 (B7-2), on antigen-presenting cells (APCs) is also required for activation. 28 Once activated, T cells express coinhibitory cell surface receptors [i.e. cytotoxic T-lymphocyte antigen 4 (CTLA4) and PD-1] to maintain immune homeostasis. 29 Once expressed, CTLA4 has a higher affinity to bind to CD80 and CD86 on APCs leading to inhibition of T-cell activation. Similarly, PD-1 binds to its ligands, program cell death ligand-1 (PD-L1) and program cell death ligand-2 (PD-L2), to prevent further T-cell activation. Tumor cells have found ways to evade the immune effects by expressing PD-L1/PD-L2 on their cell surface. PD-1 pathway blockade inhibits negative T-cell immune regulation caused by PD-1 receptor signaling, thereby reversing T-cell suppression and stimulating an antitumor response. There are several immunotherapy drugs that target both PD-1 and PD-L1 on the market and have been approved or are undergoing clinical trials (Figure 1). Pembrolizumab is approved for the treatment of multiple tumor types, including gastric cancer.30–37

Currently available checkpoint inhibitors targeting PD-1, PD-L1 and CTLA4.
Federal drug administration approval
Chemotherapy remains the most effective therapy for patients with advanced unresectable or metastatic gastric cancer, with established improvements in survival when compared with best supportive care.4–11 Several classes of cytotoxic therapy are active, but standard practice typically involves a combination platinum/fluoropyrimidine treatment regimen as the first treatment (e.g. first-line therapy). After disease progression, patients would typically receive second-line therapy to include paclitaxel and ramucirumab. There were no approved immunotherapy drugs for patients with gastric cancer, until pembrolizumab monotherapy was approved by the US Food and Drug Administration (FDA) in 2017 based on two related clinical trials.
Pembrolizumab was first studied in the phase Ib KEYNOTE-012 trial. 38 Patients with PD-L1 positive recurrent or metastatic gastric and GEJ cancer were enrolled. PD-L1 is the ligand for PD-1 and can be expressed on gastric cancers as well as other infiltrating cells within the tumor microenvironment. PD-L1 positivity for the KEYNOTE-012 study was defined as immunohistochemical (IHC) staining of at least 1% of scorable tumor cells or the presence of a distinctive interface pattern (which represented IHC staining of PD-L1 on stromal cells). Out of 39 patients treated, the overall response rate (ORR) was 22% [95% confidence interval (CI) 10–39]. Genomic profiling revealed MSI-H status in 17% of patients; of those, 50% achieved an objective response (ORR 57.1%, 95% CI 18.4–90.1). The safety profile was favorable with 13% of patients experiencing grade 3 or 4 treatment-related adverse events including fatigue, pemphigoid, hypothyroidism, peripheral sensory neuropathy, and pneumonitis. There were no treatment-related deaths.
In the phase II multicohort KEYNOTE-059 study, 259 patients were enrolled with recurrent or metastatic gastric/GEJ cancer who had progressed on more than two prior lines of chemotherapy (cohort 1). 31 All patients received pembrolizumab 200 mg intravenously (IV) every 3 weeks until disease progression, withdrawal, or toxicity. Patients were unselected for PD-L1 expression, which was considered positive if the combined positive score (CPS; number of PD-L1 positive tumor and immune cells divided by the total number of tumor cells within a microscopic high powered field, multiplied by 100) was one or greater. In all, 57.1% of patients were PD-L1 positive (e.g. CPS ⩾ 1) and 42.1% were PD-L1 negative. The objective response rate to pembrolizumab was 15.5% (95% CI 10.1–22.4%) in patients with PD-L1 positive tumors and 6.4% (95% CI 2.5–12.8%) in PD-L1 negative tumors. Interestingly, durable responses were observed in both PD-L1 positive and negative tumors. Specifically, the median (range) response duration was 16.3 (1.6+ to 17.3+) months with PD-L1 positive tumors and 6.9 (2.4 to 7.0+) months in PD-L1 negative tumors, respectively. Surprisingly, a total of six patients achieved a complete response, including three patients with PD-L1 negative tumors. These data suggest that selection of patients for pembrolizumab therapy using PD-L1 IHC and CPS scoring successfully enriches for patients who might benefit from immunotherapy, however responses with checkpoint blockade can be attained even in PD-L1 negative tumors. Further, although patients who achieved an objective response with pembrolizumab generally had durable responses, a limitation of pembrolizumab is that only ~15% of patients with PD-L1 positive gastric cancers observed an objective response, for example, the vast majority of patients who receive immunotherapy do not respond. The main exception to this observation is the high objective response rate observed in MSI-H patients with an objective response rate of 57.1% (95% CI 18.4–90.1%). Once again, the safety profile of pembrolizumab showed 17.8% of patients experiencing grade 3 or higher toxicity, including two treatment-related deaths.
GEJ tumors, specifically Siewert type 1 adenocarcinoma, were included in the phase II KEYNOTE-180 study which evaluated the role of single-agent pembrolizumab in the third-line setting for metastatic esophageal carcinoma. 39 The study included both esophageal squamous cell carcinoma, which comprised 52.1% of the study population, esophageal adenocarcinoma and GEJ Siewert type 1 adenocarcinoma. The ORR for the adenocarcinoma group was 5.2% (95% CI 1.1–14.4%) and 14.3% (95% CI 6.7–25.4%) in the squamous cell carcinoma group. The median duration of response was not reached. In patients with PD-L1 positive tumors, the ORR increased to 13.8% (95% CI 6.1–25.4%), and the disease control rate was 36.2%. In contrast, PD-L1 negative tumors had an ORR of 6.3% (95% CI 1.8–15.5%). Patients were not separated out for tumor location and histology but importantly, responses were seen irrespective of PD-L1 status and histology. Of note, PD-L1 expression was based on a CPS of 10 or greater. Treatment-related adverse events occurred in 12.4% of patients including one death from pneumonitis.
Given the modest response rates, but durable responses of nearly 18 months, with minimal toxicity, pembrolizumab is now FDA approved for patients with recurrent, locally advanced, and metastatic PD-L1 positive gastric/GEJ tumors who have progressed following two or more lines of therapy. A summary of key trials is shown in Table 1. This is the first ever drug approved in the third-line setting for advanced gastric cancer.
Summary of KEYNOTE trials 059 and 180.

CI, confidence interval; CPS, combined positive score; DOR, duration of response; GEJ, gastroesophageal junction; m, median; mo, months; NE, not estimable; NR, not reached; ORR, overall response rate; OS, overall survival; PFS, progression-free survival.
Pembrolizumab compared with chemotherapy
In the second-line setting, following disease progression with initial cytotoxic therapy, patients typically receive further cytotoxic therapy such as irinotecan, or taxanes, or the combination of paclitaxel and ramucirumab. In this second-line setting, pembrolizumab was examined in a phase III study (KEYNOTE-061) compared with standard of care chemotherapy. This phase III study failed to show superiority over paclitaxel for patients with advanced gastric/GEJ tumors. 40 KEYNOTE-061 was a random assignment, open-labeled study where patients who had progressed on first-line platinum/fluoropyrimidine based therapy received either standard-dose pembrolizumab or paclitaxel. Patients were unselected for PD-L1 status; however, primary endpoints were overall survival (OS) and progression-free survival (PFS) in patients with a PD-L1 CPS score of 1 or higher. Approximately 67% of patients had a PD-L1 CPS score of 1 or higher, and half were assigned to pembrolizumab and the other half were assigned to paclitaxel. The median OS was 9.1 months (95% CI 6.2–10.7) with pembrolizumab and 8.3 months (95% CI 7.6–9.0) with paclitaxel (HR 0.82; 95% CI 0.66–1.03; p = 0.0421), which did not reach the significance threshold for superiority (pre-specified p-value threshold was p = 0.0135 owing to the required alpha splitting for multiple primary endpoints). Median PFS was 1.5 months (95% CI 1.4–2.0) with pembrolizumab versus 4.1 months (95% CI 3.1–4.2) with paclitaxel (HR 1.27; 95% CI 1.03–1.57). However, pembrolizumab resulted in more durable responses than paclitaxel, with a median response duration of 18.0 months (95% CI 8.3–NE) versus 5.2 months (95% CI 3.2–15.3), respectively. In a subgroup analysis, patients with an ECOG 0 or primary GEJ tumors had greater treatment effects with pembrolizumab. Similarly, in a post hoc analysis, PD-L1 CPS of 10 or higher correlated to a higher response with pembrolizumab. Furthermore, as expected, patients with MSI-H tumors, irrespective of the CPS, responded better to pembrolizumab. Grade 3 or higher adverse events occurred in 14% of patients treated with pembrolizumab and 35% with paclitaxel, consistent with previous reports. Although not statistically superior, pembrolizumab was shown to produce effective and durable responses in patients with PD-L1 CPS of 1 or higher with a manageable safety profile.
In a similar phase III study in esophageal cancer, patients with GEJ tumors (Siewert type 1 adenocarcinoma) were also included and were randomized to receive either pembrolizumab monotherapy or investigators choice of standard-dose paclitaxel, docetaxel, or irinotecan (KEYNOTE-181; ClinicalTrials.gov identifier: NCT02564263). 41 In this study, pembrolizumab was superior to chemotherapy in patients with a CPS of 10 or higher. Specifically, the median OS was 9.3 months in the pembrolizumab arm compared to 6.7 months in the chemotherapy arm (HR 0.69; 95% CI 0.52–0.93; p = 0.0074). They safety profile was also comparable with previous studies. Final results have not been published, but based on the available data, pembrolizumab does appear to have improved activity over chemotherapy in esophageal carcinoma (including GEJ type I) with PD-L1 CPS 10 or higher. Further, these results are consistent with the post hoc analysis of KEYNOTE-061, which also suggested better efficacy of pembrolizumab in gastric and GEJ tumors with PD-L1 CPS 10 or higher.
Among patients with advanced MSI-H or MMR-deficient solid tumors, including gastric cancer, pembrolizumab is approved as a second-line treatment option based on the KEYNOTE-016, -12, -164, and -158 trials.23,30,38,42 In the KEYNOTE-016 study, patients with MMR-deficient noncolorectal cancers had an immune-related ORR of 71% and a median PFS of 5.4 months. Side effects were similar to those reported in other KEYNOTE studies. KEYNOTE-016 is still recruiting and median OS has not been reached.
Integration of immunotherapy into the first line
With the durable responses to immunotherapy as demonstrated in later lines of therapy, immunotherapy has been transformative in the treatment of gastric and GEJ cancer. There has been a push to demonstrate the efficacy of the combination of immunotherapy with chemotherapy, particularly as initial therapy for advanced or unresectable disease. Recently, updated results of the ongoing KEYNOTE-059 (ClinicalTrials.gov identifier: NCT02335411) cohort 2 study were presented. This cohort was the first to examine the safety of combining immunotherapy with chemotherapy in gastric cancer. In this study arm, treatment-naïve patients with advanced gastric/GEJ tumors received pembrolizumab 200 mg IV every 3 weeks plus chemotherapy using cisplatin and a fluoropyrimidine (either 5-fluorouracil or capecitabine, according to physician preference). 43 PD-L1 expression was tested and 64% of patients had PD-L1 positive tumors. The ORR was 60% (95% CI 38.7–78.9) with 32% of patients achieving stable disease (95% CI 14.9–53.5). The typical response rate to chemotherapy alone, specifically cisplatin and fluorouracil) is approximately 30–35%.7,8 These data suggest that the combination of chemotherapy and immunotherapy may have even better activity than chemotherapy alone. Responses were irrespective of PD-L1 expression, with an ORR of 68.8% (95% CI 41.3–89.0) in PD-L1 positive patients and 37.5% (95% CI 8.5–75.5) in PD-L1 negative patients. Furthermore, responses were durable, with a median duration of response of 4.6 months (2.6 to 14.4+) in all patients. Grade 3 or higher treatment-related adverse effects occurred in 75% of patients. No treatment-related deaths were reported. Based on the ongoing KEYNOTE-059 cohort 2 study, the combination of chemotherapy with checkpoint blockade resulted in greater efficacy and durable responses regardless of PD-L1 status. This suggests a role for combination strategies as first-line treatment in patients with advanced gastric/GEJ tumors, which was examined in KEYNOTE-062.
Results of the KEYNOTE-062 study were recently presented during the American Society of Clinical Oncology annual meeting in June 2019. Patients with treatment-naïve, advanced gastric/GEJ adenocarcinoma with PD-L1 positivity (defined as CPS ⩾1) were randomized to pembrolizumab monotherapy, pembrolizumab plus chemotherapy (cisplatin plus a fluoropyrimidine), or chemotherapy alone (control arm). Approximately 70% of patients enrolled across all arms had gastric cancer and 36–39% were CPS ⩾10. Pembrolizumab monotherapy was shown to be noninferior to chemotherapy (HR 0.91; 95% CI 0.69–1.18) meeting the primary endpoint of that experimental arm, whereas the addition of pembrolizumab to chemotherapy was not superior to chemotherapy with a HR 0.86 (95% CI 0.62–1.17), p = 0.158. In patients CPS ⩾10 gastric/GEJ adenocarcinoma, pembrolizumab monotherapy was associated with an improved OS by roughly 7 months (17.4 versus 10.8 months; HR 0.69; 95% CI 0.49–0.97). Notably, PFS with pembrolizumab monotherapy was significantly inferior in patients with CPS ⩾1, with a median PFS of 2.0 months with pembrolizumab and 6.4 months with chemotherapy (HR 1.66, 95% CI 1.37–2.01). In patients with CPS ⩾10, chemotherapy still demonstrated a numerically better mPFS (2.9 mo pembrolizumab versus 6.1 mo chemotherapy).
When considering the pembrolizumab with chemotherapy arm, while OS was not improved with the addition of pembrolizumab, there appeared to be a trend toward improved PFS with the addition of pembrolizumab: for CPS ⩾1 (HR 0.84; 95% CI 0.70–1.02; p = 0.039), and for CPS ⩾10 (HR 0.74; 95% CI 0.53–1.00). Both arms had similar rates of toxicity. While the results of this study may suggest that single-agent pembrolizumab may be considered noninferior to chemotherapy in patients with advanced gastric/GEJ adenocarcinoma with CPS ⩾1, one might consider the risk of early progression with pembrolizumab when considering this option if it achieves regulatory approval. The lack of benefit of combining pembrolizumab to chemotherapy is notable, and is continuing to be examined in other combination chemotherapy studies (Table 2). One explanation for the lack of significant benefit may be related to the dose and scheduling of chemotherapy and its effect on the immune response. Future studies are needed to determine the optimal chemotherapeutic and immunotherapeutic combination.
Ongoing pembrolizumab trials in advanced gastric/gastroesophageal junction cancer (actively accruing, as of 19 April 2019).
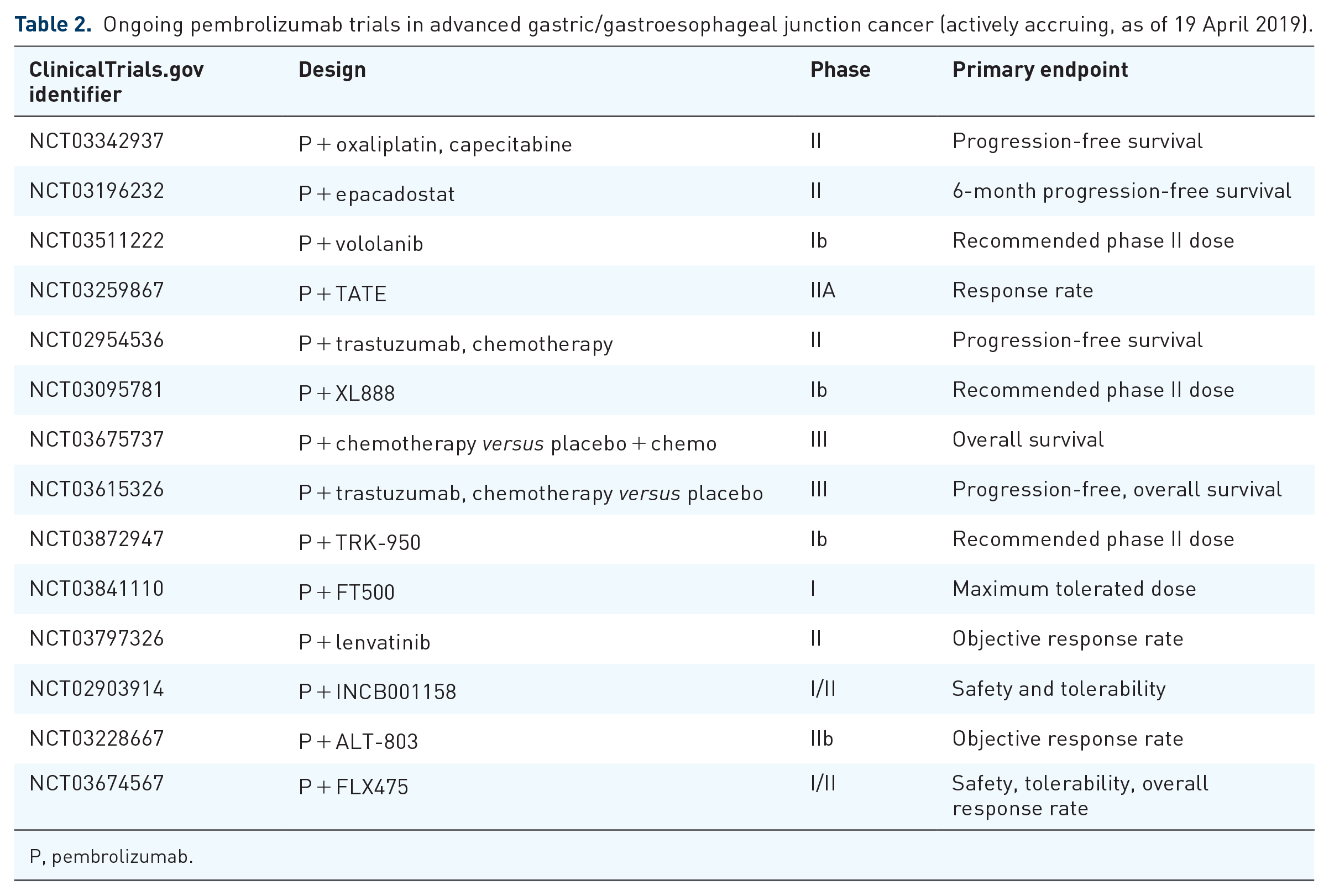
P, pembrolizumab.
In summary, the anti-PD-1 antibody pembrolizumab has been shown to produce effective and durable responses in patients with advanced gastric/GEJ tumors with a favorable safety profile. Pembrolizumab is FDA approved as third-line therapy in patients with PD-L1 positive disease and as second-line therapy in patients with MSI-H/MMR-deficient tumors. Further studies to identify patients who are likely to benefit from pembrolizumab, either alone or in combination with other treatments, are ongoing. Current ongoing studies in advanced gastric/GEJ cancer with pembrolizumab are summarized in Table 2.
CPS as a biomarker for pembrolizumab
Although PD-L1 has proven a modestly effective predictive biomarker for pembrolizumab efficacy in gastric cancer, numerous studies evaluating the relationship between PD-L1 expression and response to checkpoint inhibitors show conflicting results. As a prognostic biomarker, PD-L1 expression correlates with poor prognosis and decreased survival in non-small cell lung cancer (NSCLC), melanoma, hepatocellular carcinoma, pancreatic, and renal cell cancers.44–49 In contrast, there is also data to suggest no prognostic effects of PD-L1 expression in NSCLC and melanoma.50–52 Although several anti-PD-1 and anti-PD-L1 therapies are currently approved, pembrolizumab was approved with the validated companion diagnostic CPS test indicated for NSCLC and gastric/GEJ cancers.53–59 The CPS is calculated as the combined positive number of PD-L1 positive cells (tumor cells, lymphocytes, macrophages) divided by the total number of tumor cells, multiplied by 100 based on IHC staining of formalin fixed paraffin embedded (FFPE) tissues. In the KEYNOTE-59 cohort 1 trial, measuring PD-L1 expression with CPS reliably revealed a population of patients likely to benefit from pembrolizumab. 31 Importantly, the ORR of 15.5% in patients with PD-L1 CPS of 1 or higher was sufficient to support FDA approval of pembrolizumab for this subgroup. Therefore, the advantage of CPS as a predictive biomarker is that it incorporates PD-L1 expression on both tumor and immune cells into a single score and reliably predicts for response to pembrolizumab. 57 Notably, it enriches for patients who may benefit from pembrolizumab only modestly, for example, ~85% of patients with tumors who are CPS ⩾ 1 will not benefit from pembrolizumab. Therefore, there is a desperate need to identify a better biomarker from which to select patients for immunotherapy.
Other immune checkpoint inhibitors studied in gastric/GEJ cancer
Additional checkpoint inhibitors have been evaluated gastric cancer. The anti-PD-1 inhibitor nivolumab was studied in the ATTRACTION-2 trial. 60 This was a phase III trial completed across Japan, South Korea, and Taiwan in patients with advanced gastric/GEJ cancer who had progressed on at least two prior lines of chemotherapy. Patients were randomized 2:1 to receive nivolumab 3 mg/kg or placebo intravenously every 2 weeks. The median OS was 5.26 months (95% CI 4.60–6.37) in the nivolumab group and 4.14 months (95% CI 3.42–4.86) in the placebo group (HR 0.63; 95% CI 0.51–0.78; p < 0.0001). Overall, patients treated with nivolumab had longer survival compared with placebo independent of PD-L1 status: 5.22 months (95% CI 2.79–9.36) in PD-L1 positive (⩾1% IHC staining of tumor cells) tumors and 6.05 months (95% CI 4.83–8.54) in PD-L1 negative tumors. Grade 3 or 4 adverse events occurred in 10% of nivolumab patients including mostly commonly diarrhea, fatigue, decreased appetite, elevated liver enzymes, pneumonitis, colitis, and hypopituitarism. Based on the results, nivolumab could be a potential treatment option for heavily pretreated Asian patients with advanced gastric/GEJ cancer. Nivolumab is approved in Japan for this indication.
In the phase I/II CheckMate-032 study, patients with advanced esophageal, GEJ, or gastric tumors were treated with nivolumab or the combination of nivolumab and the anti-CTLA4 antibody, ipilimumab, and varying doses. 61 As described previously, responses were observed irrespective of PD-L1 status (CPS ⩾1%). The ORR was 12% (95% CI 5–23) in the nivolumab 3 mg/kg arm, 24% (95% CI 13–39) in the nivolumab 1 mg/kg and ipilimumab 3 mg/kg arm, and 8% (95% CI 2–19) in the nivolumab 3 mg/kg and ipilimumab 1 mg/kg arm. Stable disease for at least 12 weeks was seen in 63–67% of patients across all arms. The median OS was 6.2 months (95% CI 3.4–12 months), 6.9 months (95% CI 3.7–11.5 months) and 4.8 months (95% CI 3–8.4 months), respectively. Responses were seen in MSI-H and non-MSI-H tumors. The safety profile was manageable, with a higher rate of treatment-related adverse effects in the combination arms. The CheckMate-032 results suggest the combination of anti-PD-1 and anti-CTLA4 delivers effective and durable antitumor activity in gastroesophageal cancers. Phase III studies to confirm are ongoing.
Despite the relative success of anti-PD-1 antibodies, not all checkpoint inhibitors have resulted in improved outcomes. The JAVELIN Gastric 300 study was a phase III trial where the anti-PD-L1 antibody, avelumab, was compared to chemotherapy in patients with advanced gastric/GEJ cancer who had progressed beyond two lines of treatment. 62 The study failed to meet its primary endpoint, as the mOS was 4.6 months with avelumab and 5 months with chemotherapy (HR 1.1; 95% CI 0.9–1.4; p = 0.81). Furthermore, there was no benefit of avelumab in PD-L1 expressing tumors compared with PD-L1 negative tumors. Additional studies with disappointing results in gastric cancer include monotherapy with tremelimumab (anti-CTLA4; 1/18 partial response >30 months), atezolizumab (anti-PD-L1; 1 durable response of 9.8 months), and durvalumab (anti-PD-L1, 2/28 partial responses).63–65 Efforts to better define and select patients more likely to respond to checkpoint inhibitors warrants further investigation.
Checkpoint blockade and commonly associated toxicities
Immune checkpoint inhibitors can be associated with a wide range of adverse effects. Owing to their generalized effects on stimulating the immune system to target and kill tumor cells, any organ can be affected. The side-effect profile differs greatly compared with standard chemotherapy commonly seen in the clinic, therefore, a strong suspicion must always be present. The most commonly affected sites include the skin, gastrointestinal track, lungs, thyroid, adrenal, pituitary, musculoskeletal, renal, nervous system, hematologic, cardiovascular, and ocular systems. 66 These toxicities can result from any checkpoint inhibitor regardless of its target. Mild adverse effects can be monitored closely, however, moderate to severe toxicities can result in fatal outcomes if not detected early and managed properly with the use of immunosuppressive agents (i.e. steroids). The American Society of Clinical Oncology has published comprehensive guidelines for the management of immune related adverse events specifically in the setting of checkpoint blockade. 66
Conclusion
Gastric/GEJ cancer is a leading cause of cancer-related mortality worldwide. Despite efforts to improve systemic treatment, including combination strategies with chemotherapy and targeted therapy, the majority of patients eventually progress and prognosis remains poor. In the last few years, efforts to define and characterize gastric cancer reveals a complex and heterogenous landscape that has been shown to correlate with treatment response and survival. Immunotherapy has transformed our approach across several diseases, including gastric cancer. Patients with MSI-H tumors have seen significant clinical responses associated with antitumor activity, durable responses, and improved survival. This success across tumor types granted use of pembrolizumab in patients with MSI-H/MMR-deficient tumors as a second-line treatment option. Similarly, positive PD-L1 expression using the validated CPS test has also been shown to predict for response to immune checkpoint inhibitors in multiple tumor types. Recently, pembrolizumab was approved as a third or subsequent line treatment for patients with advanced gastric/GEJ tumors that express a CPS ⩾1. However, using PD-L1 expression as a potential biomarker has been met with conflicting results. In addition, not all checkpoint inhibitors result in antitumor effects in patients with gastric cancer.
In summary, pembrolizumab has marked great strides for immune checkpoint inhibitors in gastric cancer. Further studies evaluating the relationship between molecular tumor characteristics and the immune microenvironment are needed to determine which patients will benefit from checkpoint blockade. Significant effort in drug development lies in augmenting the modest response rates that are achieved with pembrolizumab monotherapy. In addition to novel immune system targets, combining immunotherapy with chemotherapy or with radiotherapy has shown great promise. As in many tumors, immunotherapy is sure to transform our treatment paradigms in gastric/GEJ cancer as well.
Footnotes
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Conflict of interest statement
G.B. declares no conflict of interest. M.A.S. has received research funding (institution) from Merck, Bristol Meyers Squibb, Boston Biomedical, and Astellas pharmaceuticals.
Ethics approval statement
Ethics approval was not required for this review.
Informed consent statement
Informed consent was not required for this review.