
Abstract
Background:
Barrett’s esophagus (BE) is a premalignant condition with increased incidence worldwide both in old and young individuals. However, the role of certain potential risk factors remains unclear in young adults (< 50 years). We aimed to determine the risk factors of BE in young adults.
Methods:
A total of 4943 young adults who underwent upper gastrointestinal endoscopy at our health check-up center were enrolled. The diagnosis of BE was based on histological confirmation. We analyzed demographic factors, laboratory data, potential risk factors such as smoking, alcohol consumption, presence of gastroesophageal reflux disease (GERD) symptoms, and metabolic syndrome for the risk of BE by using binary logistic regression analysis.
Results:
The prevalence of BE was 1.8% (88/4943). Male sex, the presence of GERD symptoms, and smoking were three significant risk factors related to BE. Furthermore, participants who had smoked for 10 pack-years or more had increased risk of BE with dose-dependent phenomenon (p trend < 0.001). The proportion of BE in male participants with both GERD symptoms and a smoking history of 10 pack-years or more was as high as 10.3% (16/155).
Conclusions:
Significant risk factors of BE in young adults are male sex, the presence of GERD symptoms, and smoking. The risk also increases with an increase in cumulative exposure to smoking.
Introduction
Barrett’s esophagus (BE) is characterized by the replacement of the squamous epithelium with columnar epithelium in the distal esophagus.1–3 It is a precancerous lesion with a 20–40-fold increased risk of esophageal adenocarcinoma (EAC), which has a poor prognosis with a 5-year survival rate of less than 15%.4–6 In Western countries, the prevalence of BE and EAC has increased dramatically in recent decades.7–9 Similar findings have also been observed in Asian countries.10,11 A recent meta-analysis showed that the prevalence of histological BE increased from 0.8% (in 1991–1999) to 2.2% (in 2010–2014) in Asia and that Asian populations have the potential for cancerous progression from BE to EAC. 11 In addition, the proportion of the yield of histological BE increased with age. The upward trend reached a maximum value in the sixth decade of age and then maintained a plateau in the following decades. 12 However, the prevalence of BE in people younger than 50 years was variable (approximately 0.7–8.7%) according to previous studies.13–15 Recently, the incidence of EAC has been reported to be increasing in those under 50 years of age. 16 Nevertheless, to date, BE-related risk factors in young adults remain inconclusive. It is difficult to provide information of risk stratification for BE screening in this population.
It is known that male sex, history of gastroesophageal reflux disease (GERD) symptoms, and smoking are regarded as risk factors of BE in aged patients.1–3 The role of these risk factors in the development of BE in young adults remains unknown. In addition, central obesity and metabolic syndrome (MtS) were considered to be associated with BE.3,17 However, several recent studies reported no association between central obesity and short-segment BE.18–20 Specifically, short-segment BE represents the most common type of BE in Asia. 2 Moreover, most studies demonstrated that alcohol consumption does not increase the risk of BE.21,22 However, two recent meta-analyses have revealed that alcohol consumption was positively associated with BE in Asian populations.23,24 Owing to their potential to be modified and inconsistent evidence regarding the development of BE in Asian populations, all these factors require further investigation.
Consequently, we performed this retrospective study focusing on the population of young adults who underwent upper gastrointestinal endoscopy at a health examination center. We aimed to identify the risk factors of BE and to verify the impact of these potential risk factors on BE in young adults.
Materials and methods
Participants
We reviewed 11,879 adults with or without symptoms who underwent upper gastrointestinal endoscopy at the health examination center of Kaohsiung Veterans General Hospital between January 2016 and December 2018. Among them, 1395 individuals underwent more than one round of upper gastrointestinal endoscopy during the study period. We selected the data of the round yielding histological BE or the data of the latest endoscopy if histological BE was not diagnosed during the study period. Among these individuals, we included participants (n = 5320) aged 20–49 years on the day of the visit. Participants with a history of esophageal cancer (n = 1) and with incomplete data in the questionnaire (n = 376) were excluded. Finally, 4943 individuals were enrolled (Figure 1). The Ethics Committee of the Kaohsiung Veterans General Hospital (VGHKS18-CT11-03, VGHKS19-CT5-05) approved the study. The consent from the study participants was not required because the dataset consisted of de-identified data for research purposes.
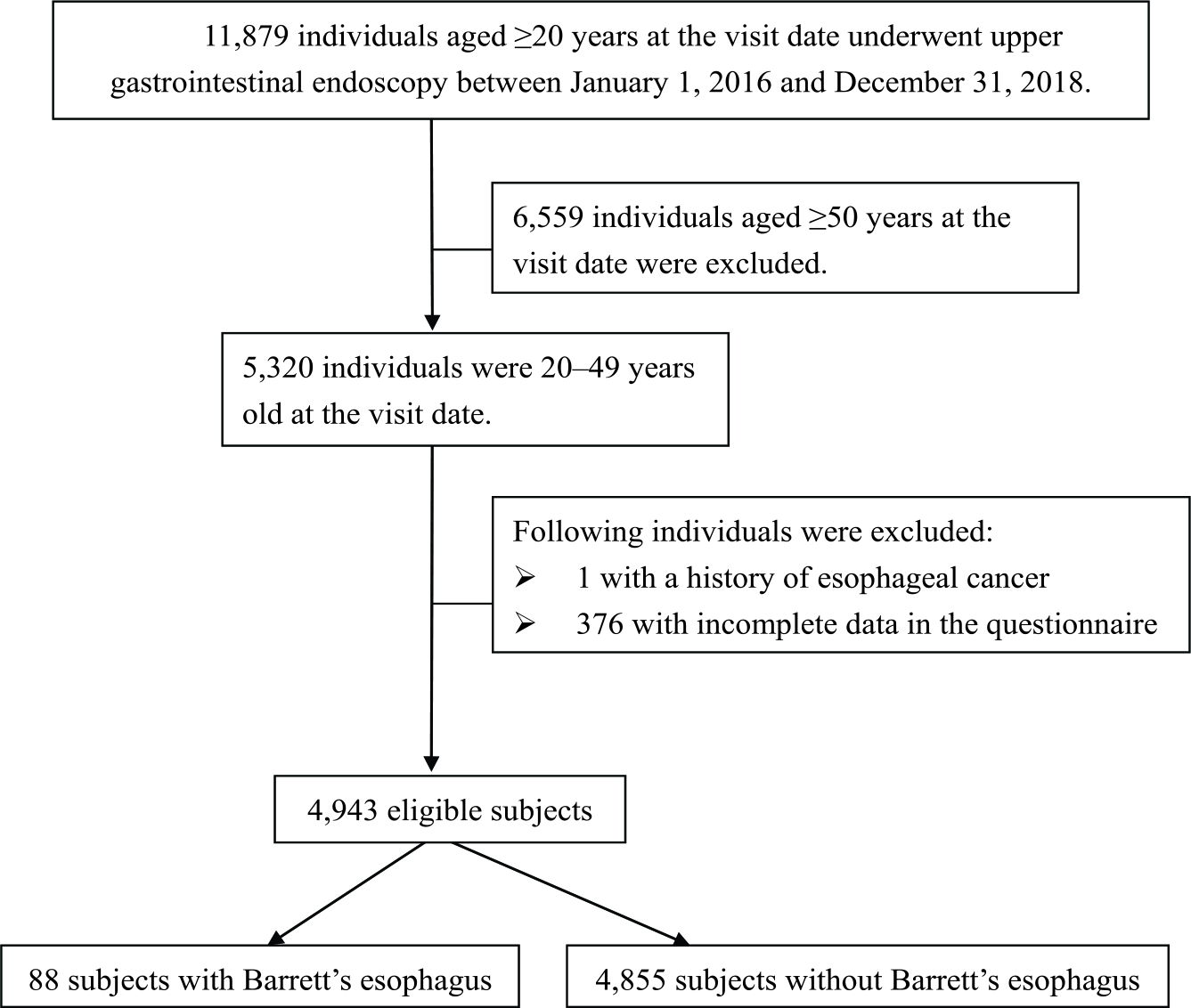
Flow chart of participants enrolled in the study.
Data collection and measurement
All the participants underwent biochemical and blood examinations before endoscopic examination. A questionnaire, including demographic data, past medical history, smoking details (number of packs, frequency, and duration), 25 alcohol intake (number, frequency, and alcohol percentage of drinks per week), 26 and GERD symptoms (heart burn, regurgitation, and dysphagia) in the previous 3 months was provided to all participants who underwent upper gastrointestinal endoscopy at our health examination center. The questionnaire was filled out by participants and then the data were recorded by one physician at our center during the pre-endoscopic examination interview. The body weight and height of all participants were measured using the electric impedance method analyzer (X-SCAN PLUS II, Jawon Medical, Seoul, South Korea). The body mass index (BMI) was calculated as weight (kg) divided by height (m) squared. Waist circumference (WC) (at the top of the iliac crests, standing position, with abdomen relaxed) of participants was measured by well-trained examiners. We obtained the definition of MtS from the International Diabetes Federation. 27 Individuals were defined as having MtS when they had central obesity (WC of ⩾ 90 cm for Chinese men and ⩾ 80 cm for Chinese women) and any two of the following characteristics: increased triglyceride level of ⩾ 1.69 mmol/L or treatment for lipid abnormality; reduced high-density lipoprotein cholesterol (< 1.03 mmol/L in men, and < 1.29 mmol/L in women) or treatment for lipid abnormality; treatment for previously diagnosed hypertension; elevated fasting plasma glucose level of ⩾ 5.60 mmol/L or previously diagnosed type 2 diabetes mellitus.
Endoscopy and biopsy
The Evis Lucera Elite Video System (CLV-290 and CV-290, Olympus Medical, Tokyo, Japan) was used in conjunction with either the GIF-Q260, GIF-HQ290, or GIF-H290Z endoscopes with narrow-band images (Olympus Medical). Six experienced attending physicians performed the gastrointestinal endoscopy with the assistance of narrow-band images. In accordance with the Seattle protocol, biopsies were performed for the circumferential part of endoscopic-suspected esophageal metaplasia (ESEM). 28 Due to the lack of consensus on protocol for biopsies for noncircumferential ESEM, the physicians decided the sites and numbers of biopsies at mucosal tongues of noncircumferential ESEM (that is Prague C0Mx). All specimens were fixed in formalin for subsequent histological examinations. The definition of BE was based on the American College of Gastroenterology clinical guidelines. 3 BE was diagnosed based on the presence of salmon-colored mucosa in the tubular esophagus proximally extending up to 1 cm or more in the gastroesophageal junction with histological confirmation of intestinal metaplasia. 3 Short-segment BE was defined as less than 3 cm in length. 2
Statistical analysis
We used SPSS, Version 20.0 (SPSS Inc., Armonk, NY, USA) to perform the statistical analyses. The included variables were: sex; age; presence of GERD symptoms (yes or no); history of smoking (yes or no); alcohol intake (heavy alcohol drinking was defined as 8 or more drinks a week for women and 15 or more drinks a week for men); 26 hyperuricemia (serum uric acid level ⩾ 0.41 mmol/L); 29 BMI; WC; MtS. Chi-square tests for categorical variables and independent t tests for continuous variables were used in the univariate analysis to evaluate the association between each variable and the prevalence of BE. Variables with a p value of < 0.1 in the univariate analysis were assessed using a binary logistic regression analysis with a forward stepwise method used in the multivariate analysis. In addition, we assessed the effect of cumulative smoking (pack-years) on BE risk in a multivariate model. We considered a p value of < 0.05 as statistically significant.
Results
Of the 4943 participants, 88 (1.8 %) had BE. BE’s mean length was 1.68 ± 0.89 cm. Short-segment BE accounted for 84.1% (74/88). The participants had a mean age of 40.5 years, and male participants comprised 51.4% of the study population. As shown in Table 1, the participants with BE were older, predominantly men, and had a higher BMI and WC. In addition, the presence of GERD symptoms, history of smoking, heavy alcohol drinking, MtS, and hyperuricemia were more common in the population with BE than without. The unadjusted odds ratios (ORs) of the aforementioned factors are presented in Table 2. Variables with a p value of < 0.1 in the univariate analysis were examined using collinearity diagnostics. WC and BMI had collinearity. Therefore, we applied two models in the logistic regression analysis (presented as model 1a and model 1b in Table 2). The two models showed the same results in that the following features were significantly associated with BE in young adults: male (adjusted OR: 2.03; 95% confidence interval [CI]: 1.20–3.45; p = 0.008); presence of GERD symptoms (adjusted OR: 2.06; 95% CI: 1.27–3.32; p = 0.003); history of smoking (adjusted OR: 2.19; 95% CI: 1.38–3.47; p = 0.001).
Demographic characteristics of participants with and without Barrett’s esophagus.

BE, Barrett’s esophagus; BMI, body mass index; DM, diabetes mellitus; GERD, gastroesophageal reflux disease; HDL, high-density lipoprotein; MtS, metabolic syndrome; WC, waist circumference.
Factors associated with Barrett’ esophagus according to the univariate and multivariate binary logistic regression analyses.

Variables with p < 0.1 were assessed using a binary logistic regression analysis.
Model 1a: adjusted for age, sex, presence of GERD symptoms, history of smoking, alcohol intake, WC, MtS, and hyperuricemia.
Model 1b: adjusted for age, sex, presence of GERD symptoms, history of smoking, alcohol intake, BMI, MtS, and hyperuricemia.
Model 2: adjusted for age, sex, presence of GERD symptoms, cumulative smoking, alcohol intake, WC, MtS, and hyperuricemia.
BMI, body mass index; CI, confidence interval; GERD, gastroesophageal reflux disease; OR, odds ratio; MtS, metabolic syndrome; WC, waist circumference.
In addition, we determined the relation between cumulative smoking (pack-years) and BE using a forward logistic regression model (presented as model 2 in Table 2). Nonsmokers were used as the reference group. Participants who smoked 10–20 pack-years (adjusted OR: 1.89; 95% CI: 1.03–3.46; p = 0.040) and more than 20 pack-years (adjusted OR: 4.09; 95% CI: 2.29–7.29; p < 0.001) had a significantly higher risk of BE, with the association strengthening with cumulative exposure to smoking (p trend < 0.001).
We performed a subgroup analysis separated by sex. The prevalence of BE was 2.6% (66/2541) and 0.9% (22/2402) in male and female participants, respectively. In male participants, the following two factors were significantly associated with BE in the multivariate analysis: the presence of GERD symptoms (adjusted OR: 2.70; 95% CI: 1.60–4.55; p < 0.001); cumulative smoking (adjusted OR: 4.27; 95% CI: 2.33–4.55; p < 0.001 for > 20 pack-years; adjusted OR: 2.12; 95% CI: 1.11–4.03; p = 0.022 for 10–20 pack-years; adjusted OR: 0.93; 95% CI: 0.35–2.49; p = 0.891 for < 10 pack-years) (Table 3). The proportion of BE in male participants with both GERD symptoms and a smoking history of 10 pack-years or more was 10.3% (16/155). In female participants, MtS was associated with BE after adjusting for WC or BMI (collinearity) and cumulative smoking (adjusted OR: 2.85; 95% CI: 1.04–7.79; p = 0.042) (Table 4).
Factors associated with Barrett’ esophagus in male participants.

Variables with p < 0.1 were assessed using a binary logistic regression analysis.
BE, Barrett’s esophagus; BMI, body mass index; CI, confidence interval; GERD, gastroesophageal reflux disease; OR, odds ratio; MtS, metabolic syndrome; WC, waist circumference.
Factors associated with Barrett’ esophagus in female participants.

Variables with p < 0.1 were assessed using a binary logistic regression analysis.
Model 1c: adjusted for cumulative smoking, WC, and MtS.
Model 1d: adjusted for cumulative smoking, BMI, and MtS.
BE, Barrett’s esophagus; BMI, body mass index; CI, confidence interval; GERD, gastroesophageal reflux disease; OR, odds ratio; MtS, metabolic syndrome; WC, waist circumference.
Discussion
There is a limited number of studies on BE in young adults. To our knowledge, this is the first large-scale retrospective cross-sectional study to determine the risk factors of BE in young adults and the first to evaluate the association between cumulative smoking (pack-years) and BE in an Asian population. In this study, the prevalence of BE in adults aged less than 50 years was 1.8%, which is slightly higher than that in other regions of Asia (0.7–1.1%).13,14 However, the prevalence was still much lower than that in a European population (8.7%). 15 Ethnicity, differences in the study population, and different definitions of BE might be contributing factors for the differences. 30 In general, risk factors for BE were male sex, the presence of GERD symptoms, and smoking.1–3 Such associations were also observed in young adults in the present study. Furthermore, consistent with earlier study results, we found that the association between BE and smoking strengthened with cumulative exposure to smoking.25,31,32 However, the precise mechanism linking smoking and BE remains unclear. Recently, Kaz and colleagues reported an association between smoking and DNA methylation in the esophagus, increasing the risk of BE. 33 In addition mechanisms caused by smoking include stimulation of gastric acid secretion, decreased lower esophageal sphincter pressure, and impaired acid clearance from the esophagus.34,35 Hence, future studies are needed to investigate the role of smoking on the mechanisms of BE development.
BMI was thought to be positively associated with BE. 36 However, in several recent studies, the correlation became weaker when simultaneously evaluating WC or waist-to-hip ratio, which are measures of central obesity.36–38 A possible explanation is that the relation between central obesity and BE was independent of GERD symptoms and that central adiposity produces proinflammatory cytokines, which could cause inflammation and stimulate BE development. 38 However, we observed no significant associations between WC and BE in the present study. Ethnicity and the type of BE may be contributing factors. Kramer and colleagues revealed that the association between a high waist-to-hip ratio and BE was only observed in White men, not in Black or Hispanic men, and a high waist-to-hip ratio was not linked to an increased risk of short-segment BE. 18 Such findings were similar to our results because most participants (84.1%) in our study had short-segment BE. Short-segment BE represents the most common type of BE in Asia. 2 Hence, as shown in the additional studies performed in Japan and Taiwan, central obesity might be not a risk factor for BE.19,20,39 Overall, these findings suggest the need to investigate the associations and mechanisms of BE, particularly in different races and types of BE, that are caused by central adiposity. On the other hand, similar to other studies, we also observed that alcohol consumption was not associated with BE.21,22
Our findings demonstrated that the presence of GERD symptoms and smoking were significantly associated with BE in male participants. They also represented the risk factors of progression to EAC from BE.40,41 The proportion of BE in male participants with both GERD symptoms and a smoking history of 10 pack-years or more was as high as 10.3% (16/155) in the present study. It could be considered to suggest endoscopic screening for BE in the group. MtS was linked with BE in female participants in our study. The association between MtS and BE had been previously reported.17,42,43 The possible mechanism that was previously proposed was that increased levels of circulating proinflammatory cytokines, serum insulin, and insulin-like growth factors may play a role in BE pathogenesis.43,44 However, the association between MtS and BE was not found in male participants. To our knowledge, literature assessing whether there is a gender difference in the association between BE and MtS is lacking. A previous study by Drahos and colleagues demonstrated that the association between MtS and esophageal adenocarcinoma was stronger in women (OR: 1.44; 95% CI: 1.20–1.73) than in men (OR: 1.09; 95% CI: 0.99–1.20). 45 Owing to the relatively fewer cases of BE in women in this study, we performed an analysis that enrolled individuals older than 50 years who underwent upper gastrointestinal endoscopy in our health examination center during the same study period (Supplemental Figure 1). We used the same study methods to analyze this population. In the participants aged 50 years or older, the association between BE and MtS was also observed only in women, not in men (Supplementary Tables 1–3). These results revealed that there is a gender difference in the association between BE and MtS regardless of age in the present study. However, why the association between MtS and BE was only noted in women remains unknown. BE is considered a chronic inflammatory condition. Rudnicka and colleagues reported that associations between inflammatory biomarkers and MtS were more obvious in women than in men. 46 Such findings may imply a gender difference in the MtS-induced inflammation. Further studies are necessary to clarify the association and mechanism between MtS and BE stratified by sex.
This study has some limitations. Being a retrospective cross-sectional study, there may be recall or information bias. For example, we did not have information on the duration and intensity of GERD symptoms, the previous history of BE, and medications history (such as proton-pump inhibitors, anti-reflux medicine, and medication with gastric irritants). Although the role of medical therapy on the regression of BE remains inconclusive, 47 the prevalence of GERD symptoms might be under- or overestimated. Furthermore, the number and location of endoscopic biopsies influence the detection rate of BE when performed by different physicians. 48 In this study, it is difficult to clarify the rate of accurate biopsy procedure. However, our well-experienced physicians assisted by narrow-band images could reduce the bias as much as possible. Moreover, there were relatively fewer cases of BE in women in the study, which may have failed to detect certain risk factors in this group; however, the data may demonstrate that the prevalence of BE in young women is very low.
Conclusion
Significant risk factors of BE in young adults are male sex, the presence of GERD symptoms, and smoking. Furthermore, the risk of BE increases with an increase in cumulative exposure to smoking. We suggest young men with GERD symptoms and smoking history of 10 pack-years or more to consider endoscopic screening for BE. However, further studies on the progression from BE to cancer in this population and a cost-effectiveness analysis of endoscopic screening are necessary.
Supplemental Material
Supplementary_Table_figure – Supplemental material for Risk factors for Barrett’s esophagus in young adults who underwent upper gastrointestinal endoscopy in a health examination center
Supplemental material, Supplementary_Table_figure for Risk factors for Barrett’s esophagus in young adults who underwent upper gastrointestinal endoscopy in a health examination center by Pin-Chieh Wu, Yan-Hua Chen, Fu-Zong Wu, Kung-Hung Lin, Chiao-Lin Hsu, Chi-Shen Chen, Yu-Hsun Chen, Po-Hsiang Lin, Guang-Yuan Mar and Hsien-Chung Yu in Therapeutic Advances in Gastroenterology
Footnotes
Acknowledgements
We are grateful to the members of the health examination center for their excellent work and thankful to Chao-Hsien Lee Ph.D for his statistics assistance.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The authors declare no conflicts of interest in preparing this article.
Ethics approval
The study was approved by the Ethics Committee of the Kaohsiung Veterans General Hospital (VGHKS18-CT11-03, VGHKS19-CT5-05).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.