
Abstract
Background:
The knowledge about risk factors for the onset of uveitis manifestations in patients with inflammatory bowel disease (IBD) is still limited. Here, we aimed to provide an overview of the clinical factors associated with the onset of uveitis in the Swiss IBD Cohort Study (SIBDCS).
Methods:
We included epidemiological and clinical data from 1840 patients with Crohn’s disease (CD) and 1426 patients with ulcerative colitis (UC) followed up in the SIBDCS between 2006 and 2018. Associations between disease characteristics and uveitis were assessed in univariate and multivariate analyses.
Results:
Overall, we identified 285 patients with uveitis. Uveitis was more frequent in patients with CD (11.1%; 205 of 1635) than UC (5.6%; 80 of 1346; odds ratio 2.11, p < 0.001). The occurrence of uveitis manifestations in patients with UC and CD was significantly associated with the onset of other extraintestinal manifestations, also in multivariate analyses. The onset of uveitis was associated with the hallmark features of severe disease in both CD and UC, including a higher clinical disease activity index and the use of immunomodulators or calcineurin inhibitors. In CD, uveitis was more frequent in females and showed a positive correlation with a positive family history of IBD.
Conclusions:
Our data demonstrate that uveitis in IBD occurs more often in CD as well as in women and is associated with a more severe disease course. This might guide physicians’ awareness in at-risk patients to the presence of uveitis extraintestinal manifestations and help to improve patient care.
Introduction
Extraintestinal manifestations (EIMs) affecting joints, skin, eyes and the biliary duct represent a common feature in patients with inflammatory bowel disease (IBD). Depending on the organ affected and their severity, EIMs can be even more devastating for the patient than the actual intestinal disease. According to the literature between up to 40% of patients with IBD suffer from at least one EIM during the disease course.1,2 The activity of some EIMs runs in parallel to the activity of intestinal inflammation, such as episcleritis, peripheral arthritis, erythema nodosum and aphthous ulcers; however, the activity of others such as uveitis, primary sclerosing cholangitis (PSC), pyoderma gangrenosum and spondyloarthropathy, is independent of intestinal disease activity.1,3–5 About 25% of patients with IBD suffer from more than one EIM.6,7
Importantly, EIMs may sometimes even occur before the onset of intestinal disease and diagnosis of IBD. 8 The pathogenesis of IBD-related EIMs to date is only poorly understood; however, a current hypothesis suggests that shared epitopes between the inflamed intestinal mucosa and extraintestinal tissue significantly contribute to the occurrence of EIMs. 9 Further, genetic factors might critically contribute to the onset of EIMs because EIMs are associated with genetic risk variants. Particularly, the onset of ocular EIMs is associated with variations in the gene loci encoding HLA-B27 and HLA-B58. 10 Further evidence for a genetic background comes from case-control studies and epidemiologic investigations.7,11,12
After manifestations in joints and skin, the eye is the third major organ affected by immune-mediated EIMs. 1 About 4–10% of patients with IBD suffer from ocular EIMs, with the majority having concomitant Crohn’s disease (CD).13,14 Episcleritis is the most frequent ocular manifestation of IBD, affecting 2–5% of patients with IBD. It is characterized by an increased activity in parallel with increased intestinal inflammation. 15 In contrast, uveitis is independent from intestinal disease and is present in up to 3% of patients with IBD. It frequently precedes IBD diagnosis and is associated mainly with peripheral arthritis and is more common in women than men. 16 A much rarer condition is scleritis, which is not related to intestinal disease activity and may either precede IBD diagnosis or occur thereafter. 15 Other rare ocular manifestations in patients with IBD are keratinopathy and retinopathy/chorioretinopathy. 17
From a clinical point of view, it would be essential to know which patient characteristics predict the onset of ocular manifestations, such as uveitis, in patients with IBD to stratify patients with IBD according to their risk of developing uveitis manifestations, increase vigilance for an early detection and to initiate appropriate treatment. The Swiss Inflammatory Bowel Disease Cohort Study (SIBDCS) featuring a large patient collective with long-term prospective follow up provides an ideal basis for the analysis of risk factors for the development of uveitis.
Patients and methods
Patient data
Demographic and clinical data were obtained from the database of the nationwide SIBDCS. The SIBDCS represents a Swiss-wide multicenter prospective observational population-based study and includes patients with IBD from all over Switzerland. The SIBDCS was initiated in the Canton of Vaud and subsequently extended to all of Switzerland in 2006 in a joint, multidisciplinary effort by gastroenterologists, pathologists, psychologists and bioinformatics specialists. The SIBDCS has been continuously funded by the Swiss National Science Foundation since 2006. To be eligible for participation in the SIBDCS, patients need to be diagnosed with IBD at least 4 months before actual inclusion in the cohort. Repetitively applying a standardized questionnaire, patient data are collected once a year and entered into a central database. Exact inclusion and exclusion criteria and further details on the SIBDCS are described elsewhere. 18 In this study on uveitis in IBD, a total number of 3266 patients in the SIBDCS followed from 2006 to March 2018 were included in our analysis. Of those, 1840 suffered from CD and 1426 from UC or IBD unclassified (IBDU; UC and IBDU were considered as one study group).
Study design
All patients from the SIBDCS (adult and pediatric) suffering from either CD, UC or IBDU were included into our study. Regarding ocular EIMs, only uveitis and iritis were specifically inquired with a distinctive tick box to cross in the physicians’ SIBDC enrollment and annual follow-up questionnaires. The tick box was named: uveitis/iritis. There were no other questions regarding eye manifestations in the questionnaire. Therefore, in the retrospective setting, we cannot distinguish between uveitis and iritis. In addition, the SIBDCS questionnaire did not ask for other ocular EIMs. The physician’s questionnaire was filled out by the treating gastroenterologist. Patients were divided into two groups: one group with uveitis or iritis at the time of inclusion into the cohort or during follow up, and another group without uveitis or iritis manifestations at any time of their disease course. The uveitis manifestations were diagnosed by the physicians involved in the care of the patient; however, from our database, the exact number of patients that were finally diagnosed by an ophthalmologist was not available.
Patients with UC and IBDU were grouped together. Univariate and multivariate logistic regression analysis was performed. The following possible explanatory variables were considered: (1) Epidemiological characteristics: diagnosis of CD, UC or IBDU, sex, age at diagnosis, age at latest follow up, disease duration, body mass index (BMI) at latest follow up, smoking status and family history of IBD. (2) Disease characteristics and complications: activity index, initial and current disease location, EIMs (i.e. other than uveitis including pyoderma gangrenosum, erythema nodosum, aphthous/oral ulcers, ankylosing spondylitis and PSC), existence of CD-related complications such as stenosis, fistula, fissure, abscess, intestinal surgery, anemia and vitamin B12 levels. (3) Selected medications: 5-aminosalicylic acid (5-ASA), antibiotics, steroids, immunomodulators (azathioprine, 6-mercaptopurin), anti-tumor necrosis factor (TNF) antibodies and calcineurin inhibitors. (4) Longitudinal data on uveitis in patients with CD and UC/IBDU.
The Modified Truelove and Witts activity index (MTWAI) and Crohn’s disease activity index (CDAI) were used as measures of disease activity. Disease activity indices were normalized to a value between 0 and 100 and expressed as an activity index. IBD medication was specified by the treating physician in the standardized SIBDC questionnaires at patient inclusion and annual follow-up visits.
Statistical analysis
All statistical analyses were carried out using Stata Software (v.14.2, StataCorp, College Station, TX, USA) and R software (v.3.3.1, The R Foundation for Statistical Computing, Vienna, Austria). QQ-plots were used to assess distribution of continuous data. Gaussian-distributed data were reported as the mean, standard deviation and range, while non-Gaussian data were presented as the median, interquartile range and range. Differences in means between the two independent groups were assessed using the Student’s t test. Differences of non-Gaussian data were assessed using the Mann–Whitney–Wilcoxon rank sum test. Categorical data were presented as raw frequencies and relative percentages. Differences in distributions for categorical data between two or more groups were assessed using the Chi-square test, or Fisher’s exact test in the case of insufficient sample size, respectively. Time-to-event data were analysed using the Kaplan–Meier estimator, using specific techniques to deal with interval-censored data. Results were presented as cumulative proportion curves. Multivariate logistic regression was used to assess the association of multiple factors with the occurrence of uveitis. At first, all factors with univariate p value <0.200 were included into the multivariate model. Nonsignificant factors (p > 0.05) were then excluded from the model one by one, until all remaining factors were significant. In a last step, all factors that were left aside were once more inserted one by one into the model and kept, if proven significant, while checking for model consistency at each step of the procedure.
Ethical considerations
The SIBDCS was approved by the respective ethical committees in Switzerland (Ethics Committee of the Canton Zürich: EK-1316). All patients signed an informed consent for data collection and analysis for research purposes. The current substudy has been evaluated and approved by the scientific board of SIBDCS.
Results
Epidemiology of uveitis in patients in the SIBDCS
Data from 3266 patients with IBD were analysed (1840 CD; 1426 UC/IBDU). Out of those 1840 patients with CD, 877 patients were male and 963 were female. Overall, 11.1% of patients with CD (205) suffered from uveitis either before inclusion or during participation in the SIBDCS. From the total number of 1426 patients with UC/IBDU, 766 patients were male and 660 were female. Overall, 5.6% of patients (80) suffered from uveitis at any time during their disease course. The risk of suffering from uveitis was significantly higher in patients with CD versus UC [odds ratio (OR) 2.11, 1.61–2.76; p < 0.0001].
Disease characteristics and uveitis manifestations in patients with CD
A total of 124 (60.5%) patients with CD with uveitis were female and 81 (39.5%; p = 0.013) were male. Patients with CD without uveitis did not show any significant sex difference (51.3% female versus 48.7% male). Though the age at CD diagnosis did not significantly differ between patients with or without uveitis, the disease duration was clearly different with a median disease duration of 16 versus 12 years in patients with CD with versus without at the time of onset of uveitis EIMs (p < 0.001). More patients without uveitis were initially diagnosed with disease located in the terminal ileum, whereas about one fifth of patients with uveitis manifestations presented with unknown/unclear disease localization at diagnosis. In contrast, no differences were observed regarding disease localization at the latest follow-up visit. Disease severity was significantly higher in patients with uveitis at enrollment as well as at the latest follow-up visit. Interestingly, patients with CD with uveitis had a higher rate of positive family history for IBD (18.0% versus 12.8%; p < 0.001; Table 1).
Disease characteristics and uveitis in patients with UC/IBDU.
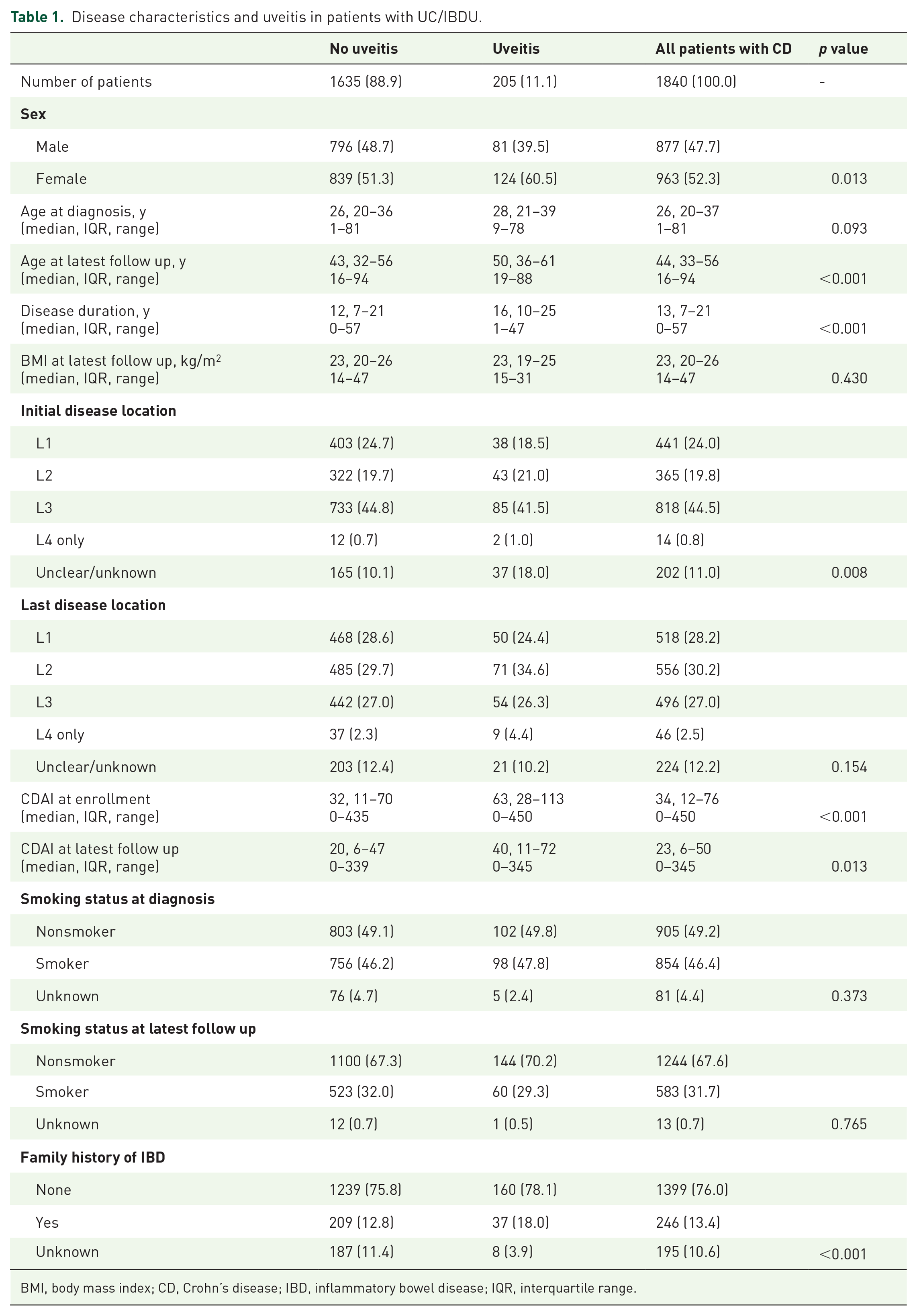
BMI, body mass index; CD, Crohn’s disease; IBD, inflammatory bowel disease; IQR, interquartile range.
Complications and medical treatment in patients with CD and uveitis
Details of complications and medical treatment in patients with CD and uveitis are in Table 2. Of note, patients with CD with uveitis manifestations suffered more often from abscesses than patients without uveitis manifestations (30.2% versus 23.9%, p = 0.047); however, we detected no difference in the occurrence of perianal fistulas, any fistulas, other fistulas or stenosis between both groups. Also, there was no difference with respect to the number of CD-related surgeries. Nevertheless, patients with uveitis suffered more often from anemia and vitamin B12 deficiency and consequently more often received vitamin B12 substitution therapy when compared with patients without uveitis manifestations. We detected several important differences in the treatment history of the patients. Patients affected by uveitis received 5-ASA, corticosteroids, immunomodulators and anti-TNF antibodies significantly more often. In addition, patients with uveitis also suffered considerably more often from other EIMs: the risk of suffering from a concomitant EIM throughout all individual EIMs in patients with uveitis was increased approximately threefold.
Complications and medical treatment in patients with CD with uveitis.

5-ASA, 5-aminosalicylic acid; CD, Crohn’s disease; IBD, inflammatory bowel disease; IQR, interquartile range; PSC, primary sclerosing cholangitis; SIBDCS, Swiss IBD Cohort Study; TNF, tumor necrosis factor; vit., vitamin.
A higher CDAI at the latest follow-up visit, immunomodulatory treatment and the presence of other EIMs (the latter with an OR of 4.692; 2.745–8.019, p < 0.001) were shown to be independent risk factors for the onset of uveitis in patients with CD in the multivariate logistic regression analysis (Table 3).
Multivariate logistic regression results for patients with CD.
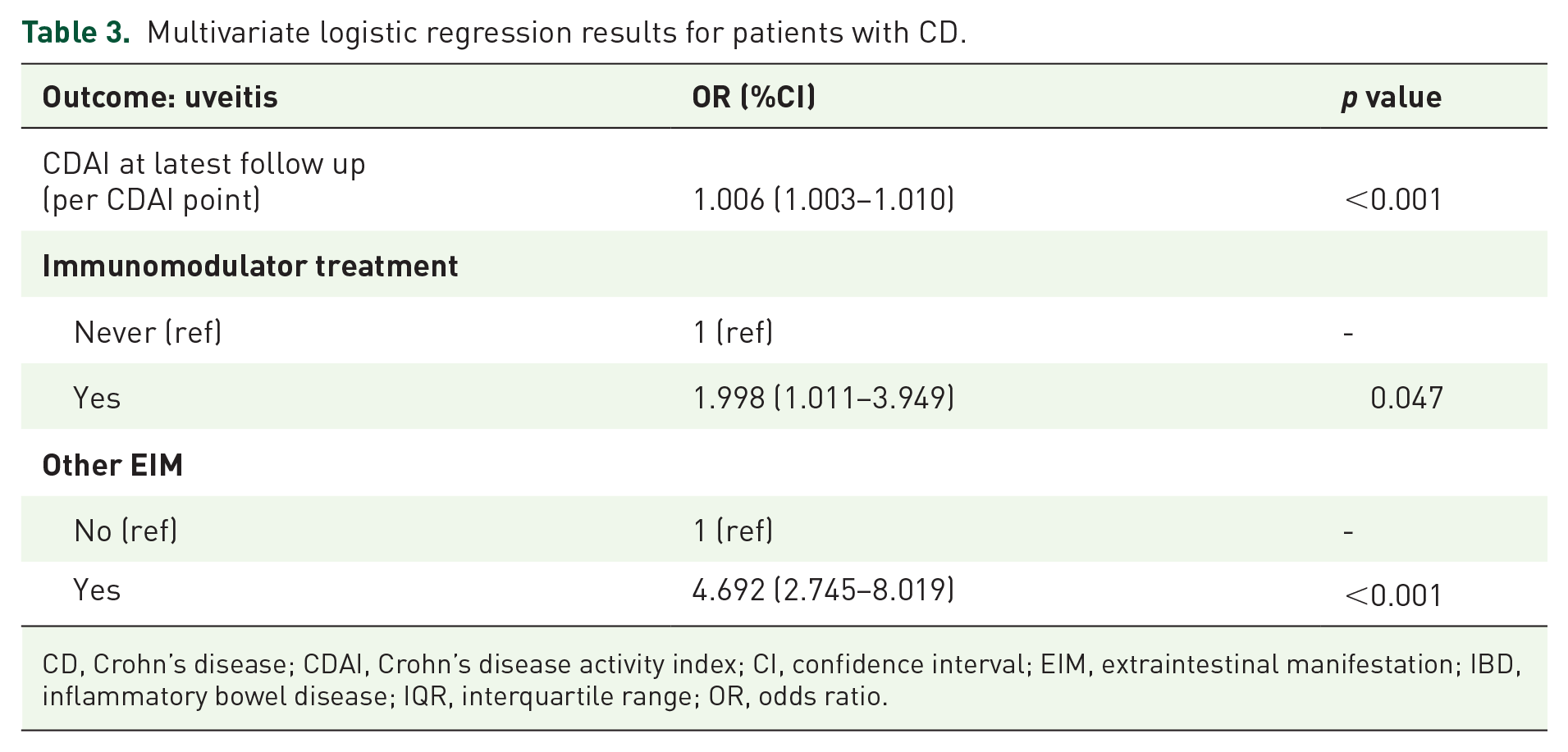
CD, Crohn’s disease; CDAI, Crohn’s disease activity index; CI, confidence interval; EIM, extraintestinal manifestation; IBD, inflammatory bowel disease; IQR, interquartile range; OR, odds ratio.
Disease characteristics and uveitis in patients with UC/IBDU
Table 4 shows the disease characteristics and uveitis in patients with UC/IBDU. A total of 45 (56.3%) male and 35 (43.7%) female patients with UC had uveitis manifestations. Patients with UC and uveitis had a significantly longer disease duration (median 14 versus 11 years, p = 0.001), and higher disease activity indices (MTWAI) at enrollment as well as at the latest follow up compared with patients without uveitis manifestations.
Disease characteristics and uveitis in patients with UC/IBDU.
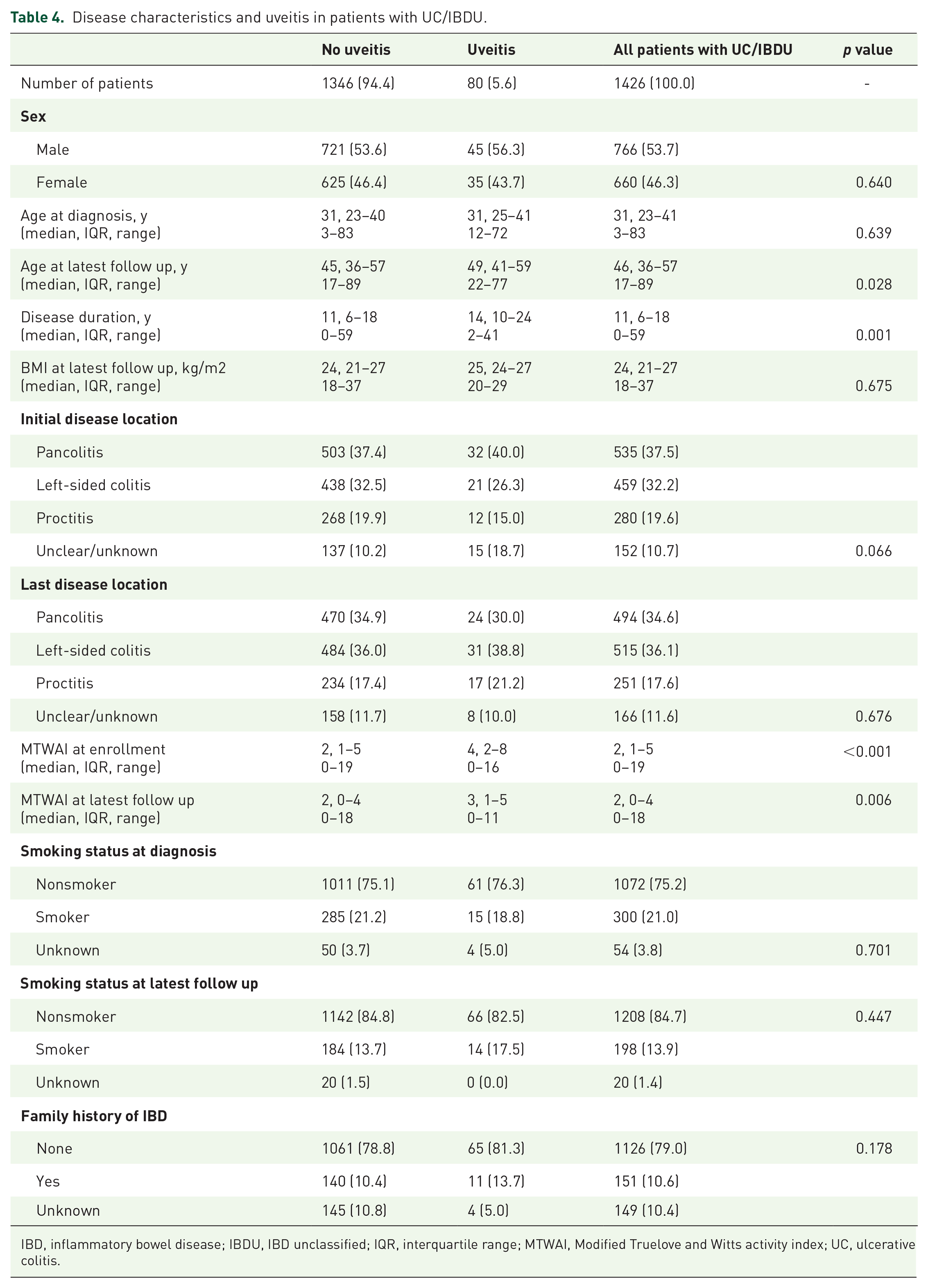
IBD, inflammatory bowel disease; IBDU, IBD unclassified; IQR, interquartile range; MTWAI, Modified Truelove and Witts activity index; UC, ulcerative colitis.
Complications and medical treatment in patients with UC/IBDU and uveitis
Similar to CD, patients with UC and uveitis also suffered significantly more often from at least one other EIM with again an approximately threefold increased risk (2–7.5-fold depending on the respective EIM; Table 5). Of note, PSC was the only exception. More than 90% of patients with uveitis received corticosteroids (compared with 78.5% without uveitis, p = 0.006) and also had antibiotics and calcineurin inhibitors more frequently during the disease course. No difference between both groups was detected for the use of anti-TNF antibodies, immunomodulators or 5-ASA. While patients with UC and uveitis received vitamin B12 substitution more often, there was no difference detected for IBD-related surgery, anemia or vitamin B12 deficiency.
Complications and medical treatment in patients with CD and uveitis.

5-ASA, 5-aminosalicylic acid; CD, Crohn’s disease; IBD, inflammatory bowel disease; IBDU, IBD unclassified; IQR, interquartile range; PSC, primary sclerosing cholangitis; SIBDCS, Swiss IBD Cohort Study; TNF, tumor necrosis factor; UC, ulcerative colitis; vit., vitamin.
The age at diagnosis, vitamin B12 supplementation, need for calcineurin inhibitors (OR: 2.285 [1.128–4.628], p = 0.022) as well as the presence of other EIMs (OR: 2.858 [1.538–5.309], p = 0.001) were independent risk factors for the onset of uveitis in patients with UC in the multivariate logistic regression analysis (Table 6).
Multivariate logistic regression results for patients with UC.
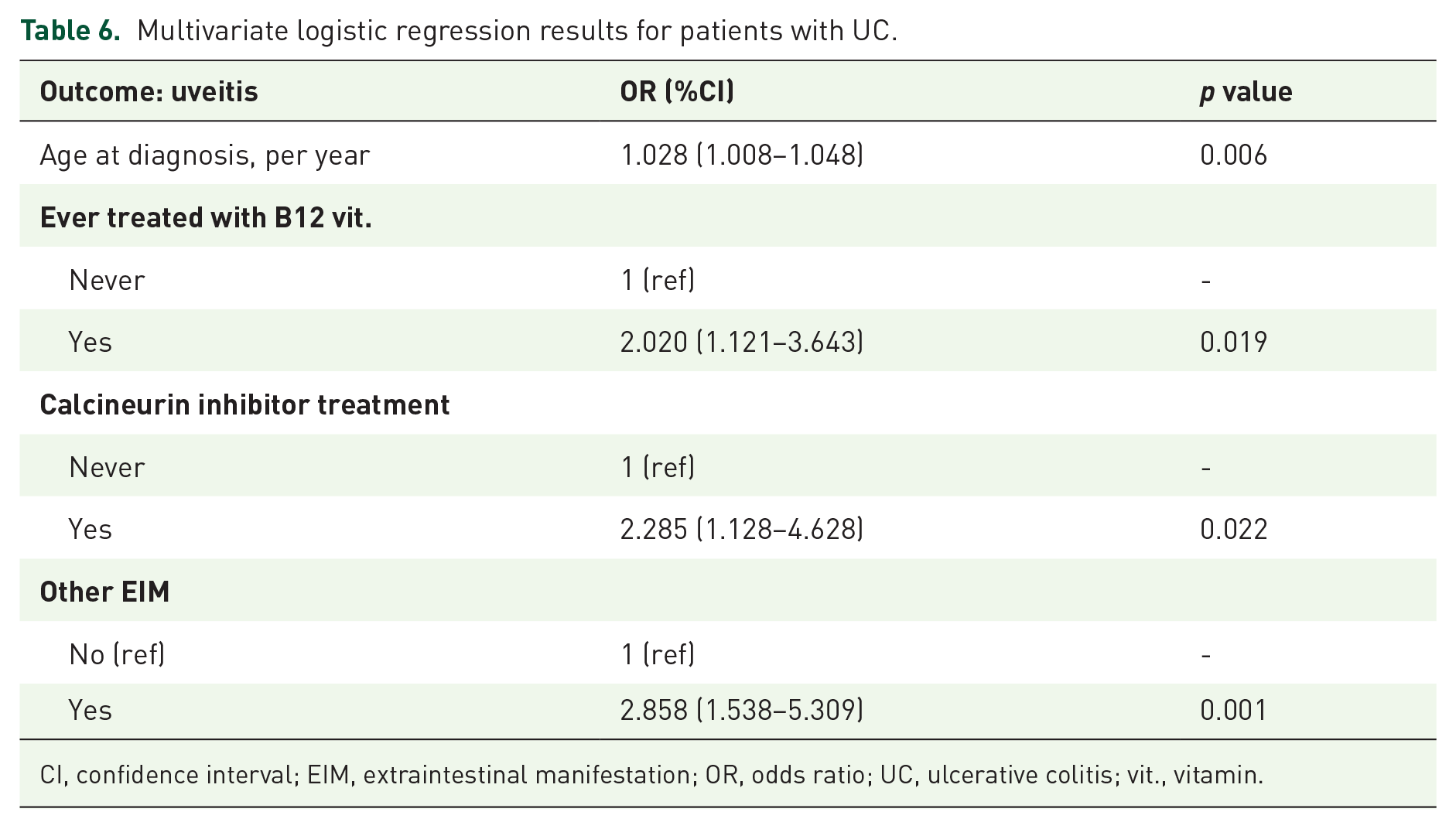
CI, confidence interval; EIM, extraintestinal manifestation; OR, odds ratio; UC, ulcerative colitis; vit., vitamin.
Longitudinal data on the onset of uveitis in patients with CD and UC/IBDU
In a small subset of 23 patients of the SIBDCS, data were available to investigate the sequence of uveitis versus non-uveitis longitudinally in the disease history. In the majority of patients, uveitis was reported as the first EIM (72.2% and 100% in patients with CD and UC/IBDU, respectively). Interestingly, while uveitis was reported before the initial diagnosis in the majority of patients with CD with this EIM (61.1%), uveitis was in contrast, reported after the onset of colitis in most patients with UC/IBDU (80% of patients with uveitis; Table 7). Interestingly, 11 patients with CD and 1 patient with UC/IBDU reported an eye EIM occurrence (uveitis/iritis) even before IBD diagnosis (Table 7). The cumulative proportion of uveitis in CD as well as in patients with UC/IBDU was constantly progressing, and particularly in patients with CD it increased about 6% every 10 years of disease duration (Figure 1). Of note, in our database, for 201 of the 285 patients with uveitis (70.5%), this EIM is mentioned in only one questionnaire, but not in the follow-up questionnaire. This suggests that the uveitis had gone between completing the two questionnaires (that were routinely answered every 12 months) and did not reoccur.
Time of occurrence of uveitis in patients with IBD.

EIM, extraintestinal manifestation; IBD, inflammatory bowel disease; IBDU, IBD unclassified; UC, ulcerative colitis.

Cumulative proportion of uveitis in the SIBDCS.
Discussion
We report on the clinical associations of IBD with uveitis manifestations in the SIBDCS, a large and well-defined cohort of about 3300 patients. Current knowledge about the clinical course as well as the associations of uveitis is limited and findings in the literature are controversial. As a key finding, we detected that the presence of other EIMs is the strongest independent risk factor for the onset of uveitis in both patients with CD and UC. In addition, the use of immunomodulators in patients with CD and calcineurin inhibitors in patients with UC are independently associated with the presence of uveitis.
Ocular manifestations represent the third most common EIM in patients with IBD and the frequency of any ocular EIM ranges between 0.3% up to 13.0% in patients with IBD.19,20 The frequency of ocular EIMs of 5.6% in patients with UC and 11.1% in patients with CD in our study is in line with these data, so is the more frequent occurrence in patients with CD as opposed to patients with UC.10,21,22 Comparable findings were obtained also in the pediatric IBD population in a large systematic review and meta-analysis including 7467 pediatric patients. 23
In the literature, ocular manifestations are generally more frequent in female patients in both, CD and UC;2,10,24 however, in our large patient collective, we found somewhat in contrast, a female preponderance of ocular uveitis EIMs only in patients with CD but not in patients with UC. Overall, in our cohort we detected a substantially higher frequency of ocular EIMs compared with the reported occurrence in the literature, particularly for instance to Bernstein and colleagues. 2
The most striking finding in our cohort is that the presence of uveitis was clearly associated with the onset of other EIMs, mainly arthritis and erythema nodosum. In addition, the presence of uveitis correlated with markers of a severe disease course, particularly the use of immunomodulators or calcineurin inhibitors, suggesting that the occurrence of uveitis per se may be considered a marker of a more severe disease course. This is supported by our finding of a significantly higher CDAI in patients with CD and uveitis than their counterparts without uveitis. An association of ocular EIMs with the onset of arthritis and erythema nodosum was also demonstrated in a recent study of approximately 3450 patients in the United States with IBD. 25 In this study, the gene locus encoding RBM19 was also significantly associated with the onset of ocular EIMs. This might indicate a pathophysiological link between the underlying mechanisms for the occurrence of ocular manifestations and thus, a potential predictive biomarker. 25
Surprisingly, even though smoking is associated with a severe disease course in CD, we did not find any correlation between smoking and the onset of uveitis in our patient collective, confirming findings of a smaller study by Isene and colleagues from 2015. 26 However, in contrast with the data from Isene and colleagues, we found a significant positive correlation between a family history of IBD and the onset of ocular manifestations in patients with CD. 26
Form a clinical perspective, it is important to know the actual type of ocular manifestation that a patient with IBD is suffering from. Since there are sometimes severe courses of ocular inflammation, an appropriate treatment requiring systemic corticosteroids or immunosuppressive medications/biologicals is often necessary. Anterior uveitis and uveitis with an uncomplicated course can be treated with topical corticosteroids. However, severe cases of uveitis or scleritis might need treatment with systemic corticosteroids or, to reduce corticosteroids in the long-term, other immunosuppressive medication or biologics. However, such treatment should always include the opinion of an ophthalmologist before it is initiated. In contrast, episcleritis is often self-limiting or responds to topical approaches. 19
Our study has several strengths, but also limitations. The very large patient collective of the SIBDCS with a highly standardized longitudinal follow up is a strength. In fact, our study is one of the biggest studies to date associating ocular manifestations with disease characteristics in IBD. Nevertheless, our study has also some limitations. First, the questionnaires routinely only asked for uveitis/iritis by a check box. Other ocular EIMs could be entered in a free-text field; however, this might have led to an underrepresentation. In fact, we could only detect 29 patients with eye manifestations other than uveitis (data not shown). Second, although the vast majority of patients with ocular EIMs are seeing expert ophthalmologists, we cannot rule out that some diagnoses of uveitis were made by nonopthalmologists with consecutive risk of over- or underdiagnosis of uveitis and iritis, or even a different ophthalmologic diagnosis, respectively. Third, as uveitis and iritis were recorded simultaneously in the SIBDCS questionnaires, we were not able to distinguish between these two ophthalmologic entities. Fourth, since the questionnaire of our cohort did not specifically ask for the treatment of eye EIMs, we cannot discriminate whether a treatment was initiated because of the eye EIM or, more likely, because of the intestinal IBD symptoms.
Our data provide an overview about the clinical associations and implications of uveitis in patients with IBD. We demonstrate that uveitis occurs in about one tenth of our patients, and therefore recognition of ocular manifestations is of crucial relevance for daily clinical practice. Additionally, the identification of risk factors for uveitis in patients with IBD, which can precede the onset of intestinal inflammation, may help to improve diagnosis of IBD and also of the ocular involvement. Our data might contribute to an increased physician awareness for the presence of ocular EIMs in patients with IBD, possibly leading to earlier diagnosis, prompt tailored therapeutic measures and finally improved care of patients with IBD.
Footnotes
Acknowledgements
Members of the SIBDCS Group are as follows:
Claudia Anderegg; Peter Bauerfeind; Christoph Beglinger; Stefan Begré; Dominique Belli; José M. Bengoa; Luc Biedermann; Beat Bigler; Janek Binek; Mirjam Blattmann; Stephan Boehm; Jan Borovicka; Christian P. Braegger; Nora Brunner; Patrick Bühr; Bernard Burnand; Emanuel Burri; Sophie Buyse; Matthias Cremer; Dominique H. Criblez; Philippe de Saussure; Lukas Degen; Joakim Delarive; Christopher Doerig; Barbara Dora; Gian Dorta; Mara Egger; Tobias Ehmann; Ali El-Wafa; Matthias Engelmann; Jessica Ezri; Christian Felley; Markus Fliegner; Nicolas Fournier; Montserrat Fraga; Pascal Frei; Remus Frei; Michael Fried; Florian Froehlich; Christian Funk; Raoul Ivano Furlano; Suzanne Gallot-Lavallée; Martin Geyer; Marc Girardin; Delphine Golay; Tanja Grandinetti; Beat Gysi; Horst Haack; Johannes Haarer; Beat Helbling; Peter Hengstler; Denise Herzog; Cyrill Hess; Klaas Heyland; Thomas Hinterleitner; Philippe Hiroz; Claudia Hirschi; Petr Hruz; Rika Iwata; Res Jost; Pascal Juillerat; Vera Kessler Brondolo; Christina Knellwolf; Christoph Knoblauch; Henrik Köhler; Rebekka Koller; Claudia Krieger-Grübel; Gerd Kullak-Ublick; Patrizia Künzler; Markus Landolt; Rupprecht Lange; Frank Serge Lehmann; Andrew Macpherson; Philippe Maerten; Michel H. Maillard; Christine Manser; Michael Manz; Urs Marbet; George Marx; Christoph Matter; Valérie McLin; Rémy Meier; Martina Mendanova; Christa Meyenberger; Pierre Michetti; Benjamin Misselwitz; Darius Moradpour; Bernhard Morell; Patrick Mosler; Christian Mottet; Christoph Müller; Pascal Müller; Beat Müllhaupt; Claudia Münger-Beyeler; Leilla Musso; Andreas Nagy; Michaela Neagu; Cristina Nichita; Jan Niess; Natacha Noël; Andreas Nydegger; Nicole Obialo; Carl Oneta; Cassandra Oropesa; Ueli Peter; Daniel Peternac; Laetitia Marie Petit; Franziska Piccoli-Gfeller; Julia Beatrice Pilz; Valérie Pittet; Nadia Raschle; Ronald Rentsch; Sophie Restellini; Jean-Pierre Richterich; Sylvia Rihs; Marc Alain Ritz; Jocelyn Roduit; Daniela Rogler; Gerhard Rogler; Jean-Benoît Rossel; Markus Sagmeister; Gaby Saner; Bernhard Sauter; Mikael Sawatzki; Michela Schäppi; Michael Scharl; Martin Schelling; Susanne Schibli; Hugo Schlauri; Sybille Schmid Uebelhart; Jean-François Schnegg; Alain Schoepfer; Frank Seibold; Mariam Seirafi; Gian-Marco Semadeni; David Semela; Arne Senning; Marc Sidler; Christiane Sokollik; Johannes Spalinger; Holger Spangenberger; Philippe Stadler; Michael Steuerwald; Alex Straumann; Bigna Straumann-Funk; Michael Sulz; Joël Thorens; Sarah Tiedemann; Radu Tutuian; Stephan Vavricka; Francesco Viani; Jürg Vögtlin; Roland Von Känel; Alain Vonlaufen; Dominique Vouillamoz; Rachel Vulliamy; Jürg Wermuth; Helene Werner; Paul Wiesel; Reiner Wiest; Tina Wylie; Jonas Zeitz; and Dorothee Zimmermann.
We acknowledge the following author contributions: M.S. conceived, designed and supervised the research. M.S. and G.R. obtained funding. M.S., L.B., L.R. and S.B. interpreted the data and wrote the manuscript. N.F. and J.B.R. performed statistical analyses. All authors edited the manuscript and approved the final version.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by grants from the Stiftung Experimentelle Biomedizin to M.S., Swiss National Science Foundation [Grant No. 314730-146204, Grant No. 314730_166381. and Grant No. CRSII3_154488/1] to M.S. and to G.R. for the Swiss IBD Cohort [Grant No. 3347CO-108792].
Conflict of interest statement
The authors declare that there is no conflict of interest.