
Abstract
Diverticulosis of the colon is a widespread disease, and its prevalence is increasing especially in the developing world. The underlying pathological mechanisms that cause the formation of colonic diverticula remain unclear but are likely to be the result of complex interactions among age, diet, genetic factors, colonic motility, and changes in colonic structure. The large majority of patients remain asymptomatic throughout their life, one fifth of them become symptomatic (developing the so-called ‘diverticular disease’) while only a minority of these will develop acute diverticulitis. The factors predicting the development of symptoms remain to be identified. Again, it is generally recognized that diverticular disease occurrence is probably related to complex interactions among colonic motility, diet, lifestyle, and genetic features. Changes in intestinal microflora due to low-fiber diet and consequent low-grade inflammation are thought to be one of the mechanisms responsible for symptoms occurrence of both diverticular disease and acute diverticulitis. Current therapeutic approaches with rifaximin and mesalazine to treat the symptoms seem to be promising. Antibiotic treatment is currently advised only in acute complicated diverticulitis, and no treatment has currently proven effective in preventing the recurrence of acute diverticulitis. Further studies are required in order to clarify the reasons why diverticulosis occurs and the factors triggering occurrence of symptoms. Moreover, the reasons why rifaximin and mesalazine work in symptomatic diverticular disease but not in acute diverticulitis are yet to be elucidated.
Keywords
Introduction
Diverticulosis of the colon is the most frequent anatomical colonic alteration, characterized by the presence of pockets called ‘diverticula’. These diverticula are characterized by herniation of the colonic mucosa and submucosa through defects in the muscle layer at the weakest point in the colonic wall: the sites of penetration by blood vessels of the colon wall [Tursi and Papagrigoriadis, 2009]. Diverticula can be detected in both left and right colon. Left-sided diverticula are pseudodiverticula as herniation is not through all colonic layers, while diverticulosis occurring in the right colon is characterized by true diverticula, with herniation of all colonic layers [Tursi and Papagrigoriadis, 2009].
Left-sided diverticulosis is largely age dependent and is uncommon (a prevalence of 5%) in those under the age of 40 years, increasing up to 65% in those aged 65 years or more [Delvaux, 2003]. Right-sided diverticulosis is quite common in Asian people. For example, Yamada and colleagues recently found that right-sided colonic diverticulosis was found in 21.6%, and left-sided or bilateral diverticulosis was found in 18.6% of people undergoing colonoscopy [Yamada et al. 2014].
Although most people with colonic diverticulosis remain asymptomatic, about 20% of patients will develop symptoms, the so-called ‘diverticular disease’ (DD) [Strate et al. 2013] and, of these, 15% will ultimately develop complications [Tursi et al. 2015c]. DD imposes a significant burden on westernized national health systems. In the United States, its prevalence increases with age, with about 70% of people aged at least 80 years showing diverticulosis [Strate et al. 2013]. DD accounts for more than 300,000 hospital admissions, 1.5 million inpatient care days, and $2.4 billion in direct costs each year [Strate et al. 2013]. The incidence of DD and its complications appear to be increasing, and the number of patients with DD can be expected to increase in coming years in accordance with current trends as the population continues to age. In the United States, the overall annual age-adjusted admissions for acute diverticulitis increased from 120,500 in 1998 to 151,900 in 2005 (+26%). Rates of admission increased more rapidly in patients aged 18–44 years (+82%) and 45–74 years (+36%). Elective operations for diverticulitis rose from 16,100 to 22,500 per year during the same time period (+29%), also with a more rapid increase (73%) in rates of surgery for individuals aged 18–44 years [Etzioni et al. 2009]. Finally, in Europe DD accounts for about 13,000 deaths/year [Delvaux, 2003].
Diverticular terminology
The literature is replete with terms of unclear meaning, such as DD, symptomatic diverticulosis, and symptomatic uncomplicated DD (SUDD). Hence, the correct use of these terms is the following:
‘Diverticulosis’ is the mere presence of colonic diverticula; these may, or may not, be symptomatic or complicated.
DD is clinically significant and symptomatic diverticulosis; this may be different from true diverticulitis or from other less well understood manifestations (e.g. visceral hypersensitivity in the absence of verifiable inflammation) [Sheth et al. 2008]. The overarching term DD implies that the pathologic lesion (diverticulosis) rises to the level of an illness. SUDD is a subtype of DD in which there are persistent abdominal symptoms attributed to diverticula in the absence of macroscopically overt colitis or diverticulitis. In contrast, ‘diverticulitis’ is the macroscopic inflammation of diverticula with related acute or chronic complications. Diverticulitis can be uncomplicated or complicated. It is uncomplicated when computerized tomography (CT) shows colonic wall thickening with fat stranding, while it is complicated when CT finds abscess, peritonitis, obstruction, fistulas, and hemorrhage [Sheth et al. 2008].
‘Segmental colitis associated with diverticulosis’ is a unique form of chronic diverticulitis that occurs in areas marked by diverticulosis that may be a variant or forerunner of inflammatory bowel disease (IBD) [Tursi et al. 2012].
Primary focus in this article is on the epidemiology, pathogenesis, and outcome of left-sided diverticulosis.
Epidemiology
For many years it has been thought that this type of diverticulosis exclusively affected the westernized world and was due to a lack of fiber in the diet and increased pressure in the colonic wall [Floch and Bina, 2004; Aldoori et al. 1994]. However, recent data have revealed an increase in the prevalence of colonic diverticulosis throughout the world [Fong et al. 2011; Alatise et al. 2012].
Necroscopic studies from the first part of the twentieth century report a colonic DD incidence between 2–10% and 5–20% in patients who underwent a colonoscopy examination [Painter and Burkitt, 1971], being more often encountered in male patients at that time [Forgey, 1966]. This distribution model is now observed in developing countries. Later studies showed an incidence levelling between sexes [Rodkey and Welch, 2000].
Recent studies found an increased prevalence worldwide. In general, diverticulosis has the highest incidence in the United States and Canada [Warner et al. 2007; Strate et al. 2012], reaching 50% in the population aged 60 and above.
Africa
Nigeria reports a diverticulosis incidence as low as 9.4% among patients who underwent colonoscopy [Alatise et al. 2012], Kenya reports a frequency of DD of 6.6% [Calder, 1979], Egypt reports a frequency of diverticulosis of 2% [Elbatea et al. 2011]. The low incidence of DD in African countries can be due to limited access to healthcare in the general population, and to the low life expectancy in this area [Aboagye et al. 2014].
Asia
In southeast Asia, the diverticulosis prevalence varies between 8% and 25% [Chan et al. 1998; Munakata et al. 1993], reaching a peak in the fifth decade [Fong et al. 2011; Miura et al. 2000], affecting the right colon in 70–98% of cases [Sugihara et al. 1984; Munakata et al. 1993; Miura et al. 2000]. A recent study from Thailand by double contrast enemas found diverticular disease in 28.5% of patients [Lohsiriwat and Suthikeeree, 2013]. Similar results were encountered in the population from Singapore and Hong Kong [Ngoi et al. 1992; Markham and Li, 1992]. However, in China and South Korea, the observed prevalence was 1.7–12.1%, affecting the right colon in 75–84% of cases [Pan et al. 1984; Song et al. 2010]. In Japan, a recent study found diverticulosis in 20.3% of the investigated population (mean age 67.6 years) and it was predominantly right sided (48.0 %). The proportion of colonic diverticulosis increased significantly (p < 0.01 for trend) from 66.0% in 2003 to 70.1% in 2011 and was associated (p < 0.01) with an increased number of patients aged 60 years and over [Nagata et al. 2014]. As the countries shift to a westernized lifestyle, an increase in DD incidence is noticed, affecting mainly the left colon [Sugihara et al. 1984].
Arabic countries offer dispersed studies on small groups of patients. A recent study from Saudi Arabia shows an incidence of DD close to 7.5%, the most exposed age being in the sixth decade [Azzam et al. 2013], the lowest incidence being reported in Iran (2.4% in the population aged 50 and above) [Dabestani et al. 1981], while Jordan encountered a 4% incidence in a study conducted over a 3-year period [Fatayer et al. 1981]. Data from Israel are from older studies: diverticulosis prevalence among the Ashkenazi Jews was 19.7%, among the Sephardi and Oriental Jews 16%, and 9.5% among the Arabic population, with a sevenfold incidence increase compared with previous studies [Levy et al. 1985].
South America data on diverticulosis prevalence are from quite old studies. In Bolivia, no cases of diverticulosis were described in autopsy records in 1975 [Rios-Dalenz et al. 1975]. In Mexico, prevalence of diverticulosis ranged from 4.1% to 9.2% in barium enema studies, while it was 1.9% on necrotic studies [Raña-Garibay et al. 2008]. No data are currently available from other large nations, such as Brazil or Argentina.
Europe
On average, the prevalence of diverticulosis among white western patients who have undergone barium enema is 15–35%, being equally distributed between sexes, but more frequent in older patients, affecting the left colon in the vast majority of cases [Delvaux, 2003].
Even in smaller geographic areas, significant variations in diverticulosis incidence are encountered.
UK prevalence of diverticulosis recently increased up to 47% [Golder et al. 2011]; studies from Germany found diverticulosis in 21–49% of cases [Delvaux, 2003; Weismüller et al. 2013]. Scandinavian countries showed similar diverticulosis prevalence: Norway diverticulosis incidence was 32.1% [Eide and Stalsberg, 1979]; in Finland, the prevalence of diverticulosis increased from 12% to more than 50%, mainly caused by population ageing and by decreased fiber intake in the diet [Mäkelä et al. 2002].
In Italy, two recent studies assessed diverticulosis prevalence. The first found a 19.4% prevalence on colonoscopy [Tursi et al. 2014]; the second found a 51.4% prevalence on CT colonography [De Cecco et al. 2015].
European developing countries show a lower incidence of colonic DD. Greece encountered diverticulosis in 22.9% of patients at the beginning of the twenty-first century [Paspatis et al. 2001]. In Poland, 21.8% of patients aged 30 and above showed the presence of diverticulosis [Blachut et al. 2004]. In Romania, diverticulosis prevalence increased from 1.29% in 2002 to 2.5% in 2005 [Miron et al. 2007].
USA
In the USA, prevalence of diverticulosis varies among different ethnic groups. In older African-American patients, colonoscopy found diverticulosis in 57.7% of patients [Smoot et al. 2009]. In Hispanic patients with incidental colorectal wall thickening on CT, diverticulosis was found in 43% of patients [Padda et al. 2007]. In Vietnamese patients living in Boston, Massachusetts, diverticulosis was left sided in 50.5%, right sided in 31.1%, and both left and right sided in 18.4% of the studied population [Mehrzad et al. 2015]. Diverticulosis prevalence can vary among the same group of patients. For example, in diarrhea-predominant irritable bowel syndrome (IBS), colonic diverticulosis was identified in 44.4% of such patients [Chey et al. 2010].
Current pathophysiology of diverticulosis
The underlying pathological mechanisms that cause the formation of colonic diverticula remain unclear. These are likely to be the result of complex interactions among age, diet, colonic microbiota, genetic factors, colonic motility, and changes in colonic structure (see Figure 1).
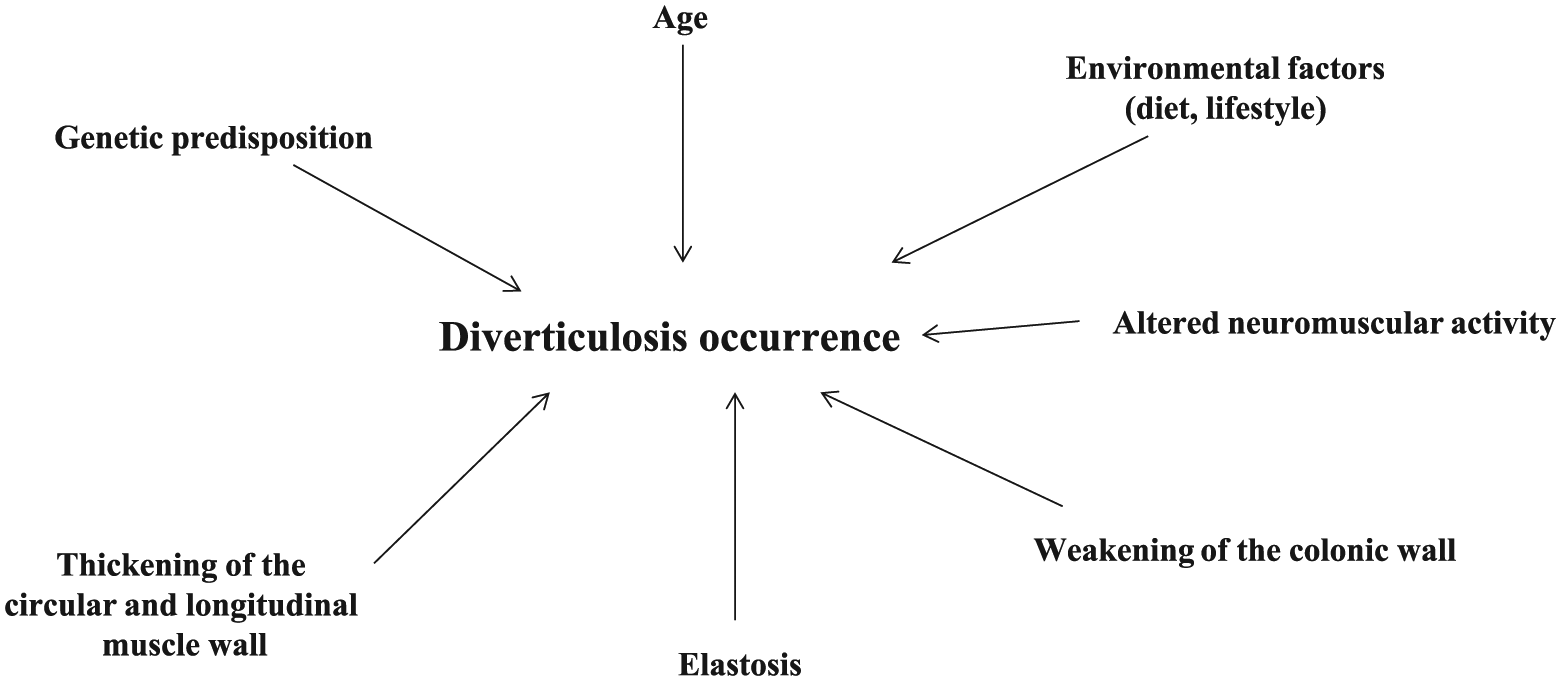
Current knowledge on the possible pathogenesis of colonic diverticulosis.
Age
Diverticulosis was first observed in older patients, with a maximal incidence in patients over 70 years old [Painter and Burkitt, 1971]. However, recent medical literature shows an increase in diverticulosis incidence in young patients. The most important increase was encountered in the group aged 18–44, in which the incidence per 1000 population rose from 0.15 to 0.251 in only 7 years. The incidence in patients aged 45–64 shows a lesser increase (from 0.650 to 0.777 over the same period) [Strate et al. 2012]. Surprisingly, no significant changes in incidence were noticed in the group aged over 65 [Strate et al. 2012].
Some studies suggest that more aggressive forms of the disease are encountered in patients younger than 40, with higher risk of recurrence [Katz et al. 2013].
European countries with a lower socioeconomic status report a 5.3% diverticulosis frequency in patients aged 30–39, 8.7% in those aged 40–49, 19.4% between 50 and 59 and up to 29.6% in subjects over the seventh decade, while maximal incidences were found in patients aged 70–79 and above 80 of 40.2% and 57.9% respectively [Blachut et al. 2004].
Although advancing age is obviously associated with diverticulosis, this association is not strong per se, as it is not age but the prolonged time course during which the colonic wall is exposed and therefore more susceptible to other pathogenetic factors.
Genetic factors
Heritability factors also seem to play a role in the development of DD. Some well defined genetic diseases are associated with a higher incidence of DD.
Patients with Ehlers–Danlos syndrome [Strate et al. 2013], Williams–Beuren [Deshpande et al. 2013], Coffin–Lowry [Machin et al. 1987] and renal polycystic disease [Lederman et al. 2000] are prone to develop diverticula with colonic or other localization.
The association with collagen disease can offer information regarding the mechanisms that lead to diverticula formation. All these syndromes have in common extracellular matrix defects, suggesting that elastin and collagen accumulation in the smooth muscle may be a prerequisite to diverticula formation [Tursi et al. 2015].
Heritability and familial aggregation of diverticulosis and DD have also been investigated. The Swedish Twin Registry was cross linked with the Swedish Inpatient Registry and a diagnosis of DD was found among all twins born between 1886 and 1980 who had not died before 1969. Of a total of 2296 twins having a diagnosis of diverticulosis, the odds ratio (OR) of developing the disease if one twin was affected was 7.15 for monozygotic and 3.20 for dizygotic twins. Similarly, concordance rates and tetrachoric correlations were higher in monozygotic than in dizygotic twins. The heritability was estimated to be 40% and the nonshared environmental effects to be 60% [Granlund et al. 2012]. Similar results were obtained in a similar population-based study conducted in Denmark [Strate et al. 2013].
Specific genes able to predict the occurrence of complications have also recently been investigated. The TNFSF15 gene has been associated with other inflammatory diseases affecting the colon, such as medically refractory ulcerative colitis (UC), aggressive Crohn’s disease (CD), and pouchitis after restorative proctocolectomy [Aiba and Nakamura, 2013]. This gene has recently been investigated in patients undergoing surgical treatment of diverticulitis, and matched with three separate groups: healthy controls, CD control patients and UC control patients. In the discovery phase, the TNFSF15 Single Nuclear Polymorphism (SNP) rs7848647 was significantly associated with diverticulitis compared with all control groups studied (p = 0.0003). The risk allele for this SNP (G substituted for A) was found in all patients with diverticulitis. The homozygous GG allele was found in 62% (13/21) of patients with diverticulitis versus only 5% (1/21) of healthy controls (p = 0.001) and 24% (10/42) of all UC + CD controls (p = 0.002). In the test group, the homozygous GG genotype was found in 56% of patients with diverticulitis compared with 17% of healthy controls (p = 0.006). Risk of diverticulitis seemed to increase with number of the G alleles, with 8% of patients with diverticulitis having AA homozygosity, 35% of patients with diverticulitis having AG heterozygosity, and 56% of patients with diverticulitis having GG homozygosity [Connelly et al. 2014].
Connective tissue
Like many other organs, with advancing age, the intestine is subjected to altered metabolism of extracellular matrix components. Studies have focused on structural alterations of the connective tissue. Two major extracellular matrix components, collagen and elastin, have been found to be altered in diverticulosis: smaller, more densely packed collagen fibrils and an overexpressed cross linking of collagen molecules with increased rigidity and a subsequent loss of tensile strength [Wess et al. 1995; Whiteway and Morson, 1985], and an increase of elastic fibers (elastosis) confined to the longitudinal muscle layer with a subsequent thickening of the colonic wall [Whiteway and Morson, 1985].
The high rigidity of the colon is therefore due to reduced reset force more susceptible to the formation of diverticula. In addition, more recent data found that matrix metalloproteinases are increased and their inhibitors are decreased in patients with diverticulosis, similar to what was observed in Crohn’s disease [Stumpf et al. 2001; Mimura et al. 2004; Meijer et al. 2007].
Colonic motility
Neural degeneration with age may also contribute to diverticulosis occurrence, with several studies suggesting reduction in neurones in the myenteric plexus [Wedel et al. 2013] and decreased myenteric glial cells and interstitial cells of Cajal [Bassotti et al. 2005]. Denervation hypersensitivity has also been reported [Golder et al. 2003], and these abnormalities of enteric nerves might lead to uncoordinated contractions and high pressure, producing diverticulosis. The associated muscular hypertrophy and altered enteric nerves [Simpson et al. 2009] may result from remodeling after acute inflammation, which numerous animal studies have shown to be associated with muscular hypertrophy, abnormal motility [Bercík et al. 2004], visceral hypersensitivity and altered neurochemical coding [Swain et al. 1992; Simpson et al. 2008]. Such changes may account for the common experience of the development of recurrent abdominal pain and disturbed bowel habits following acute diverticulitis [Simpson et al. 2003a], and the finding of visceral hypersensitivity in patients with symptomatic diverticular disease [Clemens et al. 2004; Humes et al. 2012].
Neuromuscular activity
Neurotransmission impairment could be associated with motility changes observed in patients with diverticulosis. A recent in vitro study, performed on circular muscle strips from sigmoid colon of patients with diverticulosis and controls, found that diverticulosis presents decreased spontaneous rhythmic contractions (SRCs) that were significantly enhanced after incubation with Nω-nitro-L-arginine (L-NNA, a nitric oxide inhibitor) and tetrodotoxin. Stimulation of enteric motor neurons caused an increased duration of the latency of off contractions in diverticulosis (p < 0.001), antagonized by L-NNA. No differences in the Inter-contractions50 (IC50) between controls and patients with diverticulosis were observed on inhibition of SRCs for the nitric oxide donor sodium nitroprusside and the preferential P2Y agonist ADPβS. Moreover, neuronal nitric oxide synthase relative expression was also upregulated 2.3 fold in the diverticulosis group (p < 0.05) whereas there was no significant difference in relative expression of inducible nitric oxide synthase, protein-coupled P2Y receptor and the neuronal marker PGP9.5 between groups [Espìn et al. 2014]. These findings suggest that upregulation in the nitrergic pathway in the early stages of the disease might play a role in colonic motor disorders associated with DD [Espìn et al. 2014].
Serotonin is an important neuroendocrine transmitter participating in the control of colonic motor activity through neural and biochemical mechanisms in the enteric nervous system [Simpson et al. 2009]. Thus, a possible pathophysiological factor for diverticulosis occurrence has been hypothesized. However, a significant decrease in signaling including content, release, and 5-Hydroxy-triptamine (5HT) transporter (SERT) transcript levels was present in the mucosa of patients with a history of diverticulitis compared with controls, but not in those with asymptomatic diverticulosis [Costedio et al. 2008]. The same occurs when mucosal 5HT content, enterochromaffin cell numbers, and TpH-1 mRNA levels were assessed [Costedio et al. 2008]. Alterations in serotonin signaling do not appear to be responsible for the development of diverticulosis.
Lifestyle
Fiber intake
It is difficult to study the possible link between dietary fiber intake and diverticulosis because of the time required for the development of diverticulosis and its asymptomatic nature.
The old study from Painter and Burkitt found a significantly different diverticulosis prevalence in a western population than in an African population, in which fiber intake is significantly different [Painter and Burkitt, 1971]. In the late 1970s, Gear and colleagues found diverticulosis to be more frequent in nonvegetarians than in vegetarians (33% versus 12%, p > 0.01). However, nonvegetarians with or without diverticulosis had the same fiber intake (22.8 versus 22.1 g/day), suggesting that other factors may play a role [Gear et al. 1979]. Two recent colonoscopy-based studies raised the question of the role of fiber intake. Song and colleagues did not find differences in dietary fiber scores between patients with and without diverticulosis assessed by the Mini Dietary Assessment index [Song et al. 2010]. Moreover, two recent studies conducted in the USA and Japan surprisingly found that dietary fiber intake was positively associated with the presence of diverticulosis [Peery et al. 2013; Yamada et al. 2014]. Although neither study assessed past diet, these findings raise important questions about the longstanding theory that fiber is the central player in the development of diverticulosis.
Nuts, corn and seeds
Since the late nineteenth century, people with diverticulosis have been advised to avoid nuts, corn and seeds under the assumption that undigested fragments may result in diverticular trauma and complications. In 2008, Strate and colleagues assessed 47,000 men followed for 18 years as part of the Health Professionals Follow-up study. The authors found inverse associations between nut and popcorn consumption and the risk of diverticulitis. The multivariate hazard ratios (HRs) for men with the highest intake of each food (at least twice per week) compared with men with the lowest intake (less than once per month) were 0.80 [95% confidence interval (CI) 0.63–1.01; p = 0.04] for nuts and 0.72 (95% confidence interval 0.56–0.92; p = 0.007) for popcorn. No associations were seen between corn consumption and diverticulitis or between nut, corn, or popcorn consumption and diverticular bleeding or uncomplicated diverticulosis [Strate et al. 2008].
Alcohol and smoking
Two recent case–control studies assessed the role of alcohol and smoking in the pathogenesis of diverticulosis. The first one was conducted in the USA. Aldoori and colleagues assessed these associations in a prospective cohort of 47,678 US men, 40–75 years old. During 4 years of follow up (1988–92), they documented 382 newly diagnosed cases of symptomatic DD. After adjustments for age, physical activity, and energy-adjusted intake of dietary fiber and total fat, alcohol intake (comparing those who drink > 30 g of alcohol/day with nondrinkers) was only weakly and nonsignificantly associated with risk of symptomatic DD [relative risk (RR) = 1.36; 95% CI 0.94–1.97; p for trend = 0.37). They observed no association between caffeine, specific caffeinated beverages, and decaffeinated coffee and the risk of symptomatic DD. Current smoking was not appreciably associated with risk of symptomatic DD compared with nonsmokers (RR = 1.25; 95% CI 0.75–2.09) after adjustment for age, physical activity, and energy-adjusted intake of dietary fiber and total fat. In a subset analysis restricted to men who had undergone sigmoidoscopy or colonoscopy, a modest positive association was seen between smoking and risk of symptomatic DD [Aldoori et al. 1995].
More recently, Nagata and colleagues conducted a prospective cross-sectional study in adult Japanese who underwent colonoscopy. Alcohol, alcohol-related flushing, smoking, medications, and comorbidities were assessed by interviewing the patient on the day of colonoscopy. Alcohol consumption was categorized as nondrinker, light (1–180 g/week), moderate (181–360 g/week), and heavy (⩾361 g/week). Smoking index was defined as the number of cigarettes per day multiplied by the number of smoking years and categorized as nonsmoker, less than 400, 400–799, and at least 800. Univariate analysis revealed age, male sex, smoking index, alcohol consumption, aspirin use, anticoagulant use, corticosteroid use, hypertension, and atherosclerotic disease as factors significantly associated with diverticulosis. Alcohol-related flushing was not associated with the disease. Multivariate analysis showed increasing age (p < 0.01), increasing alcohol consumption (p < 0.01) and smoking (p < 0.01), and atherosclerotic disease (p < 0.01) as significantly associated factors. Alcohol and smoking were associated with right-sided and bilateral diverticula [Nagata et al. 2013].
Red meat
The decrease in fiber intake typically seen with industrialization is paralleled by other dietary changes, including an increase in red meat intake. However, epidemiological studies have provided conflicting results. Manousos and colleagues found red meat positively associated with hospitalization for DD [Manousos et al. 1985]. Aldoori and colleagues found significant association between red meat intake and increased risk of DD, even with no dose–response relationship [Aldoori et al. 1994]. The EPIC-Oxford study found red meat eaters at higher risk of hospitalization for DD than vegetarians but, surprisingly, eaters consuming less than 50 g meat/day had a RR of 0.95 [Crowe et al. 2011]. Peery and colleagues did not find any relationship between red meat intake and diverticulosis found at colonoscopy [Peery et al. 2012].
Physical activity, obesity and serum markers
The increased prevalence of obesity has been associated with increased prevalence of a lot of gastrointestinal diseases, including diverticulosis and DD. Obesity seems to be linked to DD complications but not to diverticulosis occurrence.
Rosemar and colleagues conducted a prospective cohort study of a general population of 7494 men living in Göteborg, Sweden followed for a maximum of 28 years. A relationship between body mass index (BMI) and DD was demonstrated; men with a BMI between 20 and 22.5 kg/m2 had the lowest risk. After adjustment for covariates, the risk increased linearly in men who had a BMI of 22.5–25 (multiple adjusted HR 2.3; 95% CI 0.9–6); 25–27.5 (HR 3; 95% CI 1.2–7.6); 27.5–30 (HR 3.2; 95% CI 1.2–8.6); and 30 or greater (HR 4.4; 95% CI 1.6–12.3) kg/m2 (p for linear trend = 0.004). Men with a BMI of up to 20 kg/m2 had a nonsignificantly elevated risk (HR 3; 95% CI 0.7–12.5). Smoking (HR 1.6; 95% CI 1.1–2.3) and diastolic blood pressure (HR 1.02; 95% CI 1.01–1.04) per mmHg were also independently related to risk of DD [Rosemar et al. 2008]. Strate and colleagues conducted a prospective cohort study of 47,228 male health professionals (40–75 years old) who were free of DD in 1986 (baseline). The authors found that men with a BMI of at least 30 kg/m2 had a RR of 1.78 (95% CI 1.08–2.94) for diverticulitis and 3.19 (95% CI 1.45–7.00) for diverticular bleeding compared with men with a BMI of less than 21 kg/m2. Men in the highest quintile of waist circumference, compared with those in the lowest, had a multivariable RR of 1.56 (95% CI 1.18–2.07) for diverticulitis and 1.96 (95% CI 1.30–2.97) for diverticular bleeding. Waist to hip ratio was also associated with the risk of diverticular complications when the highest and lowest quintiles were compared, with a multivariable RR of 1.62 (95% CI 1.23–2.14) for diverticulitis and 1.91 (95% CI 1.26–2.90) for diverticular bleeding [Strate et al. 2009b]. Significantly, neither Strate [Strate et al. 2009a] nor Song [Song et al. 2010] found a significant relationship between BMI and diverticulosis detected at colonoscopy.
Physical activity also seems to show the same behavior, with a significant relationship with reduction of DD complications but with less evidence of diverticulosis occurrence [Aldoori et al. 1995; Peery et al. 2012, 2013; [Strate et al. 2009a; Williams, 2009; Rosemar et al. 2007].
Why obesity seems to be more linked to DD than diverticulosis is unknown. We know that adipose tissue may release adipocytes and chemokines [Bart and Sigmund, 2012]. Hence, it is hypothesized that the presence of adipose tissue cannot be a risk factor for diverticulosis occurrence, while the proinflammatory effect of these cytokines released by this tissue could explain the higher relationship between obesity and DD occurrence.
The relationship between obesity and some serum markers has recently been investigated as it is thought to influence the risk of diverticulosis occurrence. Comstock and colleagues found that individuals with a waist circumference greater than 45 inches were 8.1 times (95% CI 2.8–23.8) more likely to have diverticulosis than those with a waist circumference less than 38 inches. Leptin was also positively associated with diverticulosis (OR 5.5; 95% CI 2.0–14.7). Both low molecular weight adiponectin (LMW: OR 0.50; 95% CI 0.3–0.8) and the soluble receptor for advanced glycation end products (sRAGE: OR 0.4; 95% CI 0.3–0.7) were inversely related to the presence of diverticulosis. sRAGE levels were not correlated with leptin or C-peptide concentrations. The pattern of high BMI, waist circumference, leptin and C peptide increased the odds of diverticulosis while the pattern of high levels of sRAGE and LMW adiponectin decreased the odds of diverticulosis [Comstock et al. 2014].
From diverticulosis to DD and diverticulitis: what is known, what is still under-researched?
Understanding pathogenesis and establishing adequate medical and surgical management of the disease are the main clinical topics. Some things have been understood, many others still need to be investigated (Figure 2 summarizes possible mechanisms leading to the occurrence of DD).

Current knowledge on the possible pathophysiology of diverticular disease. Further explanation is given in the text.
Why DD and diverticulitis occur: what we know, what is still to be investigated?
When diverticulosis becomes symptomatic, we talk of so-called DD. Thus, it describes the symptoms linked to the anatomical and structural changes in the colon that harbor diverticula.
The clinical classification of DD is still currently based on the 1999 EASGE criteria, which subdivided DD as a symptomatic uncomplicated disease, a recurrent symptomatic disease and a complicated disease [Köhler et al. 1999]. SUDD is characterized by nonspecific attacks of abdominal pain without evidence of an inflammatory process. This pain is typically colicky in nature, but can be constant, and is often relieved by passing flatus or having a bowel movement. Bloating and changes in bowel habits can also occur due to bacterial overgrowth, and constipation is more common than diarrhea. Fullness or tenderness in the left lower quadrant, or occasionally a tender palpable loop of the sigmoid colon, is often discovered on physical examination. Recurrent symptomatic disease is associated with the recurrence of the symptoms described above, and it may occur several times per year. These symptoms may resemble IBS. Some studies recently underlined the overlap between IBS and DD [Jung et al. 2010]. However, abdominal pain (left lower quadrant pain lasting > 24 h) [Cuomo et al. 2013; Tursi et al. 2015], and the detection of increased fecal calprotectin expression are very useful to achieve a correct differential diagnosis [Tursi, 2009]. Complicated disease describes all complications related to DD, ranging from hemorrhage to peritonitis and strictures. Acute diverticulitis (DD with signs and symptoms of diverticular inflammation) is classed as complicated disease, and includes both complicated and uncomplicated disease [Köhler et al. 1999]. But several aspects are not completely understood.
We do not know why symptoms occur, bearing in mind that only one quarter of patients develop symptoms. One hypothesis is that motility alteration may be the cornerstone in symptom occurrence. We know that colonic motility is impaired in those patients, and that it is mainly linked to serotonin imbalance in the muscular layer [Yu et al. 2015]. In fact, we know that gene expression profiles of the serotonergic system and distribution of the serotonin type 4 receptor (5HT 4R) were decreased in the circular muscle layer and myenteric ganglia of patients with SUDD [Better et al. 2013]. In this way, treatment with a 5HT 4R agonist such as prucalopride may have a strong rationale, thanks to its effectiveness in improving colonic motility [Quigley, 2012]. Surprisingly, no studies have been conducted with this drug.
Another point being investigated is why and how diverticulitis occurs. Incidence of diverticulitis among patients with diverticulosis seems to be lower than expected. Over an 11-year follow-up period, only about 4% of patients with diverticulosis developed acute diverticulitis [Shahedi et al. 2013].
It has also been suggested that inspissated fecal matter owing to a low-fiber diet becomes trapped in the diverticula and as a result of colonic bacterial overgrowth, low-grade inflammation develops due to abrasion of the mucosa. This allows access of fecal microbiota into the lamina propria, leading to acute inflammation of the mucosa, which usually begins at the apex of the sac [Simpson et al. 2003; Humes et al. 2007]. This can be associated with acute inflammation of the mesenteric and pericolic fat with the formation of a diverticular abscess. Another postulated mechanism for the development of acute diverticulitis is a microperforation at the fundus of the diverticulum leading to inflammation [Rahden and Germer, 2012]. However, the role of a low-fiber diet and constipation in these patients have not been confirmed [Peery et al. 2013; Yamada et al. 2015].
The detection of small intestinal bacterial overgrowth in patients with diverticulitis supported the hypothesis that bacterial imbalance could play a role in disease occurrence [Tursi et al. 2005]. Unfortunately, more recent studies seem inconclusive. Daniels and colleagues recently compared the fecal microbiota of patients with diverticulitis with control subjects from a general gastroenterological practice using a polymerase chain reaction based profiling technique on DNA isolates from fecal samples. They found that Firmicutes/Bacteroidetes ratios and Proteobacteria load were comparable among patients and controls (p = 0.20), while a higher diversity in diverticulitis for Proteobacteria (p < 0.00002) and all phyla combined (p = 0.002) was found [Daniels et al. 2014]. Surprisingly, results in patients with SUDD seem to be the opposite. We recently found that patients having SUDD do not have bacterial overgrowth compared with healthy controls and patients with diverticulosis alone (p = 0.449). In the same way, no difference was found in the numbers of rRNA gene copies either for total bacteria or in the different types analyzed in the stool samples of the three study groups (Bacteroides, Prevotella: p = 0.354; Bifidobacterium: p = 0.876; Clostridium coccoides: p = 0.463; Escherichia: p = 0.728; Lactobacillus: p = 0.633) [Tursi A et al. 2015]. The difference between patients with SUDD and those with diverticulitis seems therefore clear: significant qualitative but not quantitative differences in bacterial population may be found among patients with diverticulitis and controls, while neither quantitative nor qualitative significant differences in bacterial population may be found among patients with SUDD and controls. Again, why this occurs is unknown.
Why symptoms occur in these patients is therefore unclear and further studies are warranted.
How to treat DD and how to prevent diverticulitis occurrence: what we know, what is still to be studied?
A large number of treatments for SUDD are currently used, ranging from a high-fiber diet to spasmolithics [Tursi et al. 2015]. However, only a few drugs have been investigated in double-blind, randomized, placebo-controlled studies. In particular the nonabsorbable antibiotic rifaximin and the anti-inflammatory drug mesalazine were found to control symptoms and to prevent symptom recurrence in patients with SUDD [Papi et al. 1995; Kruis et al. 2013; Tursi et al. 2013]. Probiotics have also been investigated in this field. However, randomized controlled studies are lacking and definitive conclusions cannot be drawn at present [Tursi et al. 2015].
In the prevention of acute diverticulitis occurrence, open-label trials found both rifaximin and mesalazine with probiotics effective in primary prevention of diverticulitis [Tursi et al. 2015]. However, randomized placebo-controlled studies found rifaximin ineffective in preventing acute diverticulitis occurrence [Papi et al. 1995], while mesalazine was effective [Tursi et al. 2013]. Finally, there are no placebo-controlled trials assessing the role of probiotics [Tursi et al. 2015]. The reasons for these conflicting results remain to be elucidated by further studies.
How to treat acute diverticulitis and how to prevent diverticulitis recurrence: what we know, what is still to be studied?
The treatments of acute diverticulitis are mainly based on support therapy and antibiotics [Tursi et al. 2015]. The use of antibiotics in mild, uncomplicated acute diverticulitis seems to be at least questionable [Chabok et al. 2012], while their use remains mandatory in severe, uncomplicated diverticulitis with comorbidities and in complicated diverticulitis [Tursi et al. 2015].
With regards to the prevention of acute diverticulitis recurrence, open-label trials found rifaximin and mesalazine and probiotics effective in secondary prevention of diverticulitis [Tursi et al. 2015]. However, no randomized placebo-controlled trials assessing the role of rifaximin are currently available. For mesalazine, randomized double-blind placebo-controlled trials failed to find it effective in secondary prevention of diverticulitis, even though there was a significant difference in symptom control among mesalazine formulations Eudragit-L, Eudragit-S, and MMX [Stollman et al. 2013; Parente et al. 2013; Raskin et al. 2014]. The reasons for these conflicting results remain to be elucidated by further studies. Butyrate seems to be a promising tool in this field, thanks to its plurifunctional role in colonic cells [Leonel and Alvarez-Leite, 2012]. A small recent randomized double-blind placebo-controlled trial found microencapsulated sodium butyrate safe and effective in reducing the frequency of acute diverticulitis recurrences, and in improving the quality of life too [Krokowicz et al. 2014]. Further, larger studies have to confirm these promising results.
Finally, there are no placebo-controlled trials assessing the role of probiotics in preventing acute diverticulitis recurrence [Tursi et al. 2015].
Summary and conclusion
Diverticulosis is a common condition that sometimes becomes symptomatic and may lead to severe complications. Its prevalence is higher in the western world, but it is increasing in the developing world as well. Diverticulosis is a multifactorial condition, ranging from structural alteration of the colonic wall, to alteration of colonic motility, but most mechanisms leading to its occurrence remain to be elucidated.
A currently active topic of debate is why symptoms occur. Some hypotheses have been made, ranging from bacterial overgrowth to the presence of low-grade inflammation. However, further studies have to be performed to clarify what is still unknown.
Finally, a great debate is currently ongoing on how to treat symptomatic uncomplicated disease and acute diverticulitis. Current data show that mesalazine and rifaximin are effective in treating SUDD, and that mesalazine is effective in preventing diverticulitis occurrence. Moreover, antibiotic treatment should be reserved for the treatment of complicated disease and for uncomplicated diverticulitis with comorbidities and complicated diverticulitis. Figure 3 summarizes current and potential therapeutic strategies for treating DD. Further, larger studies are required to explain heterogeneity of results to identify a tailored therapeutic strategy.

Current and potential therapeutic approaches in treating diverticular disease. Potential therapeutic approaches are identified with a question mark. Further explanation is given in the text.
Footnotes
Acknowledgements
The author declares that he had no assistance with study design, data collection, data analysis, or manuscript preparation.
Funding
This work received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The author declares that there is no conflict of interest.