
Abstract
Diverticular disease of the colon (DDC) includes a spectrum of conditions from asymptomatic diverticulosis to symptomatic uncomplicated diverticulosis, segmental colitis associated with diverticulosis, and acute diverticulitis without or with complications that may have serious consequences. Clinical and scientific interest in DDC is increasing because of the rising incidence of all conditions within the DDC spectrum, a better, although still limited understanding of the pathogenic mechanisms involved; the increasing socioeconomic burden; and the new therapeutic options being tested. The goals of treatment in DDC are symptom and inflammation relief and preventing disease progression or recurrence. The basis for preventing disease progression remains a high-fiber diet and physical exercise, although evidence is poor. Other current strategies do not meet expectations or lack a solid mechanistic foundation; these strategies include modulation of gut microbiota or dysbiosis with rifaximin or probiotics, or using mesalazine for low-grade inflammation in uncomplicated symptomatic diverticulosis. Most acute diverticulitis is uncomplicated, and the trend is to avoid hospitalization and unnecessary antibiotic therapy, but patients with comorbidities, sepsis, or immunodeficiency should receive broad spectrum and appropriate antibiotics. Complicated acute diverticulitis may require interventional radiology or surgery, although the best surgical approach (open versus laparoscopic) remains a matter of discussion. Prevention of acute diverticulitis recurrence remains undefined, as do therapeutic strategies. Mesalazine with or without probiotics has failed to prevent diverticulitis recurrence, whereas new studies are needed to validate preliminary positive results with rifaximin. Surgery is another option, but the number of acute events cannot guide this indication. We need to identify risk factors and disease progression or recurrence mechanisms to implement appropriate preventive strategies.
The magnitude of the problem
Diverticular disease of the colon (DDC) is one of the most common gastrointestinal disorders, involving a substantial burden on the health system in direct and indirect costs and a marked deterioration in quality of life for patients. DDC includes a number of conditions, ranging from asymptomatic diverticular disease to complicated acute diverticulitis (AD). 1 Because it is often asymptomatic and may never be identified, the true incidence and prevalence of DDC is still not accurately established, although it is now widely accepted that the global incidence of both uncomplicated and complicated DDC is increasing. In recent years, several studies have assessed the economic impact of this disease. In the year 2000, the total (direct and indirect) cost of diverticular disease was estimated to surpass $2.6 billion in the USA. 2 In a follow-up study, the total cost for 2004 had increased to more than $4.0 billion. 3 Moreover, related physician visits in the USA grew from 2.2 million in 1998 to almost 2.7 million in 2009, while hospital stays increased from 230,000 to over 283,000 within the same period.2,4 Data from the UK also show an increase, from 49,000 cases of diverticular disease in 2000 to more than 70,000 in 2006, 5 and cases with complicated disease almost doubled between 1990 and 2005. 6
US data from 2010 showed that diverticular disease was the eighth most frequent outpatient gastrointestinal diagnosis 7 and that there were over 216,000 cases of AD without hemorrhage admissions in 2012, a 21% increase compared with 2003. 7 In the same report, diverticular hemorrhage, included in the gastrointestinal hemorrhage diagnosis, was the most frequent diagnosis of admission, with over 500,000 cases in 2012. Finally, when all causes of death for gastrointestinal, liver, and pancreatic diseases in the USA are considered, diverticular disease ranked 16th in 2012, with a crude rate of 0.9 per 100,000 patients.
Approximately two thirds of adults will develop DDC. 8 From an epidemiological point of view, the two dominant characteristics of this condition when considering both prevalence and incidence are the geographical- and age-dependent differences in the populations studied. In western and industrialized countries, DDC is largely age dependent and uncommon in young people, with a prevalence of 5% in those under age 40 years, increasing up to 65% in those aged 65 years or more. The classic observation holds that the disorder has the highest prevalence rates in these areas but is rare in rural areas of nonindustrialized countries. 9 One widely accepted explanation for this geographic variation is that the fiber-poor diet consumed in western countries plays a decisive etiological role. In fact, a change in immigrant diets to western diets has been proposed to have shifted the prevalence patterns in those populations 10 (Figure 1). Results of several studies support this hypothesis, suggesting an increased number of total diverticulosis cases and increasing rates of diverticular disease–related hospitalizations in these populations compared with rates in their countries of origin.10,11 Recent reports from nonwestern countries also show a greater and growing prevalence of diverticulosis in these areas than previously appreciated.12–16

Graphical expression of relative risks (RRs) and 95% confidence of intervals (CIs) of sociodemographic determinants of hospital admissions for diverticular disease adjusted for the year of birth and sex. Reference for ethnicity was native Swedish people. The figure depicts 10-year risk of hospitalization due to diverticular disease observed in a cohort of 4 million residents in Sweden. It shows lower risk in nonwestern immigrants compared with native Swedish people. Determinants other than ethnicity can be found in the study by Herne and colleagues 10 and include type of work, recipient of social welfare, type of housing and urban residency.
Geography has emerged as an additional determinant of where diverticula arise within the colon. In western countries, a left-sided predominance of DDC has been described, with approximately 90% of patients having diverticulosis in this region. In contrast, individuals from Asian countries tend to have a 75–85% right-sided predominance of diverticulosis. 17 However, emerging data suggest that right-sided diverticulosis in Western countries has been underestimated, with some described rates between 20% and 33% of cases. 18 Beyond geography, ethnicity or race do not seem to be factors. No difference in the prevalence of diverticulosis among black and white populations has been observed, although the distribution of diverticula differs by race, with black people having a greater percentage of diverticula in the proximal colon compared with white people.19,20
At some point in their disease course, an estimated 5–25% of patients with colonic diverticulosis will suffer an episode of AD and up to a third may experience complications. 1 Data from the English Health Care System indicate that 16.3% of inpatient admissions related to diverticular disease eventually involve surgery, of which 58.1% are emergency surgeries and 41.9% elective. The overall surgical admission mortality rates are 10.1% and 15.5% at 30 days and 1 year, respectively (mortality rates, 2.1% and 5.3% at 30 days and 1 year for elective surgery; 15.9% and 22.8% at 30 days and 1 year with emergency surgery), and overall inpatient admissions mortality rates are 5.1% and 14.5% at 30 days and 1 year, respectively. In addition, the overall 28-day readmission rate is 9.6%. 5
Pathogenic mechanisms in DDC that determine current therapeutic approaches
The pathogenic mechanisms involved in DDC are complex and not completely understood. Below, we describe some mechanisms that have been reported and underlie some therapeutic approaches currently used in the management of DDC.
Colonic wall structure
The colonic wall that holds diverticula shows a thickening attributed to elastin deposition within the muscle fibers with a greater than 200% increase in elastin deposition between the muscle cells in the taenia compared with controls.21,22 An increase in type III collagen synthesis in patients with diverticulosis has been described, raising the possibility that age-related changes in collagen composition are also an etiological factor. 21 Moreover, overexpression of a tissue inhibitor of metalloproteinases, which regulate deposition of extracellular matrix proteins, and an increase in levels of this molecule have been described in the colonic tissue of these patients, which might explain the increase in elastin and collagen deposition in the colonic wall with diverticular disease.23,24 These data are consonant with the higher rate of diverticulosis reported in patients with connective tissue disorders. 2
Motility
Early investigations demonstrated higher resting, postprandial, and neostigmine-stimulated luminal pressures in patients with diverticulosis compared with controls.25,26 These findings encouraged a hypothesis based on segmentation of the colon, postulating that contraction of the colon at the haustral folds causes the colon to act not as a continuous tube but as a segmented organ subjected to high pressures.27,28 Classically, it has been suggested that the western diet, with its deficiency in fiber, may facilitate augmented hypersegmentation, increasing the tendency to form diverticula. The abnormal pressures and tonicity may contribute to both formation of diverticula and bowel dysfunction in patients with diverticulosis. In addition, patients with symptomatic diverticular disease have higher motility indices than either asymptomatic patients or controls without colonic diverticuli. 29 Moreover, retropropagation of contractile waves in diverticular segments of colon has been documented, indicating that motility in these patients may be abnormal in both magnitude and direction. 30 Finally, a lower number of interstitial cells of Cajal has been reported in the colonic wall of patients with diverticuli, which may be involved in alterations of the intestinal motility. 31 An increased activity of excitatory cholinergic nerves and decreased activity of nonadrenergic, noncholinergic inhibitory nerves both appear to induce imbalance in the normal excitatory and inhibitory influences, which results in increased tonicity. 32
Environmental factors
Dietary habits involving low fiber content and high red meat intake,33–38 obesity,39,40 smoking,25,26,41 physical inactivity,42–44 alcohol,45,46 and nonsteroidal anti-inflammatory drugs (NSAIDs) 47 have been reported as risk factors for DDC (Figure 2).
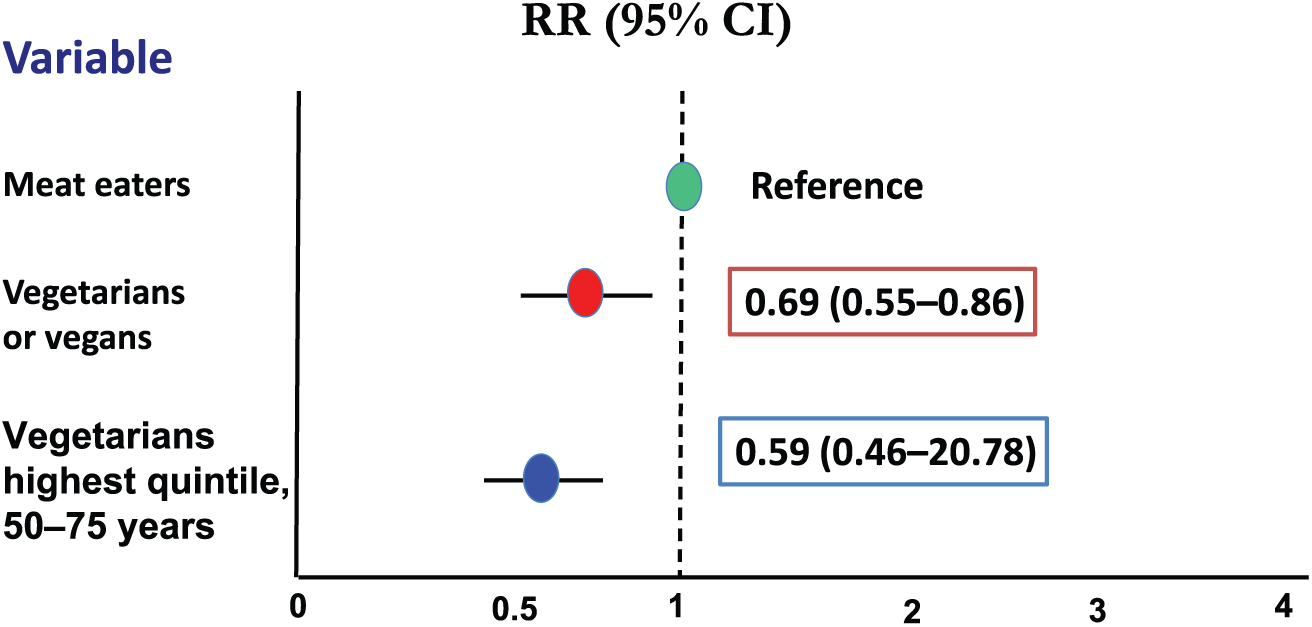
Risk of hospital admission or death due to diverticular disease associated with diet habits in a cohort of 47,033 men and women living in England and Scotland. In relative terms, that risk was 31% lower for vegetarian or vegan patients compared with meat eaters. The risk was 41% lower for those patients taking fiber in the highest fifth quintile. 39 . CI, confidence interval; RR, relative risk.
Heritable factors
A Danish study found that diverticulosis and its complications aggregate strongly in families, with a threefold increased probability of DDC among siblings of index cases than the general population. 48 Another recent investigation reported an odds ratio (OR) of 7.15 [95% confidence interval (CI) 4.82–10.61] for developing diverticular disease if a monozygotic twin is affected, and estimated the hereditable component of diverticular disease at approximately 40%. 49 A single nuclear polymorphism in the TFNSF15 gene has been considered a marker of complicated diverticulitis, suggesting a key role of T-cell receptor gene in T-cell maturation. 50 More recently, a rare single nucleotide variant in the laminin-β 4 gene (LAMB4) has been associated with early onset diverticulitis and unrelated nonfamilial sporadic diverticulitis. 51
Microbiota alterations
The rapid growth of studies focused on the intestinal microbiome has also been a topic of interest in the context of DDC, which may be a clear therapeutic target. Disease-specific variations in intestinal microbiome composition have been found for a number of intestinal disorders. In a recent study, fecal microbiota was compared among diverticulitis patients and control participants, with findings that Firmicutes/Bacteroidetes ratios and Proteobacteria load were comparable among these groups, but that microbiota diversity was higher in diverticulitis for Proteobacteria and all phyla. 52 Another recent cross-sectional study found that patients with diverticula have an increase in colonic macrophages and a depletion of Clostridium cluster IV. 53 Clostridium cluster IX, Fusobacterium, and Lactobacillaceae are reduced in symptomatic diverticular disease compared with people without symptoms and diverticuli confirmed by colonoscopy. Six urinary metabolome molecules allow discrimination of diverticular disease and control groups with over 95% accuracy. 53 Small intestinal bacterial overgrowth, commonly known as SIBO, is a frequent and easily diagnosed form of intestinal dysbiosis. SIBO has been reported to be present in symptomatic uncomplicated diverticular disease (SUDD) 54 and uncomplicated AD, 55 which may contribute to generate and perpetuate the symptoms. Gatta and Scarpignato have shown 56 in a meta-analysis that rifaximin, one of the drugs used in the treatment of DDC, is effective and safe in the treatment of SIBO.
However, although these data are all encouraging and suggest the presence of dysbiosis in patients with diverticular disease, evidence is still insufficient to ensure that microbiota alterations may be behind the development or progression of colonic diverticular disease.
Inflammation
In recent years, several findings have supported a significant role of low-grade inflammation in patients with symptomatic uncomplicated and the development of complicated diverticulosis.57,58 Evidence highlighted as supporting this hypothesis includes enhanced expression of proinflammatory cytokines such as tumor necrosis factor (TNF)-α, which decreases with treatment,59–61 and the fact that obesity is a risk factor for diverticulitis recurrence because of a proinflammatory effect of adipokines and chemokines. 62 Persistent endoscopic and histological inflammation has also been reported and identified as a significant risk factor for diverticulitis recurrence. 63 A recent study found that compared with controls, patients with diverticula, regardless of symptoms, had a greater than 70% increase in colonic macrophages. However, this low-grade inflammation hypothesis has recently been challenged. In a prospective study, Peery and colleagues 64 analyzed 619 patients undergoing a screening colonoscopy, 255 of whom (41%) had colonic diverticula. These authors found no association between diverticulosis and TNF (OR 0.85; 95% CI 0.63–1.16), and no association with CD4+, CD8+, or CD57+ cells. Compared with controls without diverticulosis, biopsy specimens from individuals with diverticulosis were less likely to express the inflammatory cytokine interleukin 6, and no association or evidence for inflammation was found in symptomatic patients when those with versus without diverticulosis were compared. Similar conclusions were reported in another study with a smaller sample size. 65
Clinical presentation of DDC and therapeutic management
Most patients with colonic diverticula have no symptoms; however, it has been estimated that 20% of patients with diverticulosis develop symptoms such as abdominal pain, malaise, swelling, and alteration of bowel habits, which are often difficult to differentiate from functional disorders such as irritable bowel syndrome. 1 A recent report outlines the main features that could help differentiate the conditions (Table 1).
Clinical and biochemical characteristics for the differential diagnosis between SUDD and IBS.

IBS, irritable bowel disease; SUDD, symptomatic uncomplicated diverticular disease.
Symptomatic DDC includes a broad spectrum of clinical manifestations and entities, ranging from symptomatic diverticular disease without complications to patients with diverticula who present with segmental colitis, colonic diverticular hemorrhage, and AD. Very often, symptoms are recurrent (in all their spectrum of clinical conditions) and alternate with periods of apparent clinical silence. Several studies have concluded that even mild symptomatic DDC has a negative impact and affects quality of life compared with control populations.66,67 This impact has recently been validated in a new test (DV-QoL) designed specifically to assess the quality of life in patients with diverticular disease, showing a broad spectrum of negative psychological, social, and physical effects in these patients. 68 In a recent study, Carabotti and colleagues analyzed QoL scores in an Italian cohort of 1217 patients with diverticulosis. They found significantly higher physical and mental component scores in asymptomatic patients with diverticulosis in comparison to patients with SUDD or patients who had a previous episode of diverticulitis. No differences were found between these last two groups, which reinforces the negative impact of this entity on the quality of life of patients. 69
Overall, the goals of treatment of the different forms of diverticular disease are focused on alleviating symptoms and preventing progression, major complications, and recurrence. 70
Asymptomatic DDC
Asymptomatic diverticulosis is usually an incidental finding in patients who undergo colonoscopy or image techniques for other indications. It should be noted that diverticulosis is the most common abnormality on colonoscopy. 3 There is no clear indication for any specific therapy or special follow up in patients with asymptomatic diverticulosis, and no treatment is required. One study found no association between constipation, low-fiber diet, and the presence of colonic diverticulosis. 71 However, prevention of progression of DDC to symptomatic DD is a therapeutic target, and several guidelines include specific recommendations.72–77 Because only a minority of patients with DDC develop symptoms or progress to more severe forms of the disease, it would be of interest to detect the susceptible population. Today, no studies are available that could generate personalized recommendations for people with asymptomatic DDC, but genetic studies or better longitudinal analysis of the microbiome of people who eventually develop symptomatic DDC should be conducted. At present, only a few cross-sectional epidemiological studies have analyzed the microbiome of patients with DDC. As commented above, Barbara and colleagues 53 reported that the fecal microbiota of patients with colonic diverticulosis show differences in symptomatic versus asymptomatic patients. Using mucosal biopsies from the sigmoid colon of 226 patients with and 309 without diverticula during first-time screening colonoscopy, Jones and colleagues 78 found few differences among cases and controls and only very weak associations for comparisons of bacterial abundances in phylum Proteobacteria (p = 0.038) and family Comamonadaceae (p = 0.035). They concluded that the mucosal adherent microbiota community composition was unlikely to play a substantial role in the development of diverticulosis. Tursi and colleagues 79 assessed fecal microbiota from 15 patients with SUDD, 13 with asymptomatic diverticulosis, and 16 healthy controls. Their results also showed that the overall bacterial abundance of dominant species did not differ among the groups, and again only small differences (e.g. higher amount of Akkermansia muciniphila species in patients bearing diverticula compared with controls) of unclear significance were detected. 79
Current recommendations (Table 2) for this stage of the disease are nonspecific and unselected for all people and include dietary recommendations, such as a classically high-fiber diet. However, scientific evidence that supports this recommendation for the sole purpose of preventing symptoms is lacking, although it might be considered part of lifestyle changes that could offer other health benefits, such as smoking cessation, avoiding alcohol consumption, and regularly exercising.72–77 Quality of evidence is rated as low, but a large cohort of 47,033 patients without a history of previous diverticulitis reported a 31% reduction in risk for incident hospitalization for diverticular disease in patients with a high-fiber diet (Figure 1). 38 Evidence is lacking to support claims that a diet rich in nuts, popcorn, or seeds has a beneficial or a harmful effect, so these foods should not be categorically avoided or recommended. 80
Overall treatment recommendations in DDC.

Mesalazine was found to be effective in just one a meta-analysis.
One proof of concept study.
DDC, diverticular disease of the colon; NSAID, nonsteroidal anti-inflammatory drug; SUDD, symptomatic uncomplicated diverticular disease.
Other measures suggested at this stage also encourage primary prevention and treatment of diabetes mellitus, which has been associated with a higher risk for symptomatic and complicated diverticular disease and colonic diverticular hemorrhage. 81 Low levels of vitamin D, obesity and smoking should be avoided to prevent progression to symptomatic DDC and AD.82,83
Symptomatic uncomplicated diverticular disease
SUDD is defined by the presence of nonspecific attacks of abdominal pain of a diverticular source without evidence of an inflammatory process and alteration in bowel habits. Pain is typically colic-like in nature, but can be constant, and is often relieved by passing flatus or with defecation. Other symptoms are diarrhea, constipation, bloating, and tenderness in the left lower quadrant or changes in bowel habits. 1 This entity shares clinical similarities with irritable bowel syndrome, so it is sometimes difficult to distinguish them or attribute the symptoms to the presence of diverticula (see Table 1). Moreover, irritable bowel syndrome is 4.7-fold more likely in patients after an episode of AD than in controls, complicating the diagnosis even more. 84 Laboratory diagnostic evaluation should be normal in patients with SUDD, but some data suggest that fecal calprotectin levels are higher in patients with SUDD compared with normal controls and patients with irritable bowel syndrome. 85 These data need further confirmation because this biomarker might represent a way to differentiate the conditions.
Figure 3 depicts current treatment options for this condition and the pathogenic basis underlying these options. Use of fiber has been a mainstay of SUDD treatment despite a weak evidence base for this practice. In addition, the literature offers no strong guidance regarding type, (e.g. soluble fiber which mainly bulks stool by drawing fluid/water into stool residues, or insoluble fiber which increases bacterial fermentation and accelerates colonic transit time, as well as increasing biomass and inducing changes in colonic pH and intestinal microbiome) 86 and quantity of fiber needed, although in SUDD the insoluble fibers can sometimes worsen symptoms by increasing bloating and flatulence, as happens in irritable bowel syndrome.87,88

Algorithm defining current therapeutic strategies for symptomatic uncomplicated diverticular disease (SUDD). Evidence is very poor, supporting the use of fiber or spasmolitics. Evidence is also limited for the use of other compounds, but rifaximin has been shown to reduce symptoms and reduces the risk of development of acute diverticulitis, whereas mesalazine use is controversial, since it was found not to relive symptoms or prevent acute diverticulitis in some studies, although a recent meta-analysis shows that it can be effective for both outcomes.72–77,89
Data on the use of fiber as a unique treatment for SUDD are ambiguous, but fiber is still recommended,72–77 complemented by other compounds such as cyclic rifaximin (400 mg/12 h for 7 days per month), a combination that is 29% more effective than placebo for symptom relief at 1 year; the number needed to treat for this benefit was 3.72–77 Based on three open and two double-blind randomized clinical trials, one systematic review, and two meta-analyses, the Italian Consensus conference 73 concluded that fiber plus rifaximin leads more patients to be symptom free compared with fiber alone and that rifaximin plus fiber is more effective than fiber alone in preventing AD, with a low therapeutic advantage.
The use of rifaximin is based on the hypothesis that disturbances in the intestinal microbiota might predispose patients to inflammation and excessive production of intestinal gas that eventually induces symptoms.1,90 Rifaximin is a nonabsorbable antibiotic with broad-spectrum activity that decreases the metabolic activity of intestinal flora, increases fecal mass, and reduces bacterial overgrowth. Its safety and tolerability are high because of its very low absorption rates, which implies that nonenteric pathogens are not exposed to selective pressure and the risk of bacterial resistance. 70
Based on the hypothesis that diverticular disease may reflect a dysbiosis (see above), probiotics are also being studied in SUDD, although evidence is lacking to support their use routinely and guidelines do not currently recommend then.72–77 Modification of the microbiome combining rifaximin and probiotics in the long term may be worth exploring as a target.
Additional medical therapies for SUDD, such as mesalazine, are controversial. Mesalazine was suggested as potentially effective in the treatment of SUDD in a way similar to its effects on inflammatory bowel disease, based on the pathogenic hypothesis that a low-grade level of inflammation is present in the colonic mucosa of patients with SUDD. Only the Polish guidelines suggest that mesalazine can be used long term in SUDD. 72 However, available individual studies do not confirm that this approach with mesalazine is effective in the treatment of SUDD or in diverticulitis prevention.73–77 A recent meta-analysis did show that mesalazine administration achieves symptomatic relief and reduces diverticulitis occurrence in a larger proportion of patients with SUDD. However, the absolute risk reduction was statistically significant only when mesalazine was compared with placebo, a high-fiber diet and low-dose rifaximin. 89 Mesalazine seems to be effective in preventing diverticulitis occurrence from SUDD, but not in preventing secondary diverticulitis recurrence. The difference between these entities could be because SUDD can be linked to mucosal inflammation, whereas AD is characterized by transmural inflammation, leading to fibrosis, which may be the key feature explaining mesalazine effectiveness in SUDD but not in diverticulitis. 89
Finally, anticholinergic and antispasmodic agents have been tested concerning the pathogenic presence of hypermotility of the colon in patients with diverticulosis; however, there is no adequate evidence documenting a benefit.72–77
Segmental colitis associated with diverticulosis
Segmental colitis associated with diverticulosis (SCAD) is a recent entity recognized as a distinct and poorly understood manifestation of diverticular disease. It is defined as a segmentary chronic inflammation of the colon in patients with diverticulosis that can mimic the clinical presentation, endoscopic findings, and histologic findings of inflammatory bowel disease, being in some cases indistinguishable from it. 91 The prevalence of SCAD in patients with diverticulosis has been described as 0.3–1.3%. 92 This diagnosis requires the exclusion of inflammation in the rectum and other areas of the colon through biopsies to differentiate it from inflammatory bowel disease. 73 Evidence is insufficient to recommend correct management of this entity, although mesalazine has been suggested, based on its pathophysiology. In any case, the distinction between SCAD and inflammatory bowel disease is important because their natural history and prognosis differ: no long-term medications are required for SCAD.93,94
Acute diverticulitis
Uncomplicated versus complicated diverticulitis
Colonic AD is a worldwide health problem, as one of the most common diagnoses in emergency rooms, and the leading cause for elective colonic resection.8,95–97 Approximately 5–25% of patients with colonic diverticulosis will develop an episode of AD; 85% of those episodes will be uncomplicated, 98 One 11-year follow-up study of incidental diverticulosis during a colonoscopy performed for other reasons found that 4.3% eventually develop an episode of AD at a rate of 6 per 1000 patient years. The incidence rate was only 1.5 per 1000 patients when using a rigorous definition of diverticulitis confirmed by a contrast-enhanced computed tomography (CT) scan or surgery. 99 A recent analysis of the temporal trends of the diagnosis of AD showed a 50% increased incidence of diverticulitis in 2000–2007 (188/1000 person years) compared with 1980–1989 (115/100,000 person years), with an especially relevant increase in women and in younger people. 100 Complicated AD includes the development of intra-abdominal peritoneal infection and perforation. Hinchey’s classification distinguishing five stages of AD is widely used globally (Table 3). 101
Hinchey’s classification.

Classic symptoms of AD involve fever, left lower abdominal pain, tenderness, and leukocytosis, among other signs. 102 These clinical symptoms are suggestive of AD, but a definitive diagnosis is confirmed by ultrasonography or, even better, a contrast-enhanced CT scan. 102 Ultrasounds are often used as a first-line diagnostic tool in patients with suspected AD, and with an expert radiologist, it can be conclusive, leaving CT scans only for doubtful cases. Following this strategy could reduce the number of CT exams by about 50%. 103
The reason some people develop AD and others do not is not well understood. Several studies have identified some risk factors for AD, which include physical inactivity, obesity, constipation, smoking, and use of aspirin or NSAIDs. 98 Statin use was reported to be protective against AD episodes, but this finding was not confirmed in a recent study. 104 A genetic predisposition has been indicated, but the clinical significance of these studies is questionable. 49 Accurate predictors of progression to complicated AD are not available. Leukocytosis with neutrophil count, white cell to lymphocyte ratio, 105 procalcitonin levels 106 or higher levels of calprotectin have been linked to severe AD. 107
Recurrence of AD is common and occurs in 15–30% of cases after a first episode of AD. 98 Treatment goals in AD include reduction or alleviation of symptoms and inflammation, along with prevention of complications and recurrence (Figure 4).
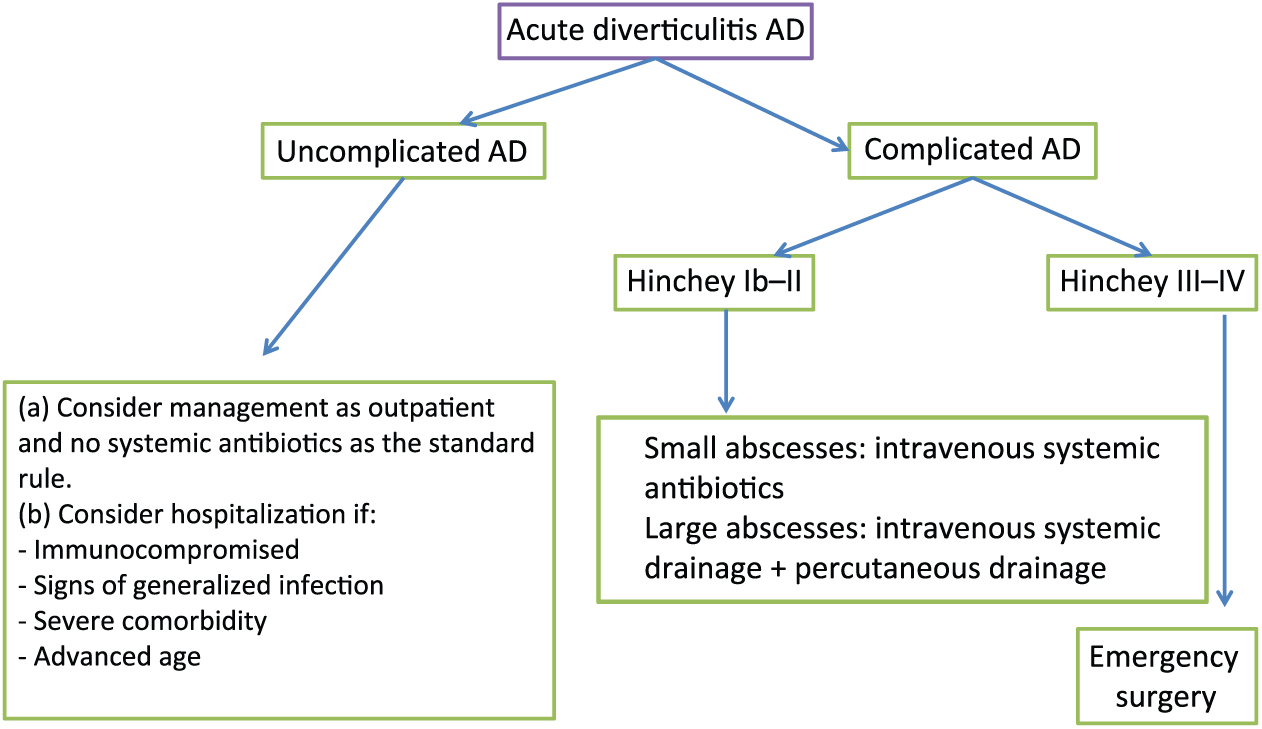
Algorithm defining current therapeutic strategies for acute diverticulitis. See the appropriate section in text.
Treatment of uncomplicated AD (Hinchey stage 0 or Ia)
Inpatient versus outpatient treatment and antibiotics versus no antibiotics for uncomplicated AD A conservative strategy with broad-spectrum antibiotics for at least 7 days in uncomplicated AD can resolve up to 70–100% of events. 108 In recent years, outpatient management in these cases has become more frequent, saving costs to health systems. 109 However, outpatient treatment should not be considered among patients over age 80–85 years or those with severe comorbidities, oral intolerance, or immunosuppression. A short hospital stay can be enough.4,95
Two prospective randomized clinical trials support outpatient management.110,111 In the first trial, almost all patients benefited from outpatient management with only 6% requiring hospital admission. The results showed similar rates of complications and relapse between inpatients and outpatients, with significant cost savings. 110 The second trial included 132 patients randomized to hospitalization versus outpatient treatment after confirmation of left-sided uncomplicated AD by CT scan, and treated with antibiotics. Treatment failure was not different between groups (four versus three patients in each group; p = 0.619). 111 Furthermore, a recent systematic review including 11 articles [one randomized controlled trial (RCT)] concluded that outpatient management for uncomplicated AD had a treatment success rate from 91.5% to 100%, with less than 8% of patients readmitted to the hospital. 112 Although outpatient management for patients with uncomplicated AD and no comorbidities seems feasible, further studies are needed to evaluate short-term and long-term recurrence rates to optimize and stratify the appropriate patients for this type of management.
Another innovative therapeutic approach is being suggested and recommended in several studies worldwide to reduce the use of antibiotics in the clinical management of these uncomplicated cases. Antibiotic treatment should be used in selected cases such as patients with signs of generalized infection, immunosuppressed patients, or conservative nonantibiotic treatment failure. Two systematic reviews have called antibiotic usage into question.113,114 The first systematic review identified three RCTs and reported that antibiotic use did not reduce the duration of symptoms or prevent subsequent complications or recurrence. 113 However, we note that the quality of evidence from the included trials was low because of a high risk of bias, and only patients with modified Hinchey stage Ia and Ib were included, thus excluding immunocompromised patients, those with symptoms of sepsis, or significant comorbidity. Data from a RCT by Chabok and colleagues found that antibiotics may reduce complication risk during treatment [relative risk (RR) 0.49; 95% CI 0.12–1.95], but with no statistical significance. 115 A recent systematic review including eight studies with over 2400 patients found no difference in complication rates between patients taking antibiotics and nonantibiotic usage, with only increasing length of hospital stay without antibiotics. 114 Also, a recent multicenter RCT of systemic antibiotic treatment (1.2 g of amoxicillin clavulanic acid/6 h intravenously for a minimum of 48 h and then switched to oral administration of 625 mg/8 h) versus observation with no antibiotics for a first episode of uncomplicated AD showed that the observational arm was not associated with poorer outcomes. 116
Recommended antibiotic regimens include ciprofloxacin plus metronidazole, penicillin derivatives such as ampicillin or piperacillin/tazobactam, and third-generation cephalosporin to cover gram-positive, gram-negative, and anaerobic bacteria. Data do not support intravenous antibiotic treatment over oral treatment, and duration of treatment from 4 days to over 7 days does not seem to have any advantage related to clinical outcomes.111,117,118 It should be emphasized, however, that the choice of antimicrobials is entirely empiric, since no trial has compared the efficacy of the different regimens mentioned above. 70
Treatment of complicated AD (Hinchey stages Ib to IV)
Hinchey Ib or II includes pericolic or mesocolic (<5 cm) abscess or intra-abdominal, pelvic, or retroperitoneal abscess, or abscess distant from the primary inflammation. Only 15% of patients suffering an episode of AD will develop a complicated episode with pericolic/distant confined abscess or worse. 108 In these cases, inpatient management should be indicated, and treatment varies with the size of the abscess. Conservative treatment with nothing other than a broad-spectrum antibiotic has a success rate up to 70% in abscesses smaller than 4 cm, 119 leaving image-guided percutaneous drainage for previous treatment failures and larger abscesses with a successful treatment rate in up to 80% of cases. 120 Surgery should be planned when conservative treatment fails.
Hinchey III or IV includes generalized purulent peritonitis/fecal peritonitis. Data show a mortality rate of 14% in patients with complicated Hinchey III and IV in AD. In the vast majority of hemodynamically stable cases, early surgery with primary anastomosis with or without fecal diversion is preferable when the patient’s clinical condition can influence different surgery treatments. Hartmann’s surgery procedure is performed in hemodynamically unstable patients.108,121
There is debate concerning the best surgical strategy in complicated AD. Laparoscopic surgery seemed to offer better outcomes than open surgery in AD in a prospective, multicenter, double-blind, parallel-arm RCT of 104 patients with Hinchey I, IIa, or IIb, symptomatic stricture, or severe rectal bleeding. Laparoscopic surgery was associated with a 15.4% reduction in major complication rates, less pain, improved quality of life, and shorter hospitalization. 122 Both the short-term and long-term results of the Sigma trial show a 27% reduction in major morbidity for patients undergoing laparoscopic surgery for diverticular disease. 123 A multicenter, parallel-group, randomized, open-label trial, however, showed no superiority of laparoscopic lavage compared with sigmoidectomy in patients with purulent perforated diverticulitis. 124 In a recent case–control study of 1175 patients undergoing surgery for Hinchey III or IV peritonitis, preoperative assessment based on an Apgar scoring system integrated with peritonitis exposure in complicated diverticulitis offered the best surgical management strategy for reducing local infection, complications, and the need for ostomy. 125
Prevention of recurrence following an episode of AD
After one episode of AD, 15–30% of patients will develop a recurrent episode, although a recent large population-based cohort study reported a lower 11.2% recurrence rate of hospital admission, 126 lower than previously reported, 127 which seems greater in women and younger people. 128 The second episode carries another 30% risk of having a third event, 4 but the first episode seems the most severe. 129 Patients also present often chronic abdominal pain after an AD event that may be difficult to manage. 130 Although quality evidence is still insufficient to identify the best preventive treatment, several secondary prevention strategies have been suggested and include a high-fiber diet, cyclic antibiotic treatment with rifaximin, probiotics, mesalazine treatment, and avoiding NSAIDs. The role of surgery is discussed below (Table 4).
Therapeutic strategies for the prevention of recurrence of acute diverticulitis.

AD, acute diverticulitis.
Dietary and lifestyle recommendations
Classically, physicians implement a high-fiber diet and lifestyle recommendations to reduce the risk of recurrent AD, but whether these measures improve the risk for recurrence remains to be confirmed. No studies are available focusing on the effect of fiber intake on recurrence risk of AD. We identified two systematic reviews including three RCTs regarding the effect of fiber intake on patients with SUDD. The results showed a significant benefit only on pain reduction.143–145 As noted above, the EPIC-Oxford study reported a 31% reduction in risk for incident hospitalization for diverticular disease in patients with high-fiber diet intake (Figure 2). 38 Strate and colleagues, using pooled data from this cohort, estimated that a high-fiber diet would result in a reduction of 59 recurrences of AD at 5 years per 1000 patients treated (95% CI 27–85). 77 Another extended recommendation is to exclude seeds, popcorn, and nuts from the diet in patients with a history of AD because these types of food may accumulate, traumatize, and obstruct the diverticular lumen. Strate and colleagues, in their large, prospective study including 50,000 patients followed for 20 years with medical questionnaires, found no association of this consumption with an increased risk for AD. 77
Weight reduction and smoking cessation may reduce the risk of recurrent AD.39–41 Although no study has evaluated whether physical activity decreases the risk for a second episode of AD, a large cohort of almost 50,000 men aged 40–75 years showed that vigorous physical activity would decrease risk for a first AD episode by up to 34% (RR 0.66; 95% CI 0.51–0.86), whereas no effect was seen with no vigorous physical activity. 43 Obviously, this finding cannot be extrapolated to prevention of AD recurrence, and regardless, many patients having an AD event are older and have different comorbidities that make implementing such a recommendation difficult.
Taking into account several clinical and biochemical parameters one study found that increased risks of recurrent AD included being a younger patient, female, obese, smoker, have dyslipidemia, suffer a first event of complicated AD or have a Charlson comorbidity score greater than 20. 126
Nonabsorbable antibiotics
The only antibiotic proposed for this condition is rifaximin, so far. 73 The suggested dose regimen is 400 mg twice a day over the first week of the month. The role of cyclic rifaximin in preventing AD recurrence has been revisited in three systematic reviews with inconclusive findings of benefit from rifaximin use.145–147 A limited proof-of-concept trial including 165 patients evaluated the effect of 3.5 g fiber supplementation with or without rifaximin 400 mg taken for 1 week per month for 1 year. Recurrences occurred in 10.4% of patients taking rifaximin plus fiber versus 19.3% of patients taking fiber alone. Patients with a prior history of diverticulitis diagnosed at least 1 year from receiving rifaximin also had a lower incidence of recurrence (10% versus 67%). 131 Therefore, although findings are promising, more quality data are needed to strongly recommend the systematic use of cyclic rifaximin for primary and secondary prevention of AD. The multicenter international ROAD trial, which will compare rifaximin versus placebo in the prevention of diverticulitis after a first episode of AD, will be the first to address this question (EudraCT number: 2017-002708).
Probiotics
Bacterial dysbiosis has been proposed as a mechanism involved in the pathogenesis of AD, which suggests that selected probiotics could have a role in recurrence prevention. 70 The first observational study that suggested a possible role of probiotics evaluated the effect of Lactobacillus plus rifaximin in 79 patients with post-diverticulitis colonic stenosis. They found that 88% of patients remained asymptomatic after 12 months of treatment. 141 One small trial of 83 patients evaluated the effect of a high-fiber diet alone versus an Escherichia coli and Proteus vulgaris suspension plus a high-fiber diet for 2 weeks every month, within the first 3 months after an event of AD. Investigators suggested that probiotic use could reduce by 63% the risk for a second AD relapse (RR 0.37; 95% CI 0.08–1.81). 142 One systematic review of 11 studies (four of them on complicated AD) evaluated the efficacy of probiotics in diverticular disease in terms of symptom remission and prevention of AD. A meta-analysis on the efficacy of probiotics in diverticular disease could not be performed because of the poor quality of retrieved studies, and the authors concluded that further investigation is required to assess systematic usage. 132
Mesalazine/mesalamine
Mesalamine [also known as mesalazine or 5-aminosalycylic acid (5-ASA)] is a common therapy among patients with ulcerative colitis. Because AD is an inflammatory process and resolution may still leave a low-grade inflammatory status including cryptitis, crypt abscesses, and other architectural changes, mesalamine has been proposed to reproduce its effects in ulcerative colitis to prevent or reduce recurrence of AD disease. Several double-blind and open RCTs have assessed the role of mesalamine in the prevention of AD recurrence. Most of them showed inconclusive results compared with placebo.133–140 A recent Cochrane review revised the efficacy of mesalamine for the prevention of recurrent AD and included 1805 patients in seven studies judged to have unclear or high risk of bias. The results showed no significant difference for mesalamine compared with placebo (RR 0.98; 95% CI 0.91–1.06; p = 0.63). 140 In addition, an American Gastroenterological Association review on acute diverticular disease analyzed six included clinical trials and found that mesalamine probably does not reduce recurrence risk and could in fact increase the risk of surgery (RR 1.82; 95% CI 0.47–7.03), suggesting that 5-ASA usage should be applied with caution until consistent and quality evidence is available. 77
NSAID and aspirin treatment
No studies have evaluated the effect of NSAIDs or aspirin on patients with prior history of AD, but indirect evidence suggests that these drugs increase the risk of AD. These indirect conclusions can be drawn from data from a long cohort study of 47,000 patients without a history of AD. The results showed that NSAIDs increased the risk of diverticulitis recurrence [adjusted hazard ratio (HR) 1.72; 95% CI 1.40–2.11] and complicated diverticulitis (adjusted HR 2.55; 95% CI 1.32–4.95). 4 Aspirin usage was also studied and increased the risk of AD by up to 20% (adjusted HR 1.2; 95% CI 1.05–1.47). These data, however, must be considered with caution because aspirin use in patients with prior history of cardiovascular events must be maintained, regardless of a history of AD events.
Surgery
Until a few years ago, guidelines recommended elective surgery after two episodes of acute uncomplicated AD or a single episode in young adults, immunosuppressed patients, and complicated AD.148–150 However, based on the increased risk of morbidity and mortality in elective surgery and the fact that recurrent AD is not more serious than a first episode, the clinical trend is to choose surgery on a case-by-case basis. Physicians should individualize treatment, attending to the patient’s medical condition, age, and persistent symptomatology as well as the number of recurrences and their severity.77,108,150 Approximately 10% of patients undergoing elective resection can experience a major surgical complication. 122
Recent data show that the natural history of recurrent AD might be more benign than a first event, with a lower risk of relapse and emergency surgery, and therefore a lower mortality risk. 151 It has been hypothesized that recurrent episodes of AD may protect against perforation because of abdominal adhesion formation. 151 The risk of recurrence in patients after a first episode of AD treated medically is estimated to be less than 20%,151,152 while the risk of recurrence after a successful surgical treatment is 7%, 153 with 10% of patients at risk of experiencing a major surgical complication and increased mortality in patients over 85 years undergoing elective surgery.149,154 Therefore, a systematic elective surgery policy after an episode of AD does not decrease the risk of further surgery or recurrent AD.
The case-by-case recommendation concerning the option of surgery to prevent recurrence of AD must rely on objective findings and not on the number of episodes alone. In clinical practice, CT scans can grade the severity of AD episodes, and left-sided AD, over 5 cm of colon involved, and retroperitoneal abscesses are predictors of recurrence. 155 Also, younger age and persistent postoperative symptoms are strong predictors. 156 Risk of recurrence might be slightly higher in patients younger than 50 years, with a 23% risk at 5 years of follow up versus 16% in patients aged 50 or older. 77 Despite these data, age alone should not be considered exclusively as a determinant for elective surgery, and further data are needed to fill these gaps. Immunosuppressed patients are at higher risk for complicated recurrent AD, with a fivefold increased risk of colonic perforation and thus emergency surgery. 157 However, another study showed that immunosuppressed patients have a higher mortality rate only with the first episode of AD. Therefore, at present, no strong recommendation for elective surgery is possible in this group of patients. 158
The role of colonoscopy
Based on expert opinion, all international guidelines recommend colonoscopy 4–8 weeks following an episode of AD for colorectal cancer exclusion. It is estimated that these recommendations would detect about 15 colorectal cancers per 1000 patients tested and 38 advanced adenomas after an episode of AD, with 0.8 colonic perforations per 1000 patients when the colonoscopy is performed within 7 days after the episode. 157 Some retrospective studies159–165 and a systematic review 166 have called into question this clinical practice. Recent data suggest that the most effective strategy would be to perform a colonoscopy on patients with suspicious malignancy on CT or persistent symptoms after an AD episode. Unfortunately, no quality data regarding this question are available, and more studies are necessary to make a definitive statement. In any case, the need for colonoscopy to rule out the presence of an underlying colorectal cancer raises the question on the potential association between diverticular disease and colorectal cancer based on common risk factors. Available data show no significant increase in colorectal cancer after the first year of follow up, with an increased risk within the first 12 months after diagnosis probably due to surveillance and misclassification in the first place.167,168
Footnotes
Funding
This manuscript and work was possible thanks in part to a grant (FIS PI14/01218) from the Instituto Carlos III and l Fondo Europeo de Desarrollo Regional (FEDER) from de European Union: ‘Una manera de hacer Europa’.
Conflict of interest statement
Angel Lanas has participated in symposiums organized by Alfa Sigma and is chairman of the advisory board for the ROAD trial sponsored by Alfasigma. Aitor Lanas-Gimeno and Daniel Abad-Baroja have no conflict of interest.