
Abstract
Background:
Subcutaneous sacral nerve stimulation is recommended by the United Kingdom (UK) National Institute for Health and Care Excellence (NICE) as a second-line treatment for patients with faecal incontinence who failed conservative therapy. Sacral nerve stimulation is an invasive procedure associated with complications and reoperations. This study aimed to investigate whether delivering less invasive and less costly percutaneous tibial nerve stimulation prior to sacral nerve stimulation is cost-effective.
Methods:
A decision analytic model was developed to estimate the cost-effectiveness of percutaneous tibial nerve stimulation with subsequent subcutaneous sacral nerve stimulation versus subcutaneous sacral nerve stimulation alone. The model was populated with effectiveness data from systematic reviews and cost data from randomized studies comparing both procedures in a UK National Health Service (NHS) setting.
Results:
Offering percutaneous tibial nerve stimulation prior to sacral nerve stimulation (compared with delivering sacral nerve stimulation straight away) was both more effective and less costly in all modeled scenarios. The estimated savings from offering percutaneous tibial nerve stimulation first were £662–£5,697 per patient. The probability of this strategy being cost-effective was around 80% at £20,000–£30,000 per quality-adjusted life-year (QALY).
Conclusion:
Our analyses suggest that offering patients percutaneous tibial nerve stimulation prior to sacral nerve stimulation can be both cost-effective and cost-saving in the treatment of faecal incontinence.
Keywords
Introduction
It is estimated that in the United Kingdom (UK), the prevalence of faecal incontinence in adults living in the community is 1–10%, depending on the definition used.1,2 Faecal incontinence affects the ability to live a normal life, work and socialize, and has huge emotional impact on patients and their carers. Faecal incontinence is associated with high costs to the UK National Health Service (NHS) and society due to heavy use of healthcare services, loss of work productivity, unemployment and disability.
According to the NICE guidelines on managing faecal incontinence, 2 the first-line treatment for faecal incontinence is conservative, such as antidiarrhoeal medication, pelvic floor muscle training, bowel retraining, specialist dietary assessment and management, biofeedback, electrical stimulation and rectal irrigation. For patients with a weak but structurally intact sphincter, in whom sphincter surgery is deemed inappropriate, subcutaneous sacral nerve stimulation (SNS) may be the next treatment option. It involves an implantation of a stimulator which applies an electric current to one of the sacral nerves via an electrode placed through the corresponding sacral foramen. 3 According to a systematic literature review, 4 41–75% of implanted patients achieved complete continence and 75–100% experienced 50% improvement in the number of faecal incontinence episodes. However, the implantation of a stimulator is associated with complications such as pain, lead migration, wound infection and loss of effectiveness. The reported pooled incidence of pain and infection after implantation was 13.0% and 3.9%, respectively. 5 Complications may lead to removal of the stimulator and subsequent re-implantation.
Percutaneous tibial nerve stimulation (PTNS) is a less invasive treatment available for people with faecal incontinence who do not respond adequately to conservative therapy. 6 It involves electrical stimulation of the posterior tibial nerve via a needle percutaneously inserted into the ankle and connected to an external pulse generator. Initial treatment usually consists of 12–15 outpatient sessions lasting 30 min each, typically a week apart. Treatment usually requires two top-up sessions every 6 months. Adverse events are rare and resolve spontaneously. PTNS was shown to be less effective in reducing faecal incontinence compared with SNS.4,7,8 The UK National Institute for Health and Care Excellence (NICE) guidance on PTNS states that there is limited evidence on the benefits of PTNS, particularly in the long term. 6 It recommends that PTNS should only be used ‘with special arrangements for clinical governance, consent and audit or research’. 6 In recent years there has been a growing body of evidence demonstrating the effectiveness of PTNS for faecal incontinence, including the long-term effects of this procedure.4,7–9 In light of these findings, the current NICE recommendations on the management of faecal incontinence2,6 should be reviewed.
Although PTNS appears to be less effective than SNS, it can be delivered prior to SNS due to good acceptance by patients. Patients eligible for SNS could be treated with PTNS before being considered for sacral nerve stimulation. 10 The cost-effectiveness of this strategy is debatable, since patients receiving both treatments incur higher costs than people receiving one of the treatments. Comparing the costs of PTNS and SNS is not straightforward, given that SNS costs are incurred mainly upfront, while PTNS costs incur over time due to maintenance treatments. To enable a comparison between the two treatment strategies, a decision analytic model was developed which compared the cost-effectiveness of PTNS followed by SNS upon PTNS failure, versus SNS alone, over a 5-year time horizon. The model was populated with effectiveness data from published studies4,7–21 and the cost data from the randomized pilot study comparing PTNS with SNS in a UK NHS setting. 22
Materials and methods
SNS and PTNS treatments
SNS is delivered in two stages. At the first stage a temporary peripheral nerve electrode is inserted under local anesthetic and attached to an external stimulator. Temporary SNS is delivered under local anesthetic as an outpatient procedure. The patients will be given questionnaires to record their faecal incontinence symptoms during the test period (2–3 weeks). 3 They may develop complications such as pain, wound infection, electrode dislocation and loss of effectiveness. Treatment of these complications may include: adjusting the stimulator’s settings, electrode re-positioning, wound revision, antibiotic treatment, removal of electrode, and insertion of new electrode. If faecal incontinence symptoms improve during the testing period (2–3 weeks), the permanent lead and the permanent stimulator (implant) will be inserted. This procedure is delivered as a day case under general anesthetic. 3 After the operation patients will be prescribed antibiotics and painkillers. They will be given a handset to control the stimulator and a diary to record symptoms of faecal incontinence. Following implantation patients may develop complications such as pain in the stimulation site, wound infection, lead migration and loss of effectiveness.5,12,15 They may also undergo removal of the device with subsequent re-implantation due to having a magnetic resonance imaging (MRI) scan, or to have the battery changed.13,23 In accordance with NICE guidance 2 all patients with faecal incontinence will attend clinic every 6 months to review the symptoms.
PTNS treatment, delivered by a trained nurse, usually consists of 12 outpatient sessions lasting 30 min each, typically a week apart; treatment may be repeated as required. Adverse events are not included in the model since these are rare and resolve spontaneously. 6
Model description
A decision analytic model was developed in TreeAge Pro Healthcare 2013 (TreeAge Software, Williamstown, MA, USA). The patient population included individuals eligible for SNS based on NICE criteria 1 for symptom severity and failure of prior conservative therapy. 2 The decision trees for SNS and PTNS are shown in Figure 1.

Decision trees for PTNS (a) and SNS (b).
PTNS decision model [Figure 1(a)]. Patients who tolerate PTNS treatment will receive 17 sessions (15 sessions within 3 months plus two top-up sessions at 6 months). Patients who do not tolerate the treatment (e.g. due to vasovagal response) may discontinue after the first session. Those who achieved ⩾50% improvement in faecal incontinence will continue receiving two PTNS sessions every 6 months. Adverse events for PTNS are not included in the model given that these were minor and resolved spontaneously. Patients who did not achieve a 50% reduction of faecal incontinence after 17 PTNS sessions will proceed to SNS [Figure 1(b)].
SNS decision model [Figure 1(b)]. Patients first receive temporary SNS. They can discontinue the treatment due to intolerance or lack of effectiveness. They can also experience adverse events such as infection, electrode dislocation and pain. Patients who improved their continence in response to temporary SNS will receive permanent SNS. Permanent SNS can cause adverse events (e.g. pain, infection, lead dislocation, loss of effectiveness). The SNS stimulator may require its battery to be changed.
The costing perspective was that of the NHS and Personal Social Services in the UK, with a price year of 2012–2013. The list of model inputs and assumptions used in the model and correspondent references are shown in Table 1. The analysis considered a 5-year time horizon. The ‘success’ of treatment was defined as ⩾50% reduction in faecal incontinence episodes per week. 4
List of parameters used in the model.

PTNS, percutaneous tibial nerve stimulation; SNS, sacral nerve stimulation.
Probabilities
The list of probabilities used in the model is shown in Table 1. Probabilities of >50% improvement in faecal incontinence for SNS and PTNS, and a probability of receiving permanent SNS were taken from a systematic review. 4 The overall probabilities of adverse events for temporary and permanent SNS were estimated as a sum of probabilities for pain in the stimulation site, electrode defect/dislocation and wound infection. Probabilities of individual adverse events were taken from Hezler and colleagues. 12 Sensitivity analyses were conducted including overall probabilities of adverse events for temporary and permanent SNS taken from published studies.14,15,17,20,24,25 The probability of discontinuation for PTNS was defined as probability of vasovagal response to needle placement during PTNS. 16 Due to lack of published data on the discontinuation rate for temporary SNS, it was assumed to be the same as for PTNS (conservative assumption). Probabilities of removal of SNS stimulator due to MRI scan or battery change were taken from Tjandra and colleagues 19 and Hollingshead and colleagues 13
Costs
The costs of delivering SNS and PTNS in an NHS setting were estimated using a micro-costing approach. Data on the use of healthcare resources were collected in a randomized pilot study comparing SNS and PTNS, published elsewhere. 22 Costs used in the model were divided into three categories:
(1) Upfront costs including devices, procedures, consultations and investigations;
(2) Maintenance costs including top-up sessions for PTNS, battery replacement for SNS, and removal of SNS device due to MRI scan;
(3) Costs associated with adverse events for temporary and permanent SNS. The major adverse events for both temporary and permanent SNS were: pain in the stimulation site (not related to stimulator settings), electrode or lead defect/dislocation, wound infection and the loss of effectiveness. It was assumed that all adverse events would require electrode removal with or without subsequent electrode replacement. Costs associated with management of wound infection also included antibiotic treatment. Costs associated with electrode defect (defined as excessive impedance) and electrode dislocation included cost of electrode replacement. Loss of effectiveness was assumed to involve electrode removal without subsequent replacement. The costs of adverse events were calculated by multiplying unit costs associated with management of each adverse event by the probability of each adverse event. Costs associated with adverse events for PTNS were not included in the model given that these adverse events resolve spontaneously.
Unit costs of SNS and PTNS devices were based on invoices. Unit costs of the SNS and PTNS procedures, consultations and investigations were taken from the National Schedule of Reference Costs (2011–2012). 30 The model assumes that all patients incur investigation and examination costs. Patients who proceed to SNS upon failing PTNS will receive additional examinations. The model does not include costs associated with 6-monthly review meetings, since these apply to all patients with faecal incontinence. 2 The lists of unit costs used in the model are shown in Tables 2–4.
Unit costs for PTNS.

PTNS, percutaneous tibial nerve stimulation; UPC, Urgent® PC Stimulator.
Unit costs for SNS.

MRI, magnetic resonance imaging; NHS, National Health Service; SNS, sacral nerve stimulation.
Unit costs of adverse events for SNS.
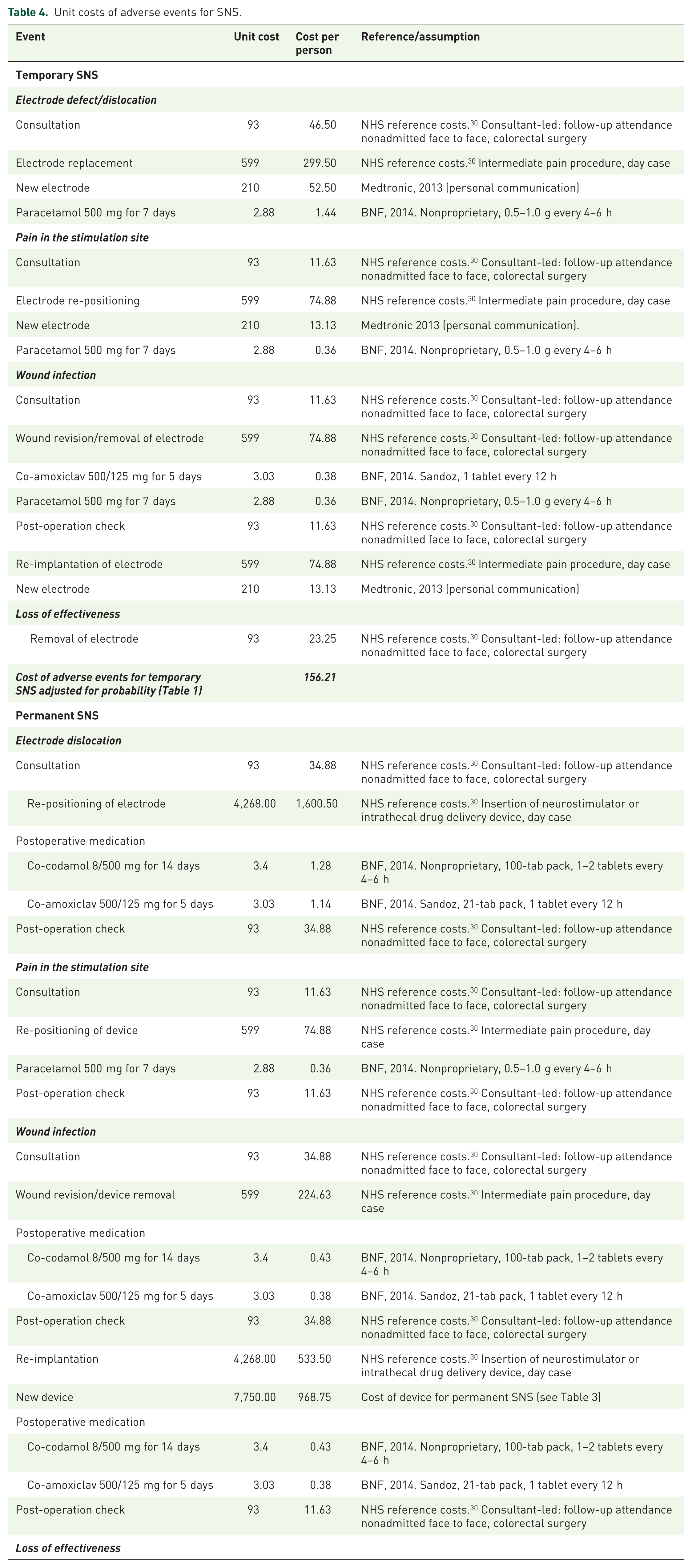
NHS, National Health Service; SNS, sacral nerve stimulation.
Health utilities
Health utilities for patients with faecal incontinence, derived using EQ-5D, were taken from published studies11,18,21 (Table 1). Due to a lack of published data on dis-utilities associated with adverse events for SNS, we used utilities for neuropathic pain derived using EQ-5D. 26 In the base case analysis we used dis-utilities for moderate pain, while in sensitivity analyses we used dis-utilities for mild and severe pain. Dis-utilities associated with adverse events were assumed to be the same for temporary and permanent SNS. In the base case scenario, the duration of adverse events was 7 days (the average UK NHS consultant-led waiting time). 30 In sensitivity analyses the duration of adverse events was 3 and 14 days. The model assumes that patients who discontinued PTNS or SNS with no adverse events have the same utility as those who did not achieve ⩾50% improvement in faecal incontinence.
Discounting
Both costs and quality-adjusted life-years (QALYs) were discounted after year 1 to reflect time preference. In the base case analysis both costs and QALYs were discounted at 3.5%. 28 In sensitivity analyses discount rates were 1.5% and 6%.28,29 Given that the majority of costs (e.g. associated with devices, procedures, and adverse events) were incurred in year 1, the discounting was applied to maintenance costs only.
Cost-effectiveness analysis
The economic analysis complied with the NICE reference case, 28 and is reported according to the Consolidated Health Economic Evaluation Reporting Standards (CHEERS). 31 The primary outcome of the model was the incremental cost-effectiveness ratio (cost per QALY gained). Univariate sensitivity analysis was conducted to assess uncertainty associated with probability of receiving permanent SNS; probabilities of >50% improvement in faecal incontinence for SNS and PTNS; probabilities of adverse events for temporary and permanent SNS; health utility for adverse events; duration of adverse events and costs of SNS and PTNS. A probabilistic sensitivity analysis was undertaken to assess the joint uncertainty in costs and QALYs. 32 Probability distributions were assigned to probabilities, QALYs and costs and 10,000 Monte Carlo simulations were conducted to calculate the probability of cost-effectiveness at the NICE threshold of £30,000 per QALY gained. 28
Results
Costs
The upfront and maintenance costs associated with PTNS are summarized in Table 2. The upfront cost, which included costs of device, consultations, investigations and 15 PTNS procedures, was £2,579 per patient. The cost of two maintenance PTNS procedures was £268 (£535 a year). Analysis assumed one stimulator per 10 patients (15 sessions for each patient) and 15 leads per patient, as per trial. 22 The life-time of a Urgent® PC Stimulator was assumed to be 5 years. The total cost of delivering PTNS in year one was £2,847, and £4,988 over 5 years. Patients who discontinued PTNS due to intolerance incurred cost of £619, which included costs of consultations, investigations and one PTNS procedure. No costs related to adverse events were included, since adverse events for PTNS were minor and transient. The major PTNS costs were associated with clinic attendances to receive PTNS sessions.
Unit costs for SNS are summarized in Table 3. The upfront costs for SNS included costs of consultations, investigations and procedures for temporary and permanent SNS. The total upfront cost of SNS was £13,829 which included the cost of temporary SNS (£1,613) and the cost of permanent SNS (£12,216). All devices were considered to be single use, except for the power source for temporary SNS, which was assumed to be shared by 18 patients, as per trial. 22 Maintenance costs included costs associated with battery change and MRI scan (Table 3), which would require removing the existing device and inserting a new one. Maintenance costs were calculated by multiplying unit costs by the probabilities of needing an MRI scan or battery change. The estimated maintenance cost over a 5-year period was £1,004 per person. The breakdown of costs associated with adverse events for SNS are shown in Table 4. The total cost of adverse events over 5 years multiplied by their probabilities (Table 1) was £156 per patient for temporary SNS, and £880 for permanent SNS. The main SNS costs were associated with the SNS device, followed by operation procedures.
The total PTNS and SNS costs over 5 years (including costs of adverse events and maintenance) are summarized in Appendix 1. These varied in the range £2,847–£4,849 for PTNS, £13,829–£19,153 for SNS, and £16,676–£22,000 for PTNS + SNS (Appendix 1).
QALYs
Total QALYs used in the model are summarized in Table 5. Patients who achieved ⩾50% improvement in faecal incontinence in the absence of adverse events generated 3.454 QALYs over 5 years, while patients who did improve their symptoms had a QALY value of 3.095 (3.5% discounting). This difference equals 131 days with improved continence. Adverse events had a small effect on total QALYs due to their transient character. The total QALYs were sensitive to the discounting rate, while changes in the duration of adverse events had only a very minor effect (Table 5).
QALYs over 5-year period calculated using different discounting rate and different duration of adverse events.

PTNS, percutaneous tibial nerve stimulation; QALY, quality-adjusted life-year; SNS, sacral nerve stimulation.
Cost–utility analysis
In the base case scenario (Table 6) the total cost of the PTNS + SNS treatment strategy was £8,619 over 5 years, and the cost of the SNS strategy was £12,386 (difference in cost −£3767). The total QALYs for patients receiving PTNS + SNS treatment were 3.379, and for SNS 3.310 (difference in QALY 0.070). The PTNS + SNS treatment strategy was less costly and marginally more effective compared with the SNS strategy.
Results of cost–utility analyses.

ICER, incremental cost-effectiveness ratio; PTNS, percutaneous tibial nerve stimulation; QALY, quality-adjusted life-year; SNS, sacral nerve stimulation.
Univariate sensitivity analysis was conducted to address variation in model parameters (Table 6). Results of sensitivity analyses demonstrate that PTNS + SNS remained less costly and more effective in all scenarios. The difference in costs between the two strategies varied from £662 to £5,697 per participant over 5 years. The difference in QALYs varied from 0.029 to 0.135. The model was most sensitive to the probability of receiving permanent SNS following temporary SNS. Nevertheless, PTNS + SNS remained the dominant strategy even when the probability of receiving permanent SNS was set to 1.
Probabilistic sensitivity analysis was conducted to assess joint variation on model parameters using Monte Carlo simulations. Probability distributions assigned to model parameters are summarized in Appendix 2. The cost-effectiveness plane and the cost-effectiveness acceptability curve are shown in Figure 2. Figure 2(a) shows a plot of 1,000 simulations of incremental cost against incremental QALYs. Almost all simulations fell within the south quadrants, indicating that the PTNS + SNS treatment strategy was less costly compared with the SNS only. The ellipse on the graph shows 95% confidence intervals for the incremental cost-effectiveness ratio. The line shows the NICE willingness-to-pay threshold at £30,000 per QALY gained. Figure 2(b) shows the cost-effectiveness acceptability at different willingness-to-pay values. The probability of the PTNS + SNS treatment strategy being cost-effective at £20,000–£30,000 per QALY gained was around 80%.

The cost-effectiveness plane (a) and the cost-effectiveness acceptability curve (b) for the base case scenario.
Discussion
The majority of economic evaluations in healthcare are focused on assessing the cost-effectiveness of alternative treatment options. Cost-effectiveness is the major driver of NICE decisions (82%), although other factors, such as clinical evidence, play an important role. 33 The benefits of PTNS for people with faecal incontinence have been questioned34,35 due to the lack of pronounced clinical effects compared with a sham treatment.36,37 It has been concluded that PTNS is unlikely to be recommended over SNS. 35 However, in real life, patients may prefer treatments which are less effective (although well tolerated) before considering more effective options. 10
In this study we looked at two treatment options, SNS and PTNS, for patients with faecal incontinence who do not respond adequately to conservative therapy. SNS has been previously shown to be more effective and more costly compared with PTNS, at least in the short term. However, comparing two strategies is not straightforward. Firstly, the majority of SNS costs are incurred upfront, while PTNS requires repeated treatments over time. Secondly, SNS is delivered in two stages and proceeding to the second stage depends on the outcome of the first stage. Thirdly, in the long term, SNS may require reoperations due to the loss of effectiveness with time, battery change or the need of MRI scan. Fourthly, patients may first try PTNS before moving to SNS. Although PTNS appears to be less effective compared with SNS, it is less invasive, and therefore more appealing to patients. The long-term effectiveness of PTNS for faecal incontinence is still to be proved, although a sustained therapeutic effect of PTNS was demonstrated for up to 42 months. 9 Due to a lack of long-term data for both SNS and PTNS, we limited our analysis to a 5-year time horizon. Within this time horizon the PTNS + SNS strategy was less costly and more effective compared with SNS alone. The probability of PTNS + SNS being cost-effective was around 80% within the NICE cutoff range of £30,000 per QALY (Figure 2).
Being model-based, this study has a number of limitations. We limited the number of adverse events for SNS to two, and the number of reoperations to one. We also assumed that there will be no hospitalisations associated with adverse events for SNS. As a matter of course, we based our model on conservative assumptions:
(1) In the base case analysis the probability of ⩾50% improvement for PTNS was set to the lowest value;
(2) Initial PTNS treatment included 15 sessions at 30 min each, as per trial, 27 while NICE recommends 12 PTNS sessions at 30 min each. 22
(3) The probability of discontinuation for SNS was assumed to be the same as for PTNS;
(4) It was assumed that the treatment of adverse events associated with SNS will require only one outpatient attendance, which may not be the case in real life.
Our estimations of SNS and PTNS costs are in general agreement with previous studies, except that the latter did not include costs associated with reoperations, adverse events and loss of effectiveness with time. A cost-effectiveness model commissioned by the UK Department of Health 38 showed that total SNS cost over 10 years was £12,847 per person, compared with the cost of conservative management of £3,705 per person. A study by Hotouras and colleagues 39 showed that the one year cost of SNS was £11,374 and for PTNS £1,740. According to our estimations, the cost of SNS ranges from £13,829 to £19,153 and the costs of PTNS from £2,847 to £4,849 per person over 5 years (Appendix 1). The conservative estimate is that 41% of patients will not benefit from PTNS 4 and subsequently receive SNS. For this group of patients, the total cost of PTNS + SNS treatment will be in the range £16,676–£22,000 over 5 years (Appendix 1). A number of sensitivity analyses conducted by varying costs, probabilities and utilities (Table 5) showed that offering PTNS prior to SNS is both less costly and more effective compared with SNS on its own.
The attractiveness of PTNS is that it can be self-administered (by at least a fraction of patients), which could reduce costs associated with maintenance treatments. The home-based PTNS was piloted in nine patients; six of them reported an improvement in faecal incontinence, anxiety and depression. 40
In summary, the results of our study demonstrate that delivering PTNS prior to SNS in the treatment of faecal incontinence can be both cost-effective and cost-saving compared with delivering SNS alone. Offering PTNS would reduce the need for SNS treatments, or at least delay these. It would decrease the costs associated with SNS complications. The savings can be up to £5,697 per patient over 5 years. Our results suggest that the probability of this strategy being cost-effective is around 80%.
Footnotes
Appendix
Model parameters used fin probabilistic analysis.

| Parameters | Mean | SD | distribution | alpha | beta |
|---|---|---|---|---|---|
|
|
|||||
| PTNS ⩾50% improvement | 0.6200 | 0.0300 | beta | 161.6822 | 99.0956 |
| Proceeding to permanent SNS | 0.7350 | 0.1500 | beta | 5.6277 | 2.0290 |
| SNS_⩾50% improvement | 0.7750 | 0.0350 | beta | 109.5439 | 31.8031 |
| Adverse events for temporary SNS | 0.2039 | 0.0828 | beta | 4.6281 | 18.0740 |
| Adverse events for permanent SNS | 0.2487 | 0.0625 | beta | 11.6484 | 35.1864 |
|
|
|||||
| PTNS ⩾50% improvement | 3.3743 | 0.5087 | normal | 44.0037 | 13.0407 |
| PTNS discontinued | 2.8793 | 0.3233 | normal | 79.3048 | 27.5434 |
| Temporary SNS_adverse_no_implant | 2.8710 | 0.3191 | normal | 80.9752 | 28.2043 |
| QALY_TempSNS_no_adverse_no_implant | 2.8793 | 0.3233 | normal | 79.3048 | 27.5434 |
| QALY_PermSNS_adverse2_improved | 3.3579 | 0.4989 | normal | 45.3080 | 13.4931 |
| QALY_PermSNS_adverse2_not_improved | 2.8628 | 0.3148 | normal | 82.6991 | 28.8878 |
| QALY_PermSNS_adverse1_improved | 3.3743 | 0.5087 | normal | 44.0037 | 13.0407 |
| QALY_PermSNS_adverse1_not_improved | 2.8710 | 0.3191 | normal | 80.9752 | 28.2043 |
| QALY_PermSNS_no_adverse_not_improved | 2.8793 | 0.3233 | normal | 79.3048 | 27.5434 |
| QALY_PermSNS_no_adverse_improved | 3.3743 | 0.5087 | normal | 44.0037 | 13.0407 |
|
|
|||||
| ⩾50% improvement | 4,040.61 | 715.54 | gamma | 31.8881 | 0.0079 |
| No improvement | 2,364.21 | 422.01 | gamma | 31.3860 | 0.0133 |
| Discontinued | 607.49 | 30.62 | gamma | 393.7170 | 0.6481 |
|
|
|||||
| Temporary SNS, no adverse events | 1,562.94 | 190.97 | gamma | 66.9787 | 0.0429 |
| Temporary SNS, adverse events | 2,229.23 | 358.08 | gamma | 38.7578 | 0.0174 |
| Permanent SNS, no adverse events, ⩾50% improvement | 14,103.89 | 2,525.38 | gamma | 31.1906 | 0.0022 |
| Permanent SNS, no adverse events, no improvement | 13,267.37 | 2,363.65 | gamma | 31.5067 | 0.0024 |
| Temporary SNS with adverse events + permanent SNS with adverse events, ⩾50% improvement | 18,150.79 | 3,898.14 | gamma | 21.6808 | 0.0012 |
| Temporary SNS with adverse events + permanent SNS with adverse events, no improvement | 17,314.27 | 3,736.41 | gamma | 21.4733 | 0.0012 |
| Temporary SNS with adverse events + permanent SNS no adverse events, ⩾50% improvement | 14,770.18 | 2,692.45 | gamma | 30.0937 | 0.0020 |
| Temporary SNS with adverse events + permanent SNS no adverse events, no improvement | 13,933.66 | 2,530.72 | gamma | 30.3140 | 0.0022 |
| Temporary SNS no adverse events + permanent SNS with adverse events, ⩾50% improvement | 17,484.51 | 3,731.08 | gamma | 21.9603 | 0.0013 |
| Temporary SNS no adverse events + permanent SNS with adverse events, no improvement | 16,647.98 | 3,569.34 | gamma | 21.7544 | 0.0013 |
|
|
|||||
| PTNS + temporary SNS, no adverse events | 3,927.15 | 521.86 | gamma | 56.6305 | 0.0144 |
| PTNS + temporary SNS, adverse events | 4,593.44 | 643.92 | gamma | 50.8871 | 0.0111 |
| PTNS + permanent SNS, no adverse events, ⩾50% improvement | 16,468.11 | 2,697.60 | gamma | 37.2677 | 0.0023 |
| PTNS + permanent SNS, no adverse events, no improvement | 15,631.58 | 2,537.74 | gamma | 37.9412 | 0.0024 |
| PTNS + temporary SNS with adverse events + permanent SNS with adverse events, ⩾50% improvement | 20,515.01 | 4,060.83 | gamma | 25.5219 | 0.0012 |
| PTNS + temporary SNS with adverse events + permanent SNS with adverse events, no improvement | 19,678.49 | 3,899.93 | gamma | 25.4607 | 0.0013 |
| PTNS + temporary SNS with adverse events + permanent SNS no adverse events, ⩾50% improvement | 17,134.39 | 2,863.45 | gamma | 35.8063 | 0.0021 |
| PTNS + temporary SNS with adverse events + permanent SNS no adverse events, no improvement | 16,297.87 | 2,703.40 | gamma | 36.3447 | 0.0022 |
| PTNS + temporary SNS no adverse events + permanent SNS with adverse events, ⩾50% improvement | 19,848.72 | 3,894.26 | gamma | 25.9786 | 0.0013 |
| PTNS + temporary SNS no adverse events + permanent SNS with adverse events, no improvement | 19,012.20 | 3,733.41 | gamma | 25.9331 | 0.0014 |
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The authors declare that there is no conflict of interest.