
Abstract
Background:
Scarce data are available on the epidemiological trend of diverticulitis and its financial burden in Italy. The aim of this work was to explore a potential variation in the rate and costs of hospital admissions for uncomplicated and complicated diverticulitis over the last decade.
Methods:
We selected all hospitalizations for diverticulitis of residents in the Abruzzo Region, Italy between 2005 and 2015. Age-standardized hospitalization rates (HRs) per 100,000 inhabitants for overall, uncomplicated and complicated diverticulitis were calculated. A linear model on the log of the age-standardized rates was used to calculate annual percentage changes (APC). Costs were derived from the official DRG tariff.
Results:
From 2005 to 2015, the HR for acute diverticulitis increased from 38.9 to 45.2 per 100,000 inhabitants (APC + 1.9%). The HR for complicated diverticulitis increased from 5.9 to 13.3 (APC + 7.6%), whereas it remained stable for uncomplicated diverticulitis. The mean hospital cost was 1.8-times higher for complicated diverticulitis compared with that for uncomplicated disease and 3.5-times higher for patients with a surgery stay compared with that for patients with a medical stay.
Conclusion:
During the last decade, in the Abruzzo Region, the HRs for diverticulitis and their costs increased significantly, mainly due to disease complications. Further studies are needed to explore strategies to prevent complications and to realise cost-saving policies.
Keywords
Introduction
Colonic diverticula are a common occurrence in elderly populations in Western industrialized countries. Their prevalence increases with age, reaching 60–80% in patients aged 80 years or older. Most patients remain clinically asymptomatic during their lifetime (diverticulosis), while up to 25% of patients will develop symptoms (diverticular disease; DD) and a variable proportion of them will experience an acute inflammatory process of diverticula (acute diverticulitis; AD). Traditionally, it has been estimated that 4–25% of DD evolves to acute diverticulitis;1,2 however, recent data based on a prospective study indicate lower long-term risk of progression (about 4%). 2
In most cases, AD is uncomplicated and self-limiting, whereas in 15–20% of cases, it is described as a ‘complicated’ presentation with abscess, perforation, fistula, obstruction, peritonitis and sepsis. Moreover, one third of patients with AD will experience a recurrence after the first acute episode, in the following 5 years, and 10% will receive emergency surgery. 3
Keeping in mind the high prevalence and the complexity of this disease, DD represents the fifth most important gastrointestinal disease in terms of healthcare costs in the United States (US) and European countries.4,5 In the US, AD accounts for more than 200,000 hospitalizations a year with costs greater than 2 billion dollars annually. 6 In Italy, a recent paper evaluated the financial impact of the disease in the Marche Region, confirming the progressive increase of management costs. 7 The cost increase is linked to an increase, in recent decades, in the hospitalization rate and incidence of AD, in particular among younger people, as demonstrated by several studies.2,8–10 Data regarding hospitalization rates (HRs) and temporal trends are available mainly in the US, whereas in European countries, few studies have focused on this topic.
The primary aim of our study was to analyse the hospital admission rates of overall, uncomplicated and complicated diverticulitis between 2005 and 2015 in a region of central Italy, by using administrative data. In addition, we also investigated the predictors of surgical intervention and hospital costs for AD. No previous studies have examined these data across these years.
Methods
This cross-sectional study was based on data extracted from the Abruzzo Hospital discharge database between 1 January 2005 and 31 December 2015, provided by the Regional Healthcare Agency of the Abruzzo Region, Italy. Since this automated system is anonymous, according to the Italian Data Protection Authority, neither ethical committee approval nor informed consent were required for this study. 11 The anonymous data file is routinely used by the regional health authorities for epidemiological and administrative purposes. 12
We selected all hospital admissions of residents in the Abruzzo Region who were admitted to any Italian hospital for diverticulitis. Diverticulitis was defined as the presence of ICD9 code (International Classification of Diseases, Ninth Revision, Clinical Modification) 562.11 or 562.13 in the primary diagnosis, or in the secondary diagnosis if a diverticulitis-related complication was recorded as the main diagnosis.
Each hospital admission was attributable to uncomplicated or complicated disease as follows. Complicated diverticulitis was defined as the presence of one of the following conditions in any diagnosis field: intestinal abscess (ICD 9 569.5), fistula (ICD9 569.81, 596.1, 619.1), obstruction (ICD9 560.0, 560.1, 560.2, 560.89, 560.9), peritonitis (ICD9 567.0–567.3, 567.9), sepsis (ICD9 785.52, 995.90–995.92), gastrointestinal haemorrhage (ICD9 578.0–578.9), or perforation (ICD9 569.83). Uncomplicated diverticulitis was defined as the absence of these complications across all diagnostic fields.
Covariates
For each year of the study period, data on patient demographics (sex and age), comorbidities calculated using the Charlson comorbidity index (CCI) score, type of stay and length of stay were reported. 13 Age was categorized into three groups: 20–54, 55–74 and 75+ years old. The type of stay was defined as ‘surgical’ or ‘medical’ if a colectomy code (ICD-9 procedure codes 45.71–45.79, 17.31–17.39, 45.8, 45.81–45.83) or a colostomy code (ICD-9 procedure codes 46.10–46.14, 46.02–46.04) was recorded or not in any procedure field, respectively
Hospitalization rates
From 2005 to 2015, age-standardized HRs for overall, uncomplicated and complicated diverticulitis were calculated and expressed per 100,000 inhabitants. We used the direct standardization method with the 2011 Italian census population as standard. Age-specific HRs were evaluated for each age group using the annual number of hospitalizations for the given age group as the numerator and the annual Abruzzo population for the same age group as the denominator. For each year, the Abruzzo population was derived from the National Institute of Statistics (ISTAT).
Statistical analysis
Chi-square statistics for trend and analysis of variance (ANOVA) were used to compare distributions of categorical variables and continuous variables respectively. Statistical significance was defined as a two-sided p-value <0.05. Annual percent change (APC) was calculated as a measure of trends in HRs for diverticulitis using a linear model on the log of the age-standardized rates. The APC value was considered statistically significant if it differed from zero with a p-value <0.05.
Separate logistic regression models were used to identify significant predictors of surgical stay versus medical stay for overall, uncomplicated and complicated diverticulitis. In these models, only hospital admissions between 2008 and 2015 were analysed in order to investigate the number of hospitalizations for diverticulitis during the previous 3 years as proxy for recurrence of diverticulitis among potential predictors. 6 Calendar year, age group, sex and CCI score were also included in the models as potential predictors. Odds ratios (ORs) and 95% confidence intervals (CIs) are also reported.
From the third-party payer perspective, inpatient hospital costs (for both ordinary and day hospital admissions) were calculated using the regional DRG tariff system. Costs were calculated as the sum for all hospitalizations for diverticulitis recorded in the last year of observation (2015 year). A generalized linear model with gamma distribution and log link was fitted to identify the predictors of hospital costs for diverticulitis. The advantage of this type of model is that it takes into account the skewed nature of cost data and produces β-coefficients that are interpreted as the relative increase in mean cost for each increment in the covariate. Covariates included in the model were sex, age group, CCI score, type of diverticulitis (i.e. complicated or uncomplicated diverticulitis), type of stay (i.e. surgical or medical) and length of stay. Costs were expressed in Euros as mean hospital cost per patient.
Results
From 2005 to 2015, 6073 hospital admissions for diverticulitis were identified. The number of hospitalizations for diverticulitis increased from 495 in 2005 to 638 in 2015 with an increment throughout the period of 28.8% (Table 1 and Figure 1). By comparison, the hospitalizations for all-cause decreased by 46.8% over the same time period (Figure 1).
Hospital admissions for diverticulitis between 2005 and 2015 in the Abruzzo Region.
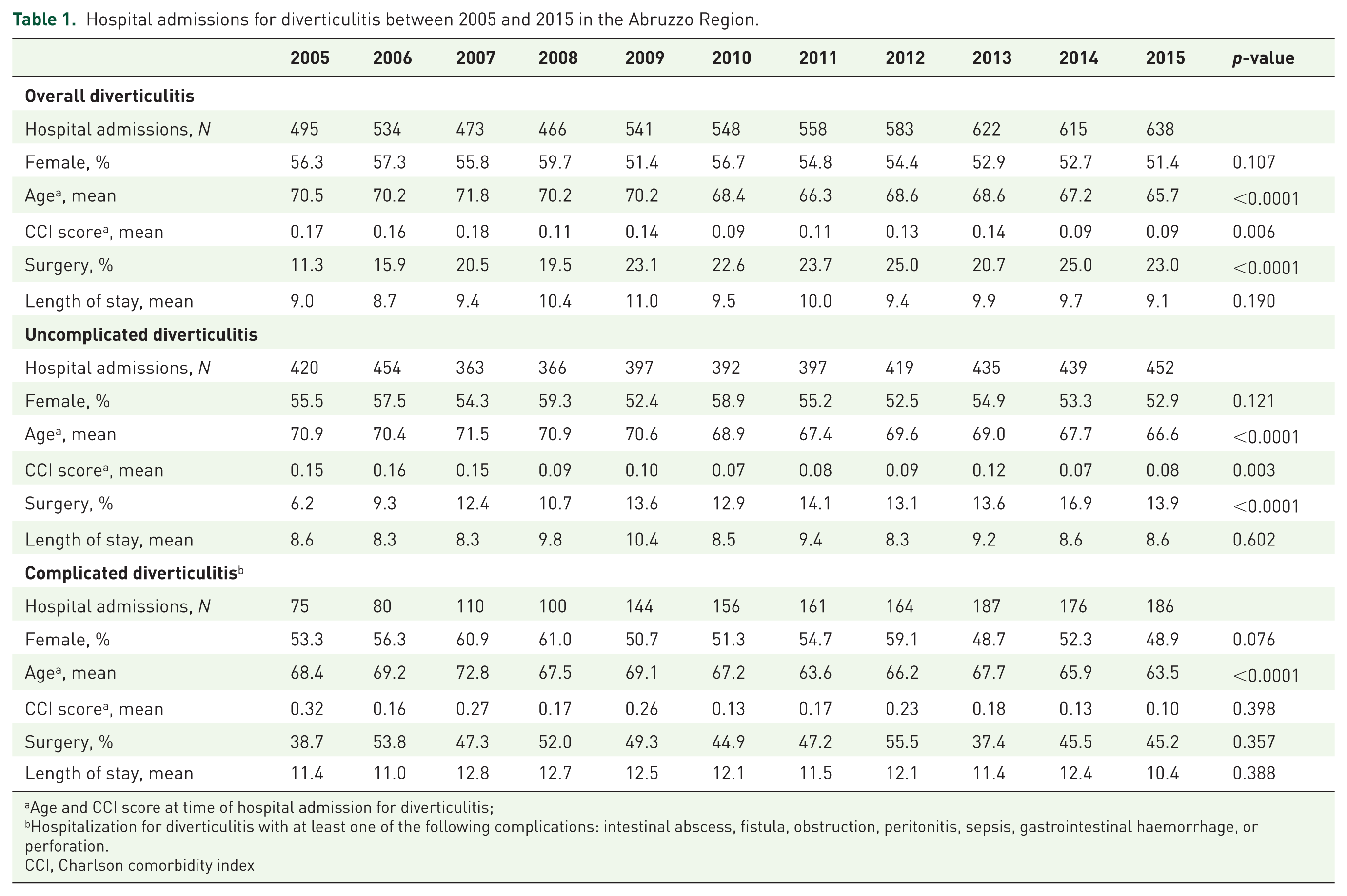
Age and CCI score at time of hospital admission for diverticulitis;
Hospitalization for diverticulitis with at least one of the following complications: intestinal abscess, fistula, obstruction, peritonitis, sepsis, gastrointestinal haemorrhage, or perforation.
CCI, Charlson comorbidity index

Percentage change in all-cause and diverticulitis hospital admissions in the Abruzzo Region, 2005–2015.
The number of admissions for complicated diverticulitis increased almost three-fold from 75 in 2005 to 186 in 2015, whereas it grew only slightly for uncomplicated diverticulitis (+7.6%; Table 1). More than half of all hospitalizations for overall diverticulitis were of women and the mean age decreased significantly over the observation period. Similar results were found for uncomplicated and complicated diverticulitis (Table 1).
The percentage of surgical stays for overall diverticulitis doubled from 11.3% to 23.0% over the period. The principal increase in surgical stays occurred in cases of uncomplicated disease (from 6.2% to 13.9%, p < 0.0001), whereas no comparable difference was detected in cases of complicated disease (from 38.7% to 45.2%, p = 0.357). Finally, the trend analysis of length of hospital stay showed no difference over the observation period for overall, uncomplicated or complicated diverticulitis. During the study period, the mean length of hospital stay was higher in patients admitted for complicated diverticulitis compared with those admitted for uncomplicated disease (p < 0.0001), as expected.
Standardized hospitalization rates
The standardized hospitalization rate for diverticulitis increased from 38.9 per 100,000 inhabitants in 2005 to 45.2 per 100,000 inhabitants in 2015 with an APC of 1.9% (95% CI: 1.0 to 2.9; Figure 2). The HR doubled from 5.9 to 13.3 for complicated diverticulitis with an estimated APC of 7.6% (95% CI: 5.5 to 9.7), whereas it remained stable for uncomplicated diverticulitis (APC = −0.1%; 95% CI: −1.5 to 1.3; Figure 2). The exclusion of recurrence episodes does not modify these results (data not shown)

Standardized hospitalization rate (per 100,000 inhabitants) for overall, uncomplicated and complicated diverticulitis from 2005 to 2015.
HRs for diverticulitis increased progressively with age. In the 2015 year, the rate was more than five times higher in the >75 year age group compared with the <55 year age group. However, the HR in the youngest age group (<55 years of age) showed an upward trend during the study period for overall, uncomplicated and complicated diverticulitis with an APC of 10.7% (95% CI: 7.9–13.6), 8.9% (95% CI: 6.1–11.8) and 14.5% (95% CI: 9.6–19.5), respectively [Figure 3(a)]. In the 55–74 year age group, the HR increased only for complicated disease with an APC of 9.2% (95% CI: 6.6–11.9) whereas it remained fairly stable for overall and uncomplicated diverticulitis [Figure 3(b)]. Finally, the oldest age group showed a statistically significant downward trend only for the uncomplicated diverticulitis with an APC of −2.9% [95% CI: −4.5 to −1.2; Figure 3(c)].

Hospitalization rate per 100,000 persons for overall, uncomplicated and complicated diverticulitis by year and age group (a, b, c).
Predictors of surgical intervention
Table 2 reports the adjusted ORs (overall, uncomplicated and complicated diverticulitis) as potential predictors of a surgical stay compared with a medical stay. For overall diverticulitis, the likelihood of undergoing a surgical intervention was statistically significantly higher in patients who were younger, had diverticulitis-related complications and with an increasing number of previous hospital admissions for diverticulitis.
ORs for predictors of surgical stay (compared with medical stay) for overall, uncomplicated and complicated diverticulitis.

OR was adjusted for all variables listed and for calendar year and sex.
Age and CCI score at the time of hospital admission for diverticulitis.
Hospitalizations for diverticulitis with at least one of the following complications: intestinal abscess, fistula, obstruction, peritonitis, sepsis, gastrointestinal haemorrhage, or perforation.
Hospitalization for diverticulitis during the 3-year period before the date of the admission.
CCI, Charlson comorbidity index; CI, confidence interval; OR, odds ratio
For both uncomplicated and complicated diverticulitis, the increasing number of previous hospitalizations for diverticulitis was a strong predictor of surgery stay with an OR of 3.05 (95% CI: 2.34–3.96) and 2.02 (95% CI: 1.60–2.54), respectively. A younger age was a risk factor for patients admitted for uncomplicated diverticulitis, whereas no significant difference was found for the complicated disease. Conversely, the increase in CCI score was associated with a higher likelihood of surgical stay only in patients admitted for complicated diverticulitis (OR = 1.25; 95% CI: 1.06–1.48).
Hospital costs
In 2015, the mean (± SD) hospital cost per patient admitted for diverticulitis was €3437 ± 3694. Table 3 reports the results from a generalized linear model performed to identify the independent predictors of hospital cost. After adjusting for sex, CCI and length of hospital stay, the estimated mean hospital cost per patient aged >75 years was €4857, that is 1.25-times higher than patients in the youngest age group (p < 0.0001). Moreover, the mean hospital cost was 1.8-times higher in patients admitted for complicated diverticulitis compared with those admitted for uncomplicated diverticulitis (respectively, €5625 versus €3125; p < 0.0001) and 3.5-times higher for patients with a surgery stay compared with those with a medical stay (respectively, €7776 versus €2260; p < 0.0001).
Annual hospital cost per patient admitted for diverticulitis (year 2015).
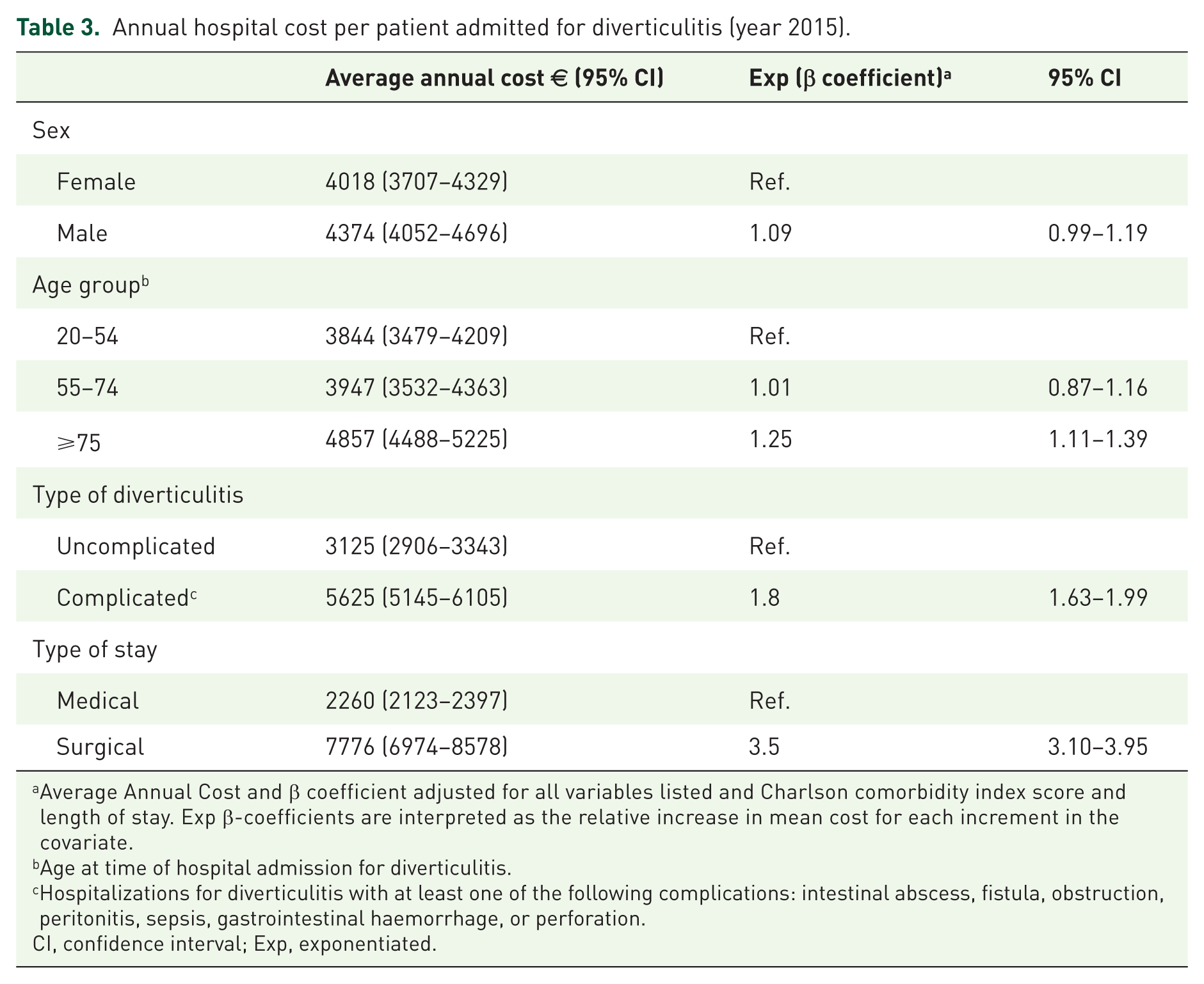
Average Annual Cost and β coefficient adjusted for all variables listed and Charlson comorbidity index score and length of stay. Exp β-coefficients are interpreted as the relative increase in mean cost for each increment in the covariate.
Age at time of hospital admission for diverticulitis.
Hospitalizations for diverticulitis with at least one of the following complications: intestinal abscess, fistula, obstruction, peritonitis, sepsis, gastrointestinal haemorrhage, or perforation.
CI, confidence interval; Exp, exponentiated.
Discussion
This is the first study that has analysed hospital admissions attributed to acute diverticulitis, separating uncomplicated and complicated disease, between 2005 and 2015 in Italy. Overall, we found an increase of 16% in HR for diverticulitis over the study period. The increase was mostly due to complicated diverticulitis (55%) since the uncomplicated form remained essentially unchanged over the study period. An analysis of annual HRs between the different age groups showed that the rate was higher for younger patients compared with older ones.
These data are in line with previous landmark studies that demonstrated remarkable changes in the HR for acute diverticulitis in recent years.9,14–17 Analysing the Nationwide Inpatient Sample (NIS) database, Nguyen and colleagues observed an increase in admissions for AD between 1998 and 2005 (from 61.8/100,000 to 75.5/100,000). 14 A further study from more recent NIS data showed a 9.5% increase in the annual emergency admissions rate for diverticulitis during 2002–2007. 17 A similar trend was also observed in Europe, as demonstrated by Kang and colleagues showing that the hospital admission rate for DD increased in England over the study period (from 1989–1990 to 1999–2000). 16 Similar results have been obtained by Jeyahraia and colleagues, analysing inpatient and day case admissions for DD in the period 1996–2006 in England. A doubling in admission rate was observed during the study period (from 0.56 to 1.20 per 1000/population). 18
Many authors related the increase in HR for AD to a greater and more widespread use of computed tomography (CT) scanning for diagnosis, considering that the higher sensitivity and specificity may allow the identification of the mild form. In our study, the proportion of hospital admissions with a CT scan increased from 11% in 2005 to 35% in 2015 for overall diverticulitis, whereas the range was 10–30% and 19–46% for the uncomplicated and complicated forms, respectively (data not shown). However, this explanation could only in part justify our results, since the rate for the uncomplicated form remained unchanged throughout the study period.
The increase in hospitalizations for AD may reflect a progressive aging of the population. However, our data highlighted a progressive decrease in the mean age of inpatients. In the study period, the mean age of uncomplicated and complicated AD dropped from 71 and 68 years to 67 and 63 years, respectively. In particular, the temporal increase in hospitalizations is more pronounced in younger people, in the group aged 20–54 years. Conversely, we observed a reduction of HR for individuals aged over 75 years.
The increased HR may be due to an increased incidence of AD. Indeed, data from the Rochester Epidemiology Project supports this hypothesis, proving that the incidence of diverticulitis jumped from 115/100,000 person-years in 1980–1989 to 188/100,000 in 2000–2007. 19 A similar trend was also noticed in other studies.20,21
In the present study, we observed a greater temporal trend increase for AD in younger people. This finding has already been observed in a study by Nguyen and colleagues where the age-specific time trends showed an increase in HRs for patients under 45 years of age, whereas the admission rate for patients over 65 years of age was unchanged. 14 Interestingly, we found that the increase in admissions for younger people was mainly associated with complicated disease. This could be the result of a more aggressive course of diverticulitis in this group of patients, as described in previous studies.20–22 Although the reasons underlying these findings are unknown, it is a likely hypothesis that the younger age of patients with AD at admission is due to the effects of lifestyle-related risk factors, including low fibre dietary intake and obesity.23–25 Indeed, a US national survey in the 90s demonstrated both a decline in fibre intake among children and a three-fold rise in childhood obesity in the previous three decades. Probably, the changes of lifestyle in recent generations may have played a critical role in the increased risk of diverticulitis among younger age groups. 23
The increase in hospital admissions for AD appears more interesting if we consider that, in the last decade, a progressive reduction in overall hospital admissions has been observed in Italy and in the Abruzzo Region.26,27
Evidence suggests that comorbidity is a major determinant for severity of AD. The CCI is associated with an increase in AD-related mortality and recurrence rate.28,29 Instead in our study, we found a progressive reduction of CCI score in the observed period, mainly in the uncomplicated form of diverticulitis. This could be explained by the reduction in the mean age of patients at admission.
Our results show a significant trend of an increasing rate of surgical treatment in patients hospitalized for AD, in parallel with the increasing number of admissions, from 10.3% in 2005 to 19.1% in 2015. A recent study 30 compared the emergency operation rates in AD in the US, United Kingdom and Australia during the period 2008–2014: the overall surgical rates were respectively 16%, 13% and 10% with a significant decreasing trend and a significant propensity for the complicated disease. In this study, the increasing trend of surgical treatment was particularly evident in the admissions for uncomplicated diverticulitis, where the rate has more than doubled, with an unmodified surgical rate in patients hospitalized for complicated diverticulitis. This data is possibly in conflict with the current guidelines31–34 that support a conservative treatment of uncomplicated presentations in order to perform elective colectomy after remission of the acute inflammation, since this is associated with a lower complication rate.35,36 One possible explanation could be the increased availability of laparoscopy for elective surgery with a consequent lower surgical threshold.37,38 Also, the younger age and number of previous hospitalizations for AD (mean of three) of patients subjected to surgery has led to surgeons lowering the surgical threshold in uncomplicated diverticulitis. This hypothesis seems to be confirmed by the more homogeneous rate of surgery between age groups and the lower number of previous hospitalizations in patients admitted for complicated diverticulitis.
In several studies it has been highlighted that DD is a source of significant healthcare costs39,40 representing one of the ‘top five’ digestive diseases in terms of direct costs in the US. 41 For the year 2015, in the Abruzzo Region, the average hospital admission costs for diverticulitis proved to be higher for complicated diverticulitis and for older patients (>75 years). Moreover, the form of clinical management also influences admission costs, since we found that patients treated with surgical procedures represent an average cost of €7776 versus medically managed patients who represent an average cost of €2260; this is quite similar to the previous study conducted in the Marche Region. 7 Therefore, considering the progressive increase in hospital admissions for diverticulitis in recent years, especially for complicated presentations, early diagnosis and prevention of AD could be the best strategy for cost saving. 6
This study has limitations, mainly inherent in the use of healthcare administration data. We based our analysis on administrative discharge data that are routinely collected in administrative practice by regional authorities, not specifically focused on the study aims; in addition, our dataset does not include patients who have been attended in emergency rooms for AD and discharged to home without admission. Recent evidences have demonstrated that visits for diverticulitis in the US emergency department have increased by 21% in the period 2006–2011. 42 However, another recent study performed in US emergency rooms has evaluated and compared patients with diverticulitis who were discharged to home versus patients admitted to hospital in the period 2010–2012: 60% of patients were admitted to the hospital while 40% were discharged to home on oral antibiotics. 43 Data relating to the rate of discharge without admission in Italian emergency rooms for diverticulitis are not available and for this reason, the number of uncomplicated diseases could be underestimated. This aspect should be analysed in the future.
In addition, it is possible that ICD9 codes for AD were misreported or not reported (i.e. assignment of codes for abscess or peritonitis, without main diagnosis code for acute diverticulitis) leading to underestimation of the number of admissions for AD. Despite these limitations, the strength of the study lies in the evaluation of the AD burden in a large population using all admissions made inside and outside the Abruzzo Region over an extended period.
In conclusion, we found that hospitalization for AD is growing mainly for complicated presentations among younger people. Complicated diverticulitis is associated with higher hospital costs, resulting in a significant burden for the healthcare system. Considering this evidence, further studies are needed to explore strategies to prevent complications of DD and to realise cost-saving policies.
Footnotes
Acknowledgements
SC was responsible for conception and study design, analysis, interpretation of data, drafting the article; MC was responsible for interpretation of data and drafting the article; AC was responsible for conception and study design, analysis, interpretation of data and reviewed the manuscript critically for important intellectual content; LM was responsible for analysis, interpretation of data and reviewed the manuscript critically for important intellectual content; PA, BT, MEF, GAB and BA reviewed the manuscript critically for important intellectual content; RC was responsible for conception and study design, interpretation of data, drafting the article. All authors approved the final version of the manuscript.
Funding
This study received an unrestricted institutional grant from the pharmaceutical company Alfasigma Italia.
Conflict of interest statement
The authors declare that there is no conflict of interest.