
Abstract
Background:
Metabolic syndrome (MetS) has been associated with colorectal adenomas and cancer. However, MetS definitions have changed over time, leading to a heterogeneity of patients included in previous studies and a substantial inextensibility of observations across time or eastern and western populations. Our aim was to evaluate the association of ‘harmonized’ criteria-defined MetS and its individual components with colorectal neoplasia and cancer in a western population.
Methods:
In this multicenter, cross-sectional study, we prospectively evaluated consecutive outpatients who underwent open-access colonoscopy over a 3-month period. MetS was diagnosed according to the 2009 ‘harmonized’ criteria.
Results:
Out of 5707 patients enrolled, we found 213 cancers (3.7%), 1614 polyps (28.3%), 240 nonpolypoid lesions (4.2%), 95 laterally spreading tumors (1.6%). Polyps presented histological low-grade dysplasia in 72.9% of samples, while in 9.8%, high-grade dysplasia or in situ carcinoma was present; dysplasia rates for nonpolypoid lesions were 66.2% (low-grade) and 2.9% (high-grade/in situ carcinoma), while for laterally spreading tumors, 29.6% and 37%, respectively. Overall, MetS prevalence was 41.6%. MetS correlated with both adenomas [odds ratio (OR): 1.76, 95% confidence interval (CI) 1.54–2.00] and cancer (OR: 1.92, 95% CI 1.42–2.58). MetS was the only risk factor for such colonic lesions in subjects younger than 50 years. For all colonic neoplasia, we found MetS and not its individual components to be significantly associated.
Conclusions:
MetS is risk factor for cancer and adenoma in Whites, especially when younger than 50 years. MetS patients might be considered as a high-risk population also in colorectal cancer screening programs.
Introduction
Colorectal cancer (CRC) is an important health issue, since one million new cases are diagnosed worldwide each year, with half a million related deaths.1,2 In most cases it is sporadic in nature, with age being the only major risk factor reported. 3 Metabolic syndrome (MetS), that is, the combination of cardiovascular risk factors, such as obesity, hypertension, diabetes and dyslipidemia,4–6 has been identified as a potential risk factor for cancer, 7 including sporadic CRC.8–10 The prevalence of MetS ranges between 34.8% and 41.9% in the US and 18% and 46% in Europe, depending on age, geographic location or demographic features of the population studied,11,12 thus raising relevant public health implications. In fact, although screening programs based on age and fecal occult blood have proven effective in reducing CRC mortality, 13 identification of other potential risk factors, such as MetS, may further improve cost effectiveness of these screening strategies by favoring a more detailed risk-based stratification of the target populations. Although the concept of metabolic syndrome has been widely accepted for a long time,14,15 there was no largely recognized international definition until 1998 and onward,16–19 up to the ‘harmonized’ classification in 2009 20 that deeply revised the concept of MetS. This has led to the identification of heterogeneous target populations based on the adopted definition. Two recent meta-analyses, although showing an association between MetS and colon cancer, have calculated I2 values indicative of a significant inhomogeneity among studies,21,22 thus weakening their conclusions.
The primary objective of this study, therefore, was to prospectively evaluate the association between MetS, defined according to the 2009 criteria, and colonic neoplastic lesions in consecutive patients undergoing colonoscopy; secondary objectives were to evaluate the role of individual components of MetS in indicating a specific risk for neoplastic disease and, finally, if MetS is a risk factor independent of age.
Methods
Study participants and design
This study has been conducted in 50 open-access endoscopy units, evenly distributed throughout Italy. Every unit prospectively enrolled consecutive outpatients undergoing colonoscopy in a 3-month period.
The indications for performing colonoscopy were abdominal symptoms (impaired bowel habitus, pain, hematochezia, anemia, weight loss, abdominal mass on physical examination), follow up [previous polypectomy, previous colonic surgery, inflammatory bowel disease (IBD)], colon cancer screening [with or without previous positive fecal occult blood (FOBT), voluntary colonoscopy if over 50 years of age, positive family history for CRC]. Patients were excluded in case of failure of cecum intubation, poor bowel cleaning, defined as persistence of solid or semisolid debris that could not be effectively cleaned, 23 age below 30 years, impossibility to obtain anthropometric measurements, polyposis syndrome, advanced neoplastic disease, impossibility to obtain written informed consent. Before implementation, this study was approved by the ethical committee of each participating center and informed consent was obtained from all participants.
For each subject, blood pressure, height, weight, and waist circumference were measured. Interviewers completed a medication history for each participant, including use of insulin, oral hypoglycemic agents, antihypertensive drugs, and hypolipidemic agents. Medical history assessment included also occupation, use of low-dose acetylsalicylic acid, and hormone replacement therapy in women. Self-reported lack of physical activity was also recorded. 24
Laboratory results for fasting plasma glucose, high-density lipoprotein cholesterol (HDL-C), total cholesterol and triglyceride levels were obtained. Since biochemistry data could not be centralized, blood tests had to be performed in sites complying with the updated European guidelines on accreditation of medical laboratories.
Quality control
Eligible endoscopy units were required to have performed at least 1000 colonoscopies in the previous year and to have already participated in at least one previous multicenter study. 25 This ensured that all endoscopists adhered to previously validated quality criteria regarding colonoscopic examination and identification of superficial lesions, in order to avoid heterogeneous diagnoses and noncomparable results. In fact, all endoscopists had already been trained to recognize and classify colonic superficial lesions according to the Paris classification. 26 A 1-day start-up preparatory meeting of at least one investigator from each participating unit was held 3 months prior to the initiation of the study, in order to discuss the protocol and instruct all participants to achieve homogeneous blood pressure and anthropometric measurements.
Blood pressure was obtained sphygmomanometrically, according to standard protocols and techniques. 27 Height was measured without shoes to the nearest centimeter; weight was measured without shoes or heavy outer clothing. Circumferences were measured to the nearest centimeter using a stretch-resistant tape that provides constant tension over light clothing. Waist circumference was measured halfway between the lower ribs and the iliac crest at the end of a normal expiration, when the lungs are at their functional residual capacity, while hip circumference was measured at the largest circumference around the buttocks with the tape parallel to the floor, as per World Health Organization recommendations. 28
Outpatients were consecutively enrolled; endoscopists were blinded to the metabolic status of the examinees.
Definitions
Metabolic syndrome
According to the ‘harmonized’ criteria set forth by a joint scientific multisocietal committee in 2009, 20 MetS is defined as the coexistence of three or more of the following risk factors: waist circumference equal or greater than 102 cm in men and equal or greater than 88 cm in women, serum triglyceride concentration of 150 mg/dl or greater; HDL-C concentration of less than 40 mg/dl for men or less than 50 mg/dl for women; blood pressure of 130/85 mmHg or greater; fasting plasma glucose concentration of 100 mg/dl or greater. Individuals who were using antidiabetics, antihypertensive or hypolipidemic drugs were treated as meeting the criteria for the affected variable.
Colonic lesions and histology
Masses or severely excavated and ulcerated lesions were classified as advanced neoplasia/cancer. Colonic superficial neoplastic lesions (SNLs) were classified according to the Paris classification 26 and subgrouped as polypoid (pedunculated or sessile, 0-Ip and 0-Is, respectively) and nonpolypoid lesions (NPLs) if measuring less than 2.5 mm in height. LSTs (laterally spreading tumors) were defined as lesions measuring less than 2.5 mm in height and more than 10mm in width, as in previous studies.25,29,30 For each type of lesion, size and number were recorded; in case of multiple lesions, measurements were performed on the largest. Location of colorectal neoplasia was defined according to anatomic site. Cecum, ascending colon, hepatic flexure, transverse colon, and splenic flexure were defined as proximal colon; descending and sigmoid colon were defined as distal colon, whereas the rectum was considered separately. Subjects who had lesions in both the proximal and the distal colon were defined as having lesions on both sides. A positive colonoscopy was defined as presence of one or more of the aforementioned lesion types.
All detected lesions, where possible, were resected endoscopically. Biopsies were obtained only in case of suspected advanced cancers or nonresectable lesions that, when confirmed as such, were referred for surgery or palliation. Therefore, histological analysis of superficial lesions was based on resected lesions; in case of multiple resections, the most advanced histological pattern was considered for analysis. All specimens were reviewed by an experienced and dedicated pathologist at each center, who was blinded to the patients’ metabolic status.
Histological findings were classified as hyperplastic lesions, low-grade intraepithelial neoplasia (LGIN: serrated adenoma, tubular adenoma, tubulovillous adenoma, villous adenoma), high-grade intraepithelial neoplasia (HGIN: SNLs revealing high-grade dysplasia or intraepithelial neoplasia or carcinoma in situ 31 ), while lesions with invasive features were defined as submucosal carcinoma, as per current literature. 25 Lesions presenting either LGIN or HGIN were subsequently grouped together under the term adenoma, for statistical analysis.
Statistical analysis
Descriptive analysis included calculations of rates and proportions for categorical data, as well as means and standard deviations (SDs) for continuous data. Differences between means of continuous variables were analyzed using the Student’s t test, while the χ2 test was used for categorical variables. All p values were two tailed, and p values below 0.05 were considered statistically significant.
A standard logistic regression model was used to estimate the association between positive colonoscopy, CRC, SNLs, MetS and demographic, anthropometric, lifestyle and biochemical data by univariate analysis. Significantly associated variables were considered for multivariable analysis, with the additional inclusion of age, sex, absence of physical activity and body mass index (BMI) > 30, unless otherwise specified in individual tables or figures. Results are presented as odds ratio (OR) with a 95% confidence interval (95% CI). Analyses were performed using the SPSS version 17.0 statistical package (SPSS, Inc., Chicago, IL).
Results
In the present study, 5707 subjects out of 5824 have been enrolled; 117 were excluded mainly due to missing data. Demographic, anthropometric and laboratory data are shown in Table 1. Indications for colonoscopy were presence of symptoms in 48%, follow up 38%, colon cancer screening 17%. No previous colonoscopy was reported in 62% of cases.
Baseline characteristics of study participants.

ASA, acetylsalicylic acid; BMI, body mass index; HDL, high-density lipoprotein; n.s., nonsignificant; SD, standard deviation.
Colonoscopy was positive for SNL/CRC in 35.2% (2010/5707) of the procedures, for a total of 2162 lesions observed. Of these, 90.1% were SNL and 9.8% were cancers. Four cases of familiar adenomatous polyposis were diagnosed at this stage and therefore excluded. The majority of neoplasia were sessile polyps (62%); 20.8% were pedunculated, 15.4% were flat elevated and 1.7% were flat depressed lesions. Detailed histological grading of endoscopic findings is shown in Table 2.
Histological patterns of superficial neoplastic lesions (n = 1949).
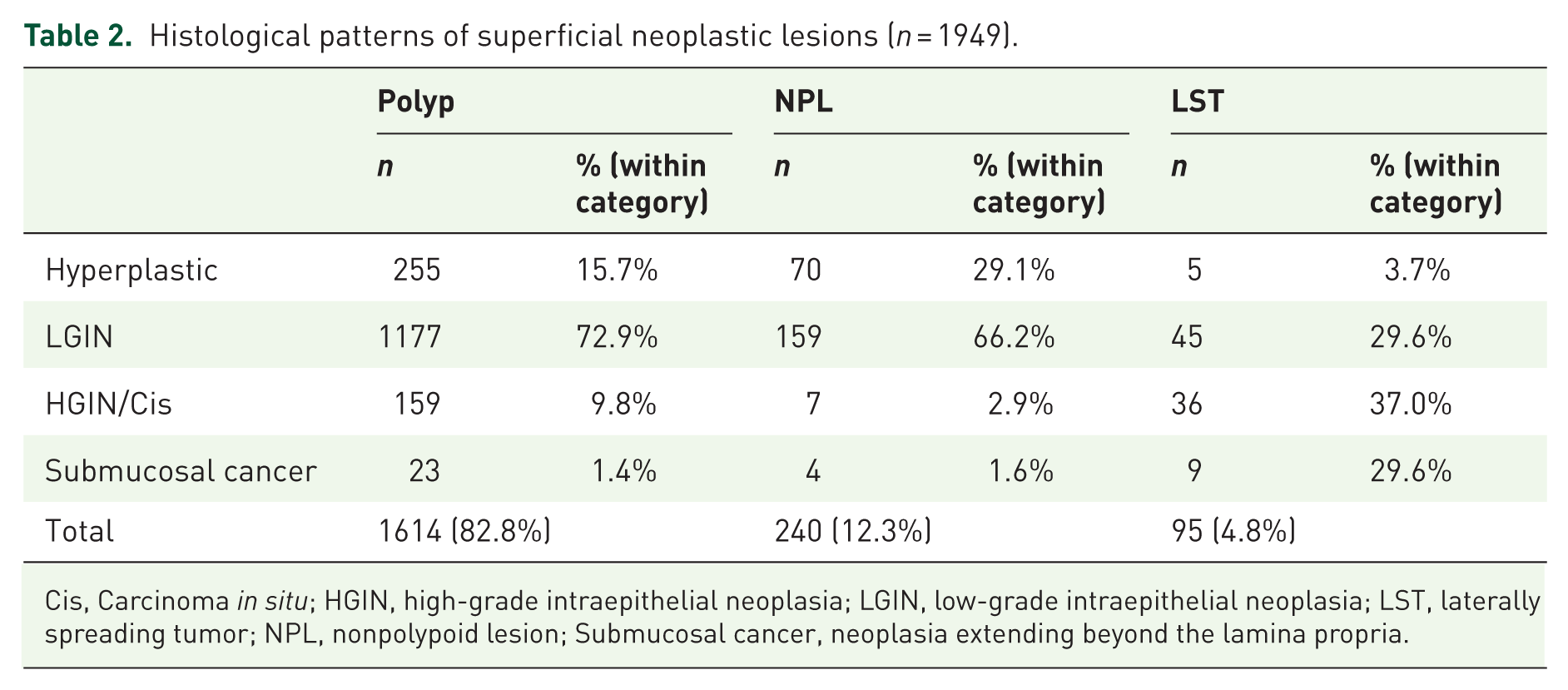
Cis, Carcinoma in situ; HGIN, high-grade intraepithelial neoplasia; LGIN, low-grade intraepithelial neoplasia; LST, laterally spreading tumor; NPL, nonpolypoid lesion; Submucosal cancer, neoplasia extending beyond the lamina propria.
MetS was found in 41.6% of subjects enrolled; it was significantly more prevalent among females (females 43.4% versus males 40.1%; p < 0.05). In both sexes, MetS positively correlated with older age (mean age of MetS versus non-MetS, males 65.3 ± 10.5 versus 58 ± 13.7 years; p < 0.001, females 65.8 ± 10.7 versus 56.1 ± 13.6 years; p < 0.001). Regarding geographic distribution, MetS was found more frequently in individuals from southern Italy (south versus central or northern Italy: OR 1.48, 95% CI: 1.11–2.19; p < 0.001). Northern and central populations were similarly affected.
Male sex (OR 1.48, 95% CI: 1.33–1.66), age > 50 years (OR 3.57, 95% CI: 3.01–4.24), absence of self-reported regular physical exercise (OR 1.29, 95% CI: 1.12–1.48), obesity (OR 1.38, 95% CI: 1.20–1.58) and MetS (OR 2.17, 95% CI: 1.94–2.43) were significantly associated to a positive colonoscopy at univariate analysis. At multivariable analysis, MetS (OR 1.84, 95% CI: 1.63–2.08; p < 0.001), age > 50 years (OR 3.00, 95% CI: 2.51–3.59; p < 0.001) and male sex (OR 1.50, 95% CI: 1.34–1.69; p < 0.001) remained statistically significant when corrected for age, sex, absence of physical exercise and obesity. Notably, obesity did not show any association with colonoscopy outcomes. Overall, MetS significantly associated by multivariable analysis with both adenoma and cancer (respectively, OR 1.76, 95% CI: 1.54–2.00 and OR 1.92, 95% CI: 1.42–2.58; p < 0.001), as did age > 50 years (respectively, OR 3.16, 95% CI: 2.56–3.90 and OR 2.83, 95% CI: 1.59–5.04; p < 0.001); this remained true when colonic and rectal lesions were considered separately. Male sex significantly associated with colorectal adenoma (OR 1.47, 95% CI: 1.30–1.67; p < 0.001) but not cancer, while the opposite was true for subjects reporting no regular physical exercise (OR 1.98, 95% CI: 1.25–3.14; p < 0.01; see Table 3). No differences in terms of anatomical distribution of lesions were observed between sexes; we observed a tendency for a more proximal localization in MetS subjects, although this did not achieve statistical significance. MetS was significantly associated to the presence of both polypoid and NPLs (p < 0.05), but not to their size and number; moreover, no association was found with LSTs.
Multivariable-adjusted estimates of odds ratios for superficial neoplastic lesions and colorectal cancer.
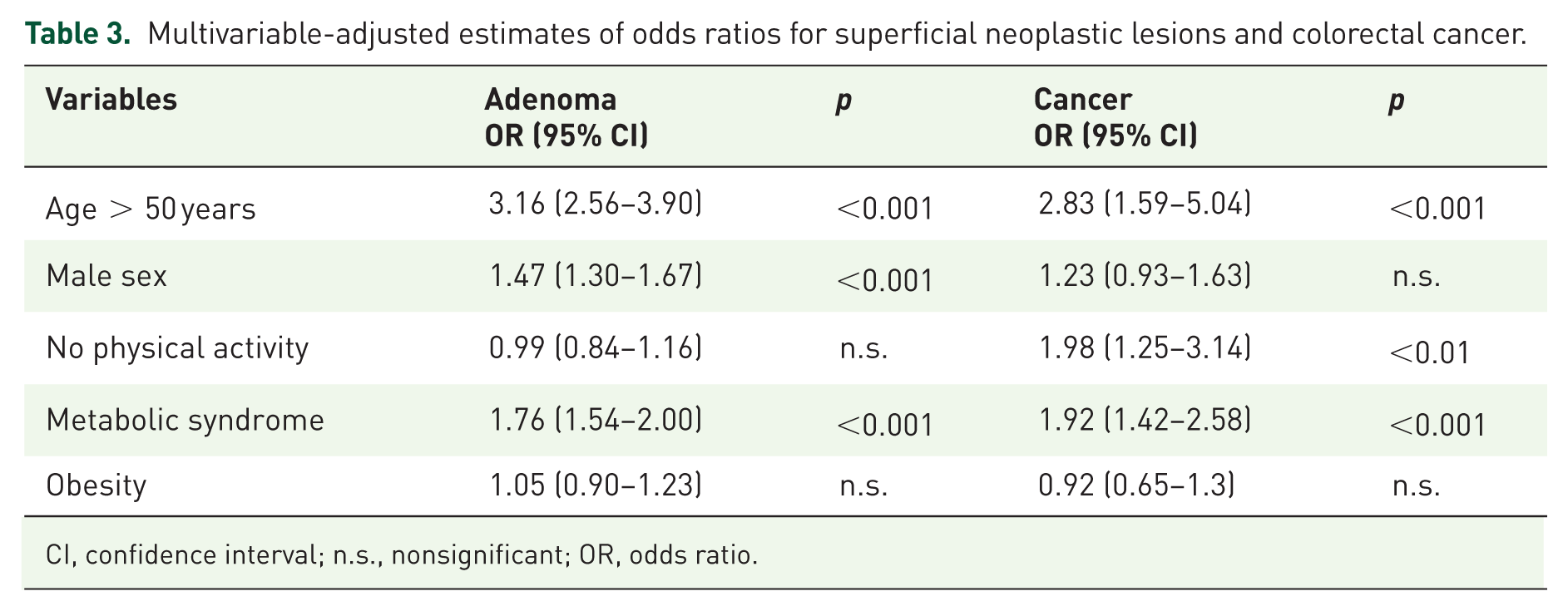
CI, confidence interval; n.s., nonsignificant; OR, odds ratio.
In order to take into account the possibility that colonoscopic neoplasias were more prevalent in symptomatic patients, we performed a multivariable analysis correcting for all indications for colonoscopy (detailed in the Materials and Methods section), as well as sex, age, absence of physical activity and obesity; MetS was again confirmed as independently associated with adenomas (OR 1.78, 95% CI: 1.58–2.00, p < 0.05) and CRC (OR 1.86; 95% CI: 1.40–2.49, p < 0.05). In a subgroup analysis on patients undergoing screening colonoscopies (n = 967), we found 464 lesions (367 adenomas and 24 cancers). In this subgroup, at multivariable analysis, MetS was again associated to adenomas (OR 2.23, 95% CI: 1.70–2.92, p < 0.05). Association with cancer was not statistically significant (OR 1.19, 95% CI: 0.53–2.70, p > 0.05), possibly due to the low number of occurrences (n = 28).
None of the components of MetS was individually associated with a positive colonoscopy in multivariable analysis (Table 4). However, a statistically significant association was observed when at least three components were simultaneously present, as per MetS definition, in both adenomas and CRC (p < 0.05; Figure 1). MetS as a risk factor for neoplastic lesions was independent of BMI; its role was maintained in lean (BMI < 25, OR 2.27, 95% CI: 1.84–2.79), overweight (BMI ⩾ 25 but <30, OR 1.74, 95% CI: 1.47–2.05), and obese subjects (BMI ⩾ 30, OR 2.55, 95% CI: 1.90–3.41, p < 0.05).
Univariate and multivariable analysis of metabolic factors associated with neoplastic findings at colonoscopy.

Adjustment was made for each component of MetS, as well as age, sex and absence of physical activity.
CI, confidence interval; HDL, high-density lipoprotein; MetS, metabolic syndrome; OR, odds ratio.

Occurrence of superficial neoplastic lesions or colorectal cancer according to the number of components of MetS present.
Finally, MetS was an important predictor of a positive outcome at colonoscopy in subjects younger than 50 years, which represented 19.9% of the studied population (555 male, 581 female, mean age 41.6 ± 6.38 years). Although the prevalence of colonic lesions within this age group was expectedly lower than in the elderly (15.8% versus 40.1%, respectively), in subjects with MetS, it was almost three times higher (2.7% versus 0.8%; p < 0.05). In addition, when analyzed in a multivariable model corrected for IBD, family history, sex, physical activity, and obesity, MetS was the only factor associated with the presence of colonic lesions (OR 2.59, CI 95%: 1.78–3.79, p < 0.05).
Discussion
Previous studies from Asian populations have shown that MetS is a risk factor for colonic adenomas.32–34 In one study 35 conducted on a Korean population, MetS was associated to adenomas in the rectosigmoid colon; however, in this study, rectosigmoidoscopy only was performed, and modified Adult Treatment Panel criteria (using BMI instead of waist circumference) were used to diagnose MetS. Morita and colleagues 33 confirmed the association of MetS with adenomas in the proximal colon for lesions greater than 5 mm. However, this study was restricted to male patients and a positive correlation was found only when the lowest cut-off for waist circumference was applied, thereby increasing the sensitivity of MetS diagnostic criteria. The importance of MetS was also highlighted in a recent 5-year follow-up study by Chiu and colleagues, showing that MetS is a significant risk factor for advanced adenoma in negative baseline colonoscopy and low-risk patients. 36
Although the association between MetS and colorectal cancer has been previously investigated,37–39 available studies are widely heterogeneous in terms of the criteria used to diagnose the syndrome; in fact, some studies included features not previously adopted by any internationally formalized definition.37,40–43 Some authors have used BMI, an indicator of obesity rather than of a multifactorial metabolic disturbance, as a discriminatory component for MetS.39,43–45 Studies were also different in terms of design (cohort or association) and endpoints (mortality or incidence);45–47 variable adjustments for confounding factors and ethnicity may also account for disparity. Moreover, although it is known that colon and rectal cancer are different in terms of prevalence, natural history and prognosis, distinctions between them,38,40 or between male and female sex38,41 have variably been described, thus, making the results difficult to pool and interpret. Finally, evolving definitions of MetS have previously required mandatory criteria such as insulin resistance 16 and waist circumference; 18 as such, those individual criteria were, by nature, associated with endoscopic neoplasia because of selection bias.
For these reasons, in this cross-sectional, multicenter, observational study, we have applied the latest ‘harmonized’ criteria for the diagnosis of MetS 20 in a well-defined population of 5707 White patients undergoing colonoscopy. This includes also patients with metabolic disturbances preceding prediabetes or diabetes, hypertension or obesity, thus, strengthening the role of MetS as a cluster of factors and not a mere association of unrelated phenotypes. Our data demonstrate that patients affected by MetS have a significantly increased risk of colonic and rectal adenomas and cancer at endoscopy.
To our knowledge, no consistent data from western countries on the relationship between MetS and colonic lesions are available. Large previous studies on western populations using older or not universally accepted definitions of MetS, many retrospective in nature, have variably reported a positive association between MetS and colonic adenoma or cancer,39,41,43,44,46,48,49 noting important differences between sexes. This is the first large prospective cross-sectional study that establishes an association between MetS, as defined by the current ‘harmonized’ criteria, and adenoma/CRC in a western population. In contrast to previous studies, we have shown that MetS is an independent significant risk factor for neoplastic lesions in the colon and rectum, both in men and women, in a large White population.
Our data demonstrate that patients affected by MetS have a significantly increased risk of colonic and rectal adenomas and cancer at endoscopy. None of the components of MetS when considered individually or in pairs, were associated with an increased risk of neoplasia. On the contrary, simultaneous presence of at least three out of five criteria abruptly increased this risk in a statistically significant fashion, regardless of age. This observation further strengthens the notion that MetS is more than the sum of its parts, potentially indicating an independent underlying pathophysiological drive for epithelial transformation at any age. A previous large retrospective case-control European study, 45 utilizing multiple MetS definitions, including the ‘harmonized’ criteria, found a significant relative risk for colon cancer in affected patients irrespective of the definition used. However, the authors found that this risk was adequately accounted for by the presence of an abnormal glucose metabolism and abdominal obesity, rather than the syndrome itself. Furthermore, cases included only final CRC diagnoses, but not adenomatous lesions or specific endoscopic outcomes.
The potential implication of these findings is that a set of particular dysmetabolic alterations giving rise to MetS might be an important factor that modulates the transition from a hyperproliferative to an adenomatous epithelium. 50 Environmental risk factors and dysmetabolic conditions (obesity, increased visceral adipose tissue, diabetes or insulin resistance, dyslipidemia) have been largely investigated in relation to CRC.8,51,52 Some have reported positive associations between CRC and obesity with an incremental risk of 1.24 for men and 1.09 for women per 5 kg/m2 increase. 51 Others have shown that fat tissue distribution (waist circumference, hip circumference, waist-to-hip ratio), more than BMI, correlates with the risk of colorectal cancer or adenoma,32,53 and that a higher visceral adipose tissue volume is associated to an increased risk for adenoma at baseline and follow-up colonoscopy.54,55 Both adult-onset diabetes mellitus and glucose intolerance have been associated with an increased risk of colon cancer56,57 or adenoma.58,59 Elevated arterial blood pressure, 60 hypertriglyceridemia and hypercholesterolemia61,62 have also been associated with CRC. The mechanisms underlying these associations are not completely understood, yet insulin resistance has been proposed as a key mechanism in promoting cancer through adipokine imbalance, reactive oxygen species and inflammatory cytokine release, such as tumor necrosis factor-alpha and interleukin-6, that act as ancillary pathways in this context.8,50,63–66
In our study, the association between MetS and colonic neoplasia was independent from obesity, as defined by BMI class. In fact, the correlation between this complex metabolic disturbance and colorectal adenoma or cancer was similar in either lean, overweight, or obese patients. Moreover, after accounting for MetS status, BMI-defined obesity showed no residual risk for colonic neoplasia, probably because MetS is a much more specific state of metabolic imbalance, transcending simple overweight/obesity. It has been noted that while BMI is generally an accurate index of obesity in the general population, it is less well correlated to the metabolic disturbances implied by such a status. In fact, it is precisely this drawback of BMI that led to the adoption of waist circumference as a marker of metabolic disturbance and a relevant component of MetS. It has been hypothesized that the partial lack of correlation between these anthropometric indices is due to the fact that waist circumference, a more specific marker of abdominal obesity, is a better predictor of the metabolically active visceral adipose tissue, as opposed to the less active peripheral fat.19,50,54 Previously, colon cancer risk has been reported as more strongly associated with abdominal obesity, persisting even after adjusting for BMI, while the relation between BMI and colon cancer was notably attenuated after adjustment for waist circumference. 67 Thus, MetS should be considered more as including a subset of obese individuals, in whom body mass alone may not be a major factor associated with an increased cancer risk. This is of particular relevance to colonic neoplasia in which the role of other risk factors beyond age and genetics remains to be elucidated.
One additional interesting observation of our study is that patients younger than 50 years were also at risk for neoplasia at colonoscopy, if affected by MetS. This is in agreement with a Korean study on a prescreening population, showing that colorectal neoplasias were significantly more frequent in subjects 45–49 years old, if affected by MetS. 68 These data might suggest that MetS, as defined by the ‘harmonized’ criteria, could be a useful addition to the current screening protocols, in addition to FOBT positivity and age beyond 50 years.
The main limitation of this study is the inclusion of consecutive subjects at colonoscopy, with a significant proportion of symptomatic patients. This design was deemed necessary due to local differences in colorectal cancer screening protocols across Italy, which are implemented on a regional basis. Yet, the per-protocol and post-hoc analyses confirm the role of MetS as a potential risk factor for colorectal neoplasia independently of symptoms.
In conclusion, MetS is associated with an increased risk for colorectal adenoma and carcinoma at colonoscopy, seemingly owing to its underlying dysmetabolic status, regardless of sex and age. This could be particularly useful when targeting younger populations for screening. To this day, aside from age and FOBT positivity, no other dependable clinical marker is used for risk stratification and prevention. Further studies are needed to establish the potential prospective value of MetS as a marker of increased risk for colonic neoplasia, as well as its real-world impact on CRC screening programs and prevention.
Footnotes
Acknowledgements
AM and MN: study concept and design; acquisition of data; analysis and interpretation of data; drafting of the manuscript; final approval of the article.
MAB, LB, LC, EG, and GR: study concept and design; acquisition of data; critical revision of the manuscript for important intellectual content; final approval of the article.
FT: study concept and design; statistical analysis; final approval of the article.
KE: acquisition of data; analysis and interpretation of data; drafting of the manuscript; final approval of the article.
NEOCOSM study group participants: study concept and design; acquisition of data. Please note that all participants in the NEOCOSM study should have the same credit for co-authorship for bibliometric and indexing purposes.

| City | Chief of unit | Coworkers |
|---|---|---|
|
|
SBRAMA Fabio | AGNOLUCCI Angiolo, AGLIETTI Alessandro |
|
|
CANNIZZARO Renato | CANNIZZARO Renato, MAIERO Stefania |
|
|
MASTROPAOLO Gaetano | MASTROPAOLO Gaetano, MONICA Fabio |
|
|
GERMANA’ Bastianello | GERMANA’ Bastianello, LECIS Pier Enrico |
|
|
CESTARI Renzo | CESTARI Renzo, LANCINI Gian Paolo |
|
|
INGROSSO Marcello | INGROSSO Marcello, MARANGI Stefania |
|
|
CARRATO Alfredo | CARRATO Alfredo |
|
|
FORTE Giovanni Battista | GRIMALDI Enzo, ASTRETTO Silvia |
|
|
DI MATTEO Giovanni | CUPPONE Renato, BURATTINI Osvaldo |
|
|
VIRGILIO Clara | VIRGILIO Clara, MIRAGLIA Stefania |
|
|
SACCA’ Natale | SACCA’ Natale, RODINO’ Stefano |
|
|
NERI Matteo | MILANO Angelo, SERIO Mariaelena, EFTHYMAKIS Konstantinos |
|
|
MOBILI Massimo | BALATSINOU Chrysanthi, MANCINI Stefano |
|
|
SPINZI Giancarlo | MANDELLI Giovanna, TOLDI Anna |
|
|
LEO Pietro | LEO Pietro, LEDONNE Ester |
|
|
BUFFOLI Federico | BUFFOLI Federico, IIRITANO Elena |
|
|
MANCA Aldo | ASNAGHI Giuliano |
|
|
ANNESE Vito | ANNESE Vito, BONANOMI Andrea Giovanni |
|
|
RICCI Enrico | RICCI Enrico, DE PADOVA Angelo |
|
|
SAVARINO Vincenzo | GEMIGNANI Lorenzo, GIAMBRUNO Elisa |
|
|
COCCIA Gianni | COCCIA Gianni, ALLEGRETTI Annaglays |
|
|
TOMBESI Giorgio | FELICIANGELI Giuseppe |
|
|
DE MAIO Giovanni | DE MAIO Giovanni, CORAZZA Luciano |
|
|
PIERAMICO Oreste | PIERAMICO Oreste |
|
|
FAMILIARI Luigi | FAMILIARI Luigi, PALLIO Socrate |
|
|
MUTIGNANI Massimiliano | MUTIGNANI Massimiliano, Salerno Raffaele |
|
|
DI GIORGIO Pietro | DI GIORGIO Pietro |
|
|
NARDONE Gerardo | ROCCO Alba, NARDONE Gerardo |
|
|
TEMPESTA Alfonso | MARONE Pietro, D’ANGELO Valentina |
|
|
ROMANO Marco | ROMANO Marco, GRAVINA Antonietta Gerarda |
|
|
DEL PIANO Mario | DEL PIANO Mario, TARI Roberto |
|
|
TOMARELLI Luigi Maria | SILVESTRELLI Marco, BOUSERHAL Toufic |
|
|
CARDONE Francesco Carmelo | CARDONE Francesco Carmelo |
|
|
CIUFFI Mario | TREMOLATERRA Fabrizio, CIUFFI Mario |
|
|
DI GIULIO Emilio | DI GIULIO Emilio, CORLETO Vito |
|
|
CICALA Michele | DI MATTEO Francesco Maria |
|
|
COSTAMAGNA Guido | PETRUZZIELLO Licio, CESARO Paola, COSTAMAGNA Guido |
|
|
PALLONE Francesco | DEL VECCHIO BLANCO Giovanna, COPPOLA Manuela |
|
|
STROPPA Italo | STROPPA Italo |
|
|
ANDRIULLI Angelo | ANDRIULLI Angelo, BISCAGLIA Giuseppe |
|
|
CORDUA Anna Maria | ROMANO Maurizio, BORGHERESI Patrizia |
|
|
SCARPULLA Giuseppe | SCARPULLA Giuseppe, CAMILLERI Salvatore |
|
|
VECCHI Maurizio | VECCHI Maurizio, POLIANI Luca |
|
|
FROSINI Giorgio | FROSINI Giorgio, RENTINI Silvia |
|
|
CIPOLLETTA Livio | BIANCO Maria Antonia, ROTONDANO Gianluca |
|
|
GUGLIELMI Francesco William | GUGLIELMI Francesco William, REGANO Nunzia |
|
|
BURI Luigi | BURI Luigi, SIMETH Catrin |
|
|
ZILLI Maurizio | ZILLI Maurizio, CHECCHIN Davide |
|
|
SPADACCINI Antonio | SPADACCINI Antonio, SILLA Michele |
|
|
GABBRIELLI Armando | GABBRIELLI Armando, BERNARDONI Laura |
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: An unrestricted grant for logistical support was provided by Bracco SpA, Italy.
Conflict of interest statement
The authors declare that there is no conflict of interest.