
Abstract
Fecal microbiota transplantation (FMT) has changed the treatment landscape of Clostridium difficile infection (CDI). Emerging evidence has shown that FMT can also be an effective and safe treatment strategy in CDI with underlying inflammatory bowel disease (IBD). Recently, randomized controlled trials of FMT in ulcerative colitis support its expanding role in restoring gut homeostasis in this disease. However, heterogeneous study designs leave several questions yet to be answered, including how to best position this novel therapy in the treatment approach of Crohn’s disease and pouchitis. Additional studies are needed to validate whether FMT can assume a complementary role in the standard treatment of IBD.
Introduction
Inflammatory bowel disease (IBD), comprising ulcerative colitis (UC) and Crohn’s disease (CD), is a chronic, relapsing and remitting, destructive disorder of the gastrointestinal (GI) tract. In UC, inflammation occurs in a continuous pattern in the colonic mucosa. 1 In CD, inflammation is transmural with a discontinuous distribution, involving any part of the GI tract, but primarily the terminal ileum and colon. By the nature of its penetrating damage, CD can be complicated by fibrosis, stenosis, fistulae or abscesses. 2
The pathophysiology of IBD is complex and its etiology remains incompletely understood. Prior models of IBD proposed that the pathogenesis was multifactorial, involving a dysregulated immune response to environmental factors in a genetically susceptible individual. 3 More recent concepts of IBD pathophysiology additionally recognize the critical role of the gut microbiota in IBD. 4
Intestinal dysbiosis, characterized by reduced gut biodiversity and disrupted microbial function, has been repeatedly demonstrated in IBD. A healthy gut microbiota is characterized by an abundance of two major phyla, Firmicutes and Bacteroidetes. 5 These anaerobic bacteria are significantly reduced in IBD, including the commonly reported underrepresentation of Faecalibacterium prausnitzii. 6 F. prausnitzii, a butyrate-producing Firmicute, has been shown to be protective against host mucosal inflammation via immunomodulatory effects on inflammatory cytokines.7,8 The IBD microbiome is also characterized by an increase in facultative anaerobes, including the phyla Actinobacteria and Proteobacteria, such as Escherichia coli. 9
Alterations to the gut microbiota have been closely linked to intestinal inflammation in IBD.10,11 Substantiating this relationship are animal models demonstrating that transfer of pro-inflammatory bacteria into healthy mice or microbiota from diseased mice into healthy mice can induce gut inflammation.12–15 Fittingly, measures to correct dysbiosis, such as fecal microbiota transplantation (FMT), have emerged as potential therapeutic approaches in IBD.
FMT is the inoculation of minimally manipulated microbiota from healthy donors to affected patients, with the goal of correcting dysbiosis and restoring gut flora homeostasis. This therapeutic approach has been shown to be incredibly successful in treating recurrent Clostridium difficile infection (rCDI), another disease in which dysbiosis is thought to play a dominant pathogenic role. In the general population, multiple meta-analyses and systematic reviews have shown the efficacy of FMT for recurrent CDI to approach 90%.16,17 The efficacy and safety of FMT in IBD is less established, but emerging data support a potential increased role in these diseases.
Here, we review the current evidence on the use of FMT in IBD, focusing on efficacy and safety of this novel therapy, and continuing areas of study in this evolving field.
FMT in IBD patients with CDI
Clostridium difficile infection has become a rapidly growing problem in IBD. CDI incidence has doubled in CD and tripled in UC.18,19 Compounding this problem, IBD patients have 4.5-fold higher risk of CDI recurrence after antibiotic treatment, and have an 8-fold higher risk of toxigenic C. difficile carrier state compared to non-IBD patients, which may be an indicator of disease severity. 20 Overall, IBD patients have a 10% lifetime risk of CDI. 19
Standard anti-CDI antimicrobial agents are generally effective in IBD patients, particularly when given early in the disease course. Although the evidence for FMT in rCDI in the setting of IBD is less substantial, recent advances in FMT are changing the treatment paradigm in this at-risk population. In addition to several smaller reports, there have been three large retrospective studies of FMT for rCDI in patients with concurrent IBD.20–22 Unfortunately, heterogeneous study designs limit our ability to critically compare FMT outcomes in these studies. However, in the largest multicenter retrospective cohort study to date, Fischer and colleagues 20 observed a 79% CDI cure rate after initial FMT and 90% cumulative cure rate following a second FMT. All 67 IBD patients (35 CD, 31 UC, 1 indeterminate colitis) received FMT for recurrent or refractory CDI via sigmoidoscopy or colonoscopy. Following FMT, IBD activity was reported as worse in 13% of patients and no severe adverse effects directly attributable to FMT were found, supporting its tolerability in IBD. Reports of flare rates or worsening of IBD post-FMT in this setting are variable; however, all the data collected in this space are retrospective. Currently, there is a prospective trial assessing the safety and efficacy of FMT at clearing CDI in IBD patients, but will also be assessing IBD outcomes more systematically (ClinicalTrials.gov identifier: NCT03106844).
Recent advances in FMT continue to support an expanded role for CDI in the setting of IBD; however, patient selection remains critical to improving treatment outcomes. First and foremost to selecting FMT candidates is establishing the presence of true CDI. Differentiating active IBD versus concomitant CDI with IBD can be challenging due to overlapping symptoms and the rising prevalence of C. difficile colonization in IBD. Accordingly, we recommend adoption of the two-step diagnostic approach supported by the European Society of Clinical Microbiology (ESCMID). 23 This incorporates a highly sensitive test, either glutamate dehydrogenase (GDH) immunoassay or polymerase chain reaction (PCR) test, followed by the highly specific ELISA-based toxin A/B immunoassay.
The status of underlying IBD at the time of FMT also appears to impact FMT outcomes. 15 Specifically, IBD patients with more active disease at the time of FMT are more likely to have post-treatment flare or require IBD treatment escalation. Thus, a comprehensive clinical and mucosal assessment at the time of FMT is essential. Additional benefits of colonoscopy or sigmoidoscopy at the time of FMT include the convenience of co-administration of the fecal preparation and the establishment of an objective mucosal baseline in cases of post-FMT flare. 15
FMT for the treatment of IBD
Ulcerative colitis
To date, four randomized controlled trials (RCTs) have investigated FMT for UC, which include a total of 277 patients (Table 1). Overall, 28% (39/140) of UC patients who received donor FMT achieved clinical remission compared to 9% (13/137) of patients who received placebo (OR = 3.65, 95% CI: 1.85–7.22, p = 0.0002). Clinical response was achieved in 49% (69/140) of patients who received donor FMT and in 28% (38/137) of patients who received placebo (OR = 2.53, 95% CI: 1.54–4.17, p = 0.0003). Endoscopic remission, defined as an endoscopic Mayo score of zero, was observed in 14% (20/140) of FMT recipients compared to 5% (7/137) of those who received placebo (OR = 2.69, 95% CI: 1.07–6.74, p = 0.04, I2 = 0%).24–28
Summary of randomized controlled trials of FMT in UC.
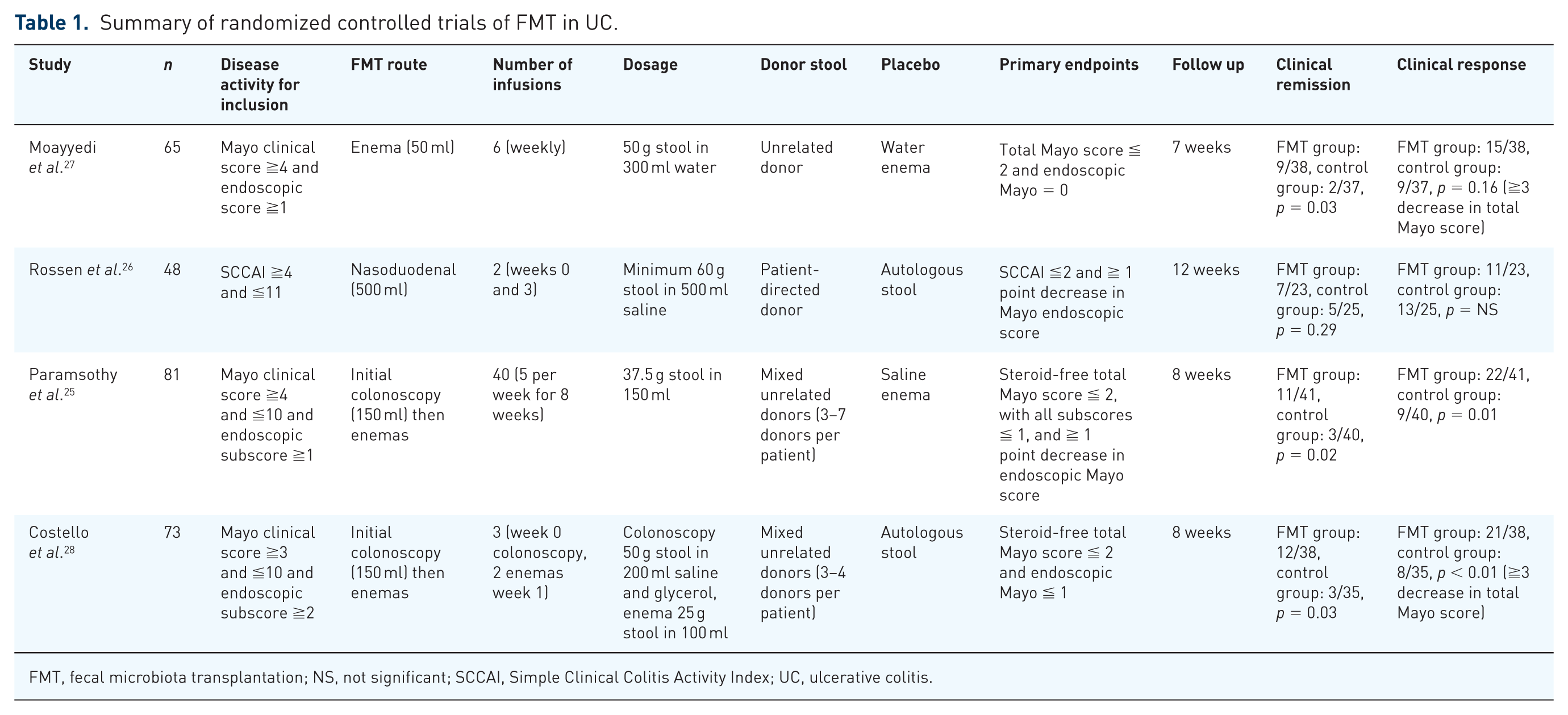
FMT, fecal microbiota transplantation; NS, not significant; SCCAI, Simple Clinical Colitis Activity Index; UC, ulcerative colitis.
As demonstrated in a recent meta-analysis by Paramsothy and colleagues, which included 20 uncontrolled cohort studies (n = 307) in addition to the above RCTs, the pooled proportion of UC patients achieving remission was 33% (95% CI: 23–43%, p = 0.001) with moderate risk of heterogeneity (I2 = 54%). The pooled proportion of UC patients achieving clinical response was 52% (95% CI: 40–64%, p = 0.001, I2 = 58%). 24 Combined, these studies suggest that FMT may be an effective treatment option for not only achieving clinical response but also for inducing clinical remission.
Crohn’s disease
The evidence for FMT as treatment for CD is less robust. While there are several clinical trials underway, published data are limited to uncontrolled cohort studies and case reports. A meta-analysis of six cohort studies (Table 2), consisting of 71 CD patients, reported clinical remission in 52% (95% CI: 31–71%, p = 0.063, I2 = 52%) of patients receiving FMT. Clinical response was achieved in 63% (95% CI: 30–88%, p = 0.016, I2 = 71%) of 59 CD patients in the four cohort studies. 24 Only one of the above studies reported endoscopic remission, occurring in none of six patients. 29 Drawing conclusions about the potential role for treating CD with FMT is not currently possible due to the lack of high-quality data. The heterogeneous nature of CD poses an additional challenge as the benefit of FMT may not be seen across all phenotypes. We hypothesize that FMT may prove to be more effective in inflammatory Crohn’s colitis and perhaps in early postoperative recurrence, and less so for penetrating complications such as fistulae or strictures. Future studies will need to address this issue while determining whether FMT should be included within the management strategy for CD.
Summary of cohort studies of FMT in CD.

CD, Crohn’s disease; HBI, Harvey Bradshaw Index; CDAI, Crohn’s Disease Activity Index; FMT, fecal microbiota transplantation; PCDAI, Pediatric Crohn’s Disease Activity Index; SES-CD, Simple Endoscopic Score for Crohn’s Disease; NR, not recorded.
Pouchitis
Similar to observations made in UC and CD, decreased microbial diversity has been linked to the pathogenesis of pouchitis. Efficacy of antibiotic therapy in pouchitis underscores the crucial role of pouch bacteria in the disorder; however, antibiotic refractory disease is common.35,36 Accordingly, there have been three prospective uncontrolled cohort studies evaluating FMT in pouchitis (Table 3). In the two studies that used a single FMT inoculation, no patients (0/19) achieved clinical remission, and clinical response varied widely (25–63%). In the third study, in which multiple FMT treatments were employed, 80% (4/5) achieved clinical remission with the remaining patient attaining clinical response. 37 These preliminary results, while limited, are encouraging and will need to be replicated in larger controlled trials to validate FMT use in pouchitis.
Summary of cohort studies of FMT in pouchitis.

FMT, fecal microbiota transplantation; PDAI, Pouchitis Disease Activity Index; NR, not recorded.
FMT methodology
Delivery route and dosing frequency
Delivery protocols for FMT infusions in IBD studies remain poorly standardized and the optimal route is uncertain. The route of FMT delivery is an important consideration as it may impact outcomes. FMT via colonoscopy allows for direct inoculation of donor stool to the affected area, but it carries the inherent risk of endoscopy. Upper GI tract administration (nasogastric, nasoduodenal or nasojejunal tube) may not be ideal in IBD as it delivers donor stool far away from the inflamed bowel, and could be impacted by proximal gut secretions, but it may be safer in frail patients who are not suitable for endoscopy. Importantly, it is recommended that patients be kept upright for up to 4 h after the upper GI infusion to reduce the risk of aspiration. 40
Prior reviews have suggested that colonoscopy may be superior to upper GI administration for FMT delivery.15,24 These suggestions should be interpreted with caution, as the number of infusions varied greatly between studies, potentially confounding results. Alternatively, frozen or gelatin-covered fecal capsules offer an attractive option for FMT delivery and clinical trials are underway to determine their efficacy in treating IBD. If effective, the safety profile of capsules and their potential for improving patient accessibility to FMT would suggest that they may eventually become the preferred route for FMT.
As for the frequency of the FMT infusions, it is reasonable to expect that multiple administrations will be needed to achieve lasting therapeutic effect. This is reflective of the chronic dysbiosis in IBD, and is in contrast to the dysbiosis associated with CDI, which is often overcome with a single FMT infusion. Expectedly, published subgroup analysis of UC cohort studies demonstrated that patients who received a higher number of FMT infusions (>10) were more likely to achieve remission (49%) compared to UC patients who received fewer than 10 infusions (27%, 95% CI: 17–40%, p = 0.001, I2 = 58%). 24
Donor selection
The optimal donor stool profile is an area of great interest. Donor stool sources have yet to be standardized and thus donor microbial composition varies significantly, potentially impacting FMT efficacy. Commercial stool banks offer the benefit of accessing a large unrelated donor database. In theory this may offer greater collective alpha diversity compared to stool from healthy related donors, as related stool donors may be at risk for decreased biodiversity by living in similar environmental conditions as the FMT recipient. Additionally, it is not known whether individual donor versus pooled multi-donor stool protocols translate to more effective reestablishment of microbial homeostasis. Importantly, while the Paramsothy and Costello UC RCTs used multi-donor stool, the majority of IBD FMT studies have used individual donor stool, and the FDA currently requires that only individual donors be used in RCTs. Interestingly, FMT studies in UC suggest a “super donor” phenomenon exists. Moayyedi and colleagues reported that the majority of treatment benefit observed was linked to an individual donor (Donor B). 27 Similarly, Paramsothy and colleagues reported that 37% of UC patients who received pooled FMT containing stool from Donor 54 (n = 38) achieved the primary outcome, compared to only 18% (n = 40) in patients who did not receive pooled stool including that donor (p = 0.054). 25
Although neither study was powered to detect a true donor effect, they offer potential insight to future donor selection targets. Specifically, greater microbial richness alone may not be sufficient to induce remission. It may be that the extent to which donor–recipient bacterial phyla profiles complement each other influences host engraftment and predicts FMT benefit. Therefore, specific donor microbial compositions may be required to facilitate alteration of mucosal immune response. Supporting this assertion, a recently published trial of intensive multi-donor FMT demonstrated that increased abundance of specific species of Bacteroides (B. fragilis and B. finegoldii) in donor stool was associated with remission in patients receiving FMT, whereas Streptococcus was associated with no response to FMT. 41 Advancing our understanding of both donor and recipient microbiota using deep molecular characterization may help further clarify which donor features are associated with remission, and improve our ability to match donor microbiota to the appropriate beneficiary.
Patient selection
There is currently insufficient data to determine which IBD patients will benefit most from FMT. Subgroup analysis from Moayyedi and colleagues suggests that FMT may be more effective in UC when performed early in the disease course or in less severe colitis. 27 Nevertheless, there are multiple reports of successful FMT in severe and steroid-dependent UC.42,43 Fulminant colitis may be less likely to benefit from FMT, as it is inherently treatment-resistant.
While limited data exist, disease extent in UC does not appear to be predictive of achieving remission following FMT. Additionally, which CD phenotype might benefit from FMT remains unknown. 27
Safety
FMT is generally well tolerated, with the majority of studies not reporting serious adverse events. In a large study of IBD patients who underwent FMT for CDI, Fischer and colleagues reported that post-FMT IBD flare occurred in a minority of patients and no severe adverse effects directly attributable to FMT were observed. 20 Furthermore, a meta-analysis by Qazi and colleagues demonstrated that marginal risk of flare in high-quality studies and RCTs. 44 Commonly reported complications in IBD trials of FMT include bloating, diarrhea, abdominal pain or fever, which are often self-limiting.34,42,45,46 Additionally, rigorous donor-screening protocols limit the risk of transmissible diseases. However, there is a theoretical risk of cytomegalovirus (CMV) and Epstein–Barr virus (EBV) transmission or reactivation with FMT in this high-risk population, yet they are not routinely screened for. Lastly, long-term safety data on FMT is lacking and will need to be explored further as the science matures.
Conclusion
Advances in IBD therapeutics, including new biologic classes and drug monitoring protocols, have drastically improved how we treat UC and CD over the past decade. Despite these steps forward, disease control remains elusive for many patients. The increasing recognition of microbial imbalance in the pathogenesis of IBD has propelled FMT into the conversation of potential novel therapies. The rapidly progressing evidence for FMT in IBD is promising, but at this time it is not sufficient to support the routine use of FMT in IBD. Looking forward, as the science of FMT is refined through upcoming trials, our hope is that FMT will achieve a complementary role in standard IBD therapy and potentially usher personalized therapy into IBD treatment algorithms.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
JRA consults for and has research support from Finch Therapeutics Group. ANL has no conflicts of interest.