
Abstract
Background:
Somatostatin analogues (SAs) reduce liver volume and relief symptoms in polycystic liver disease (PLD). Its effect wears off after continuing therapy suggesting development of SA tolerance in patients on chronic therapy. We postulate that a drug holiday resensitizes the liver to its acute pharmacological effects. Therefore, this study examines the liver volume-reducing effect of SAs after a drug holiday.
Methods:
Patients were identified from the International PLD Registry and included in our analysis when (1) treated with SAs during two cycles separated by a drug holiday and (2) height-adjusted total liver volume (hTLV) was available at start and end of each cycle. For our primary outcome we compared the effect of SAs (in % per 6 months) on hTLV between the first and second treatment cycle.
Results:
In 34 patients, initial liver volume-reducing effect was similar to that after rechallenge [−2.6% per 6 months (interquartile range, −3.8–0.8) versus −1.6% per 6 months (interquartile range, −3.1–1.1), p = 0.510]. Cessation of treatment led to a rebound effect, but liver volume remained stable compared with the baseline with intermittent therapy in responders to SA [−0.6% (interquartile range, −7.4–5.7) after 46.5 months].
Conclusions:
PLD patients treated with SAs benefit from retreatment after a drug holiday. The significant increase of liver volume after cessation of treatment complicates widespread use of a drug holiday as new treatment strategy. Our results contribute to a better understanding of the pharmacological effect of SAs and help to identify patients who might benefit.
Introduction
Polycystic liver disease (PLD) is a rare hereditary disorder characterized by the formation of multiple cysts in the liver. Development of liver cysts is the primary presentation in patients with autosomal dominant polycystic liver disease (ADPLD), and the most frequent extra-renal manifestation in patients with autosomal dominant polycystic kidney disease (ADPKD). 1 PC-1 deficiency, caused by genetic mutations, plays a defining role in liver cystogenesis. It leads to decreased intracellular calcium levels, cAMP activation and subsequent cell proliferation and fluid production. 2 Although the majority of PLD patients remain without symptoms, patients with severe hepatomegaly could develop severe mechanical symptoms and malnutrition. This category of patients is in need of treatment. 3
A growing body of evidence suggests that somatostatin analogues (SAs) possess a liver volume-reducing effect and alter the natural growth of the polycystic liver. SAs reduce cell proliferation and fluid production by inhibiting cAMP production in cholangiocytes. 4 In a pooled analysis from three randomized controlled trials, livers from patients on placebo grew by 1.8% whereas SAs for 6–12 months gave a decrease of 3.6%.5–8 Withdrawal of treatment led to a recurrence of the growth rate to values seen at the baseline.9,10
A study suggests that chronic SA therapy for symptomatic patients is warranted based on results of a placebo-controlled single-blind trial in which patients were successfully treated with SAs for 3 years. 10 However, the results of this study cannot be translated to all PLD patients and there are a number of potential issues that preclude widespread use of chronic SA therapy. One of the main issues is that the effect of the drug is mainly achieved in the first months of treatment and wears off beyond that. 9 This suggests that tolerance to SAs develops in patients on chronic therapy. Drug holidays, defined as an interruption of pharmacotherapy for a defined period of time, could be the answer to prevent the development of tolerance. Indeed, drug holidays have been hypothesized to ‘resensitize the system’ to the acute pharmacological effects for other types of drug.11,12 For instance, retreatment with chemotherapy is an established practice in many cancers such as lung cancer, gastrointestinal stromal tumours (GISTs) and renal cell cancer.13,14 Although PLD is a benign disease, we reasoned that rechallenge after a drug holiday might benefit PLD patients.
We examined the effect of SA rechallenge after a drug holiday and explored whether the benefit from treatment is related to the initial response to treatment, and whether the length of drug holiday affects treatment success. In addition, we compare natural growth before the start and after cessation of SA therapy to determine a rebound effect.
Methods
Patients and study design
The International PLD Registry, which consists of PLD patients with >10 liver cysts, allows us to explore these issues in a real-world cohort in which clinical data from individual patients are collected uniformly.15,16 Patients from two centers [Radboud University Medical Center (Nijmegen, The Netherlands) and University Hospital Leuven (Leuven, Belgium)] were evaluated for inclusion since these were the only centers with a history of SA prescription. Out of 741 patients, included in the International PLD Registry until December 2017, 231 patients were treated with SAs at least once. Selection for our study was based on the following inclusion criteria: (1) SA therapy-naïve PLD patients treated with any type of SA for two separate cycles with a drug holiday in between; (2) each cycle (either treatment or drug holiday) lasted at least 3 months; (3) minimum interval between consecutive imaging was 3 months; and (4) height-adjusted liver volume (hTLV) was available at the start and end of each cycle (either treatment or drug holiday) and measured with computed tomography (CT) or magnetic resonance imaging (MRI). Selected patients were treated with SAs in regular clinical care or they participated in prospective clinical trials.6,9,17–19 All imaging in clinical trials and regular clinical care was performed according to standard protocols. The majority of patients received lanreotide 120 mg subcutaneously or octreotide 40 mg intramuscular every 28 days. In some patients, dose escalation occurred, especially in the second treatment cycle (Table S2, supplementary files).
For our primary research question, we compared the effect of SAs on hTLV in two treatment cycles (On-1 versus On-2) separated by a drug holiday (Off-1) to evaluate whether the volume-reducing effect of SAs is repeated. For our secondary research question, we aimed to compare natural liver growth before SA treatment (Off-0) with liver volume change during drug holiday (Off-0 versus Off-1) to evaluate whether a rebound effect occurs. Therefore, we included all patients in whom hTLV was available before the start of the first treatment cycle. Figure 1 illustrates the design of our study.

Study design.
For both research questions we excluded patients in case imaging was performed >2 months after the start or end of SA therapy as this might underestimate the effect of SAs and the natural growth in the preceding drug-free period. Patients were also excluded who received other liver volume-reducing therapy during our observation period.
Data collection
The following data were extracted from the International PLD Registry; sex, age, height, weight, body mass index (BMI), etiology (ADPKD/ADPLD), date and type of imaging (CT/MRI), liver volume, treatment (type, dose and duration of treatment) and serious adverse events (SAEs). Liver volume was measured in the past as part of clinical trials or regular clinical care by assessing CT or MRI imaging using semi-automatic software; CT scans in Belgium were measured with Volume (Siemens, Erlangen, Germany)18,20 and in the Netherlands with Pinnacle3® version 8.0 (Philips, Eindhoven, The Netherlands).21,22 Volumetry on MRI was performed with Analyze 11 software (AnalyzeDirect Inc). 23 Liver volume was divided by height to obtain hTLV.
Ethical consideration
Concerning ethical approval of the International PLD Registry and thereby these analyses, formal evaluation was waived by the Institute Review Board Committee on Research Involving Human Subjects Arnhem-Nijmegen given the retrospective character of the data collection in the PLD Registry. Ethical approval has been obtained for all clinical trials in which these patients participated in the past. This study was conducted in accordance with good clinical practice guidelines and the code of conduct for medical research (www.federa.org). No identifying patient data were collected, and all patient data were anonymously entered in the database.
Statistical analyses
Baseline characteristics were presented as mean [standard deviation (SD)] for normally distributed data, median [interquartile range (IQR)] for nonnormally distributed data and absolute numbers with percentages (%) for dichotomous variables. Outcomes were presented as percent change (%) and absolute change in hTLV (ml/m) and total liver volume (TLV; ml).
For our primary and secondary research questions we tested for differences between On-1 versus On-2 and Off-0 versus Off-1 respectively, using a dependent Student’s t-test for normally distributed data or Wilcoxon signed ranks test for nonnormally distributed data. As it was expected that duration of observation periods would follow a skewed distribution, total percent change in hTLV over a total period was calculated per 6 months [calculated as: ((ending value/beginning value) ᶺ (6/duration in months) −1) × 100)] to correct for these time differences, this being our primary outcome. To verify these results, we used generalized linear mixed models to correct for baseline differences in baseline hTLV and/or duration of treatment cycle, if necessary. A variable ‘patient identifier’ was included in our model as random effect to handle paired comparisons. Correlation between the duration of a drug holiday (Off-1) and the effect in Off-1 and On-2 was calculated with a Spearman’s correlation coefficient.
We performed a secondary analysis in order to determine the response chance after re-exposure to SA therapy. Responders were defined as having a decrease in hTLV per 6 months (<0% growth in hTLV) and nonresponders as having an increase in hTLV per 6 months (⩾0% growth in hTLV) during the first treatment cycle (On-1).
Subsequently, we performed an exploratory analysis to determine the response rate during the entire treatment period (On-1, Off-1, On-2) for the total group as well after stratification for responders and nonresponders in the first treatment cycle.
Finally, we repeated all analyses in an exploratory subgroup analysis by dividing our cohort based on disease severity. Patients were classified as mild (hTLV < 1600 ml/m), moderate (hTLV 1600–3200 ml/m), and severe (hTLV > 3200 ml/m).
A p-value of <0.05 was considered significant. Analysis were performed using SPSS 22.0 (SPSS Inc., Chicago, IL, USA).
Results
Of a total of 231 SA-treated patients, 53 patients were re-exposed to SAs during a second treatment cycle separated by a drug-free period. Ultimately 45 patients met our inclusion criteria (Figure 2). We included 34 patients for our primary objective, 11 patients were excluded because imaging (i.e. hTLV) was performed ⩾2 months after start of treatment. A total of 25 patients could be included for our secondary objective. The main reason for exclusion was that no hTLV was available before the first treatment cycle (NOT-0 missing, n = 14; Figure 1).

Flowchart of patient selection.
Primary objective
Change in hTLV between On-1 and On-2
The majority of patients were female (88.2%) and diagnosed with ADPKD (61.8%). The mean age was nearly 48 years (SD 7.8) at the start of first SA treatment (BOT-1; Table 1). The baseline liver volume was significantly lower at the start of On-1 (BOT-1) compared with On-2 (BOT-2) whereas the duration of both treatment cycles was similar. In On-1, hTLV decreased with −2.6% (IQR −3.8–0.8) per 6 months compared with −1.6% (IQR −3.1–1.1) in On-2 which was not significantly different [p = 0.510; Table 2 and Figure 3(a)]. These findings were confirmed after correction for baseline liver volume, treatment duration and treatment center using generalized linear mixed models (p = 0.253). The absolute change in hTLV was similar between On-1 (−75 ml/m) and On-2 (−70 ml/m, p = 0.263). There was a significant correlation between the duration of the drug holiday and effect of SAs in On-2, with improvement of the liver volume-reducing effect when longer off treatment (r = −0.298, p = 0.016).
Characteristics of study population (primary objective).
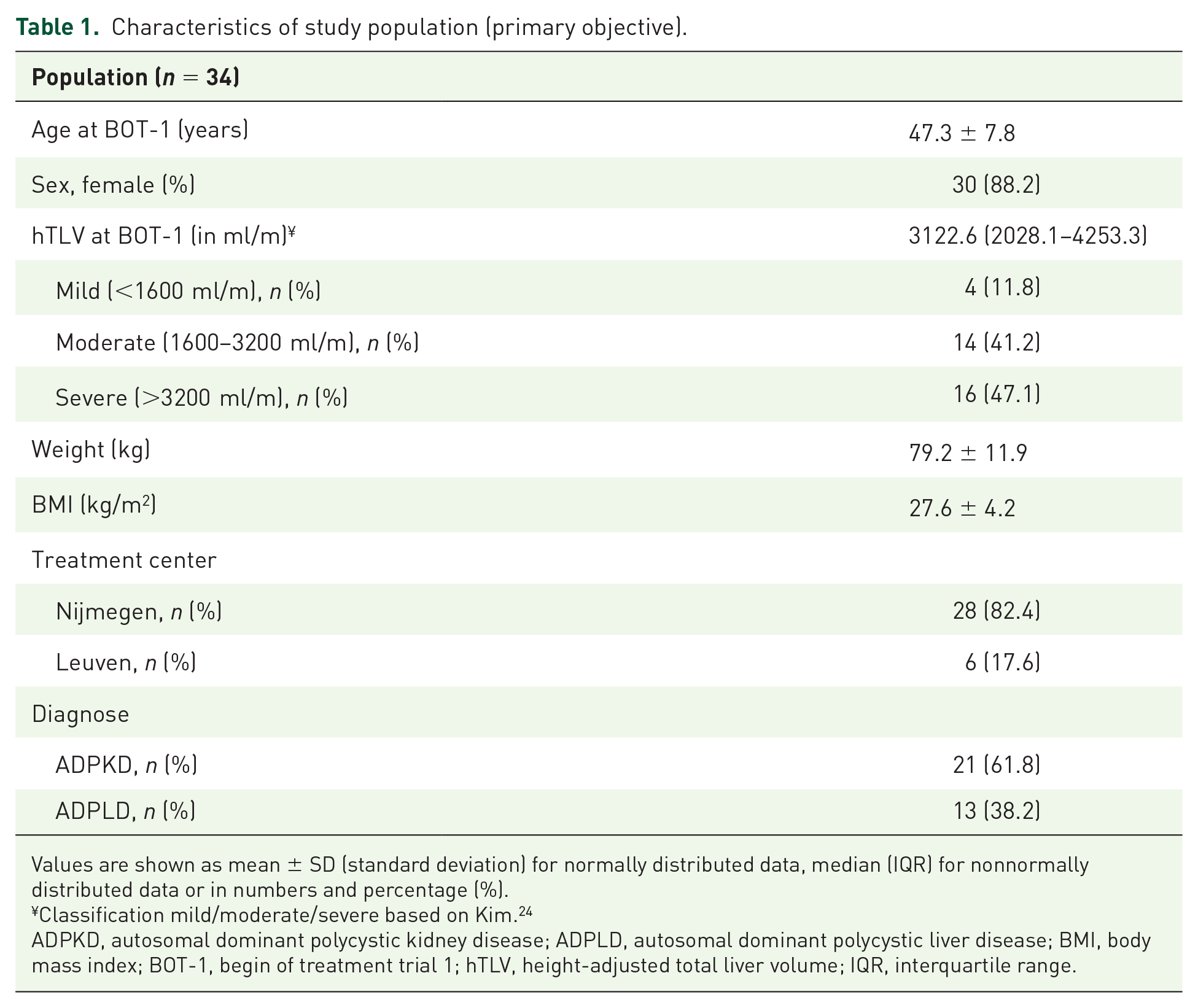
Values are shown as mean ± SD (standard deviation) for normally distributed data, median (IQR) for nonnormally distributed data or in numbers and percentage (%).
Classification mild/moderate/severe based on Kim. 24
ADPKD, autosomal dominant polycystic kidney disease; ADPLD, autosomal dominant polycystic liver disease; BMI, body mass index; BOT-1, begin of treatment trial 1; hTLV, height-adjusted total liver volume; IQR, interquartile range.
Outcomes of primary (n = 34) and secondary objective (n = 25).

Values are shown as median (IQR).
p-values were calculated using Wilcoxon signed rank test.
hTLV, height-adjusted total liver volume; IQR, interquartile range; TLV, total liver volume.

Primary and secondary outcome. (A) Percentage change in hTLV per 6 months between On-1 and On-2. (B) Change in hTLV per 6 months between Off-0 and Off-1. Data are presented as a median with interquartile range.
There was no difference in serious adverse events (SAEs) between On-1 (n = 1; cyst infection) and On-2 (n = 2; cyst infection and cyst bleeding). No other SAEs were described during SA treatment, such as formation of gall stones or diabetes mellitus de novo.
Responders versus nonresponders
In our secondary analysis, the first treatment with SAs resulted in a decrease of hTLV in 22 patients (64.7%) whereas in 12 patients, volume reduction was not achieved (nonresponse). The vast majority (86.4%) of responders in On-1 again showed a decrease in hTLV after re-exposure to SAs (On-2). In case of nonresponsiveness in On-1, re-administration of SAs still reduced hTLV in 33.3% of patients (Figure 4).

Responders versus nonresponders. Response is defined as a decrease in liver volume (<0%). Grey boxes represent nonresponders.
Secondary objective
Change in hTLV between Off-0 and Off-I
Baseline characteristics for this subgroup are shown in Table S1. hTLV at beginning of each drug-free period (NOT-0 and EOT-1) was not different. The observation time was significantly longer in Off-1 (18.6 months, IQR 13.9–24.0) compared with Off-0 (5.7 months, IQR 5.5–10.0, p = 0.012; Table 2). The increase in hTLV per 6 months was significant higher during the drug holiday (Off-1) compared with the natural growth (Off-0) before pharmaceutical intervention [4.5% versus 1.6%, p = 0.010; Figure 3(b)]. After correction for differences in duration using generalized linear mixed models, increase in hTLV per 6 months remained significant higher in Off-1 (p = 0.011), indicating a rebound effect. The duration of the drug holiday (Off-1) was positively correlated with hTLV growth (r = 0.461, p = 0.021).
Response during entire observational period
We determined the response rate during the entire observational period (On-1, Off-1, On-2) in 34 patients. Patients were treated with SAs 54.4% of the time and hTLV increased with 0.5% per 6 months (4% after 43.5 months). In the group of patients who responded in the first treatment cycle (On-1), hTLV decreased with 0.1% per 6 months (−0.6% after 46.5 months) whereas the livers of nonresponders grew with 1.9% per 6 months (+14.2% after 40.6 months). Nonresponders were treated with SAs relatively longer compared with responders (63.7% versus 53.1%; p = 0.034; Table 3).
Baseline characteristics stratified for responders and nonresponders.

Values are shown in absolute numbers (%) or median (IQR).
p-values are calculated between responders and nonresponders using Chi-square tests (absolute data) or independent-samples Mann–Whitney U test (continuous data). p < 0.05.
Total observation period consists of On-1 + Off-1 + On-2.
ADPKD, autosomal dominant polycystic kidney disease; ADPLD, autosomal dominant polycystic liver disease; BOT1, begin of treatment trial 1; EOT-2, end of trial 2; hTLV, height-adjusted total liver volume; IQR, interquartile range.
Disease severity
We divided patients into two groups based on baseline hTLV at the start of the first treatment cycle: mild or moderate PLD (18 patients, hTLV <3200 ml/m) and severe PLD (16 patients, hTLV >3200 ml/m). Both in On-1 and On-2 there was no difference in liver volume-reducing effect per 6 months between the two subgroups. For our secondary objective we observed that semi-annual liver growth during drug holiday (Off-1) was significantly higher in the severe subgroup (6.2% versus 2.8%; p = 0.007). The evaluation of liver volume change in the entire observational period (On-1, Off-1, On-2) was 5.4% (IQR −5.9–23.4) per 6 months in the severe group and 1.4% (IQR −6.7–12.6) per 6 months in patients with mild/moderate PLD (p = 0.317; Table S3).
Discussion
In this study we show that PLD patients treated with SA-targeted therapy, who discontinue treatment, benefit from retreatment at a later stage. Patients with an initial good response, defined as a decrease in liver volume, are most likely to benefit again from SAs during subsequent treatment cycles. However, polycystic liver growth accelerates after cessation of therapy which complicates the widespread use of a drug holiday as a treatment strategy.
A major issue with SAs is that patients tend to become tolerant to therapy and lose the maximal benefits of medication after 6 months. Indeed, open-label studies showed that prolonged 12–24 months administration of SAs did not demonstrate beneficial effects in terms of liver volume decline as observed in the first months9,25 which speaks against the use of continuous therapy. The loss of effect beyond 6 months of therapy might be explained by desensitization or down-regulation of somatostatin receptors (SSTRs). SSTRs are expressed on normal and cystic cholangiocytes and these receptors are activated by SAs, leading to inhibition of cAMP and cell proliferation. 4 Several animal studies have provided evidence of SSTR down-regulation after prolonged somatostatin treatment (for other diseases), which might explain why patients become tolerant with time. Confirmation of this hypothesis is needed for PLD in human liver cells.26,27 Our study shows that the polycystic liver volume-reducing effect of SAs repeats after re-exposure, even after an initial treatment cycle of more than 6 months (median 11.3 months). We hypothesize that the expression of SSTR in these patients have been reset during a drug holiday. Further studies are needed to clarify the role of SAs on SSTRs expression in PLD patients during and after therapy.
In our cohort the length of the drug holiday was significantly associated with the effect size in terms of liver size reduction in the second treatment cycle. However, stopping therapy is associated with a rebound effect which is correlated with the duration of drug holiday. This potentially negates the beneficial effect of re-exposure. Earlier findings from another group reported similar rebound effect with liver growth by 9.7% 2 year after SA therapy and 4.9% in nontreated patients in a placebo-controlled trial (n = 27). 10 They also demonstrated that 3 years of treatment with octreotide followed by 2 years of follow up resulted in stabilization in liver volume (−0.8%) despite the rebound effect, whereas the livers of patients on placebo increased with 11.0% after 5 years. In our study, we saw that liver volume increased with 4% in 43.5 months after two treatment cycles with an intermittent drug holiday (54.4% of the observation time treated) with liver volume stabilization (−0.6%) in patients who responded to SAs in the first treatment cycle. One should realize that the study population of Pisani and colleagues 10 contained only ADPKD patients with mild PLD, whereas our study population contains both ADPKD and ADPLD patients with moderate/severe PLD with potential more liver volume progression. This could explain why significant liver reduction has not been detected during the treatment cycles. Nonetheless, results of both these studies suggest that in a subset of patients, treatment with SAs for only half of the time could result in overall stabilization of liver volume, especially for patients that respond well to initial SA therapy.
The findings of our subgroup analysis in which we divided patients based on PLD severity are explorative in nature and should be interpreted very carefully due to the low numbers in each subgroup. Nonetheless, it suggests that a ‘rebound effect’ during a drug holiday is more severe in patients with severe PLD. This raises the hypothesis that patients with mild/moderate disease might benefit the most from an intermittent treatment regime. Indeed, in our population proportional and absolute liver volume change in patients with mild/moderate PLD was less increased during the whole observational period. Possibly because of the large variety and small sample size no significance was detected. Further research is needed to confirm this hypothesis.
Our present analysis has inherent limitations associated with nonprospective studies such as variability in patient selection. Most patients received SA therapy during a clinical trial or protocolized standard care, which enabled collection of high quality data. The main reason for re-exposure to SAs was that patients participated in a second clinical trial. It is likely that patients who did not tolerate SAs during first exposure, were not willing to proceed to the subsequent trial. Although this might lead to selection bias, it corresponds with daily practice as nontolerable patients will not be treated. Furthermore, we were able to include both responders and nonresponders to SAs in our study which reduces potential selection bias. Secondly, the sample size of this cohort is small because of the rarity of PLD and the low frequency of SA prescription. Treatment with SAs in PLD has only been available for a couple of years which complicates obtaining a larger cohort that meets our inclusion criteria. Nonetheless, all patients from the International PLD Registry were screened and included when eligible. Third, we could not explore the effect of dosage, type of drug and etiology on our primary outcome because of lack of power. No studies directly compared the efficacy between octreotide and lanreotide, however multiple trials demonstrated comparable results for both types of SA. 5 The results in both treatment cycles seen on SAs in this study are in line with these trials. In a pooled analysis of four trials including treatment with lanreotide 120 mg or octreotide 40 mg for 6–12 months, SA type and underlying diagnose did not significantly interact with treatment effect. 28 One clinical trial explored alternative doses of lanreotide and found that both 90 mg and 120 mg reduce liver volume compared with placebo with numerically higher effect when exposed to 120 mg. 18 In the second treatment cycle of our study, five patients were treated with lanreotide 90 mg of which three patients had a dose escalation to 120 mg because of nonresponse after 6 months. In the first treatment cycle only one patient was treated with lanreotide 90 mg (with dose escalation to 120 mg). It is possible that a lower dosage masked the effect of treatment leading to underestimation of the liver volume-reducing effect of SAs in On-2 (Table S2).
A strength of our study is that independent assessment of liver size measurements was part of the treatment protocol. Although different quantification methods were used to measure liver volume, all of these methods are frequently used in trials and standard of care. Previous studies showed that the agreement between techniques and inter-observer variability is low which minimizes its potential effect on our results.6,18,21 Patients did not receive other treatment that may have affected the primary outcome of the study and as such the study results may be ascribed to the effect of SAs therapy.
The findings of this study are a prelude to further exploration of alternative SA treatment strategies and contribute to a better understanding of the pharmacological effect of SAs in PLD. Although the effect of SA therapy is reproducible, the rebound effect after cessation of treatment complicates the implementation of drug holidays. Our data fuel the evidence base for alternative approaches for physicians who might be anxious to discontinue therapy. For instance, it could be worthwhile to discontinue SA therapy in patients who become asymptomatic under treatment or for those who have a lower risk for significant liver growth (e.g. women who entered the menopause). Liver growth rate can be followed, and, in the case of accelerated liver growth, treatment can be resumed safely with high probability of response. This low-risk strategy potentially avoids needless continuous therapy (with possible loss of effect) and reduces medical costs. Second, these results afford a more granular picture of the effect after cessation or re-exposure to SAs. Third, in a subset of patients, intermittent treatment might be a potential strategy as it may lead to an overall stabilization of liver volume. Future research is needed to explore the effect of intermittent treatment on liver volume and symptoms and to identify those who might benefit from this regimen.
Supplemental Material
Supplementary_Material – Supplemental material for Drug holiday in patients with polycystic liver disease treated with somatostatin analogues
Supplemental material, Supplementary_Material for Drug holiday in patients with polycystic liver disease treated with somatostatin analogues by René M. M. van Aerts, Marieke Kolkman, Wietske Kievit, Tom J. G. Gevers, Frederik Nevens and Joost P. H. Drenth in Therapeutic Advances in Gastroenterology
Footnotes
Acknowledgements
The establishment of the International PLD Registry was supported by a EASL Registry Research Grants Program and an unrestricted IPSEN grant. EASL and IPSEN had no role in the design or conduct of the study, or in the writing and submission of the manuscript.
The Radboudumc Department of Gastroenterology and Hepatology is part of ERN-rare liver.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
J. P. H. Drenth declares associations with the following organizations/companies: Ipsen, Novartis. All other authors declare no competing interests.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.