
Abstract
Background:
Granulocyte and monocyte apheresis (GMA) has shown therapeutic efficacy in active ulcerative colitis (UC). We thought that in patients with pouchitis after proctocolectomy for UC, GMA might produce immunological effects in the intestinal mucosa, and improve clinical symptoms. This prospective study was to evaluate the efficacy of GMA for antibiotic-refractory pouchitis after proctocolectomy for UC.
Methods:
A total of 13 patients with pouchitis disease activity index (PDAI) > 7 unresponsive to 2 weeks of antibiotic therapy were included. All patients received 10 GMA sessions at 2 sessions/week over 5 consecutive weeks. The primary endpoints were response (a decrease of ⩾3 points in the PDAI) and remission (PDAI < 4). Secondary endpoints included reduction of white blood cells (WBCs), C-reactive protein (CRP), faecal markers (calprotectin and lactoferrin), reduction of the PDAI endoscopic subscore, and GMA safety.
Results:
The median PDAI score was significantly decreased from 11 (range, 9–15) at entry to 9 (range, 6–13) after the GMA therapy (p = 0.02). A total of six patients (46%) responded to the treatment, but none achieved remission. The median endoscopic subscore (maximum: 6) was 5 (range, 4–6) at entry and 5 (range, 1–6) after the treatment (p = 0.10). None of the laboratory markers (WBCs, CRP, faecal calprotectin and lactoferrin) significantly changed during the treatment. Transient adverse events (AEs) were observed in two patients (15%), dyspnoea in one and headache in one. The AEs were not serious, and all patients completed the 10 GMA sessions.
Conclusions:
GMA has a good safety profile, but its efficacy appears to be limited in the management of chronic refractory pouchitis. However, a large controlled study should be conducted to evaluate the efficacy of GMA therapy in patients with pouchitis at an earlier clinical stage, before the disease has become refractory to conventional medical therapy.
Introduction
Pouchitis is a nonspecific inflammatory condition in the ileal pouch reservoir [Shen et al. 2005]. It is the most common long-term complication after ileal pouch surgery, and has a significant adverse impact on patient’s quality of life. The precise pathologic mechanism for the development of pouchitis remains to be described. Nevertheless, some evidence suggests that an abnormal mucosal immune response to altered microflora in the ileal pouch leads to inflammation. However, the immune mechanisms of pouchitis have been extensively studied, and it is understood that inflammatory cytokines including interleukin-6 and tumour necrosis factor (TNF)-α are released in the inflamed mucosa of the ileal pouch of patients with pouchitis [Gionchetti et al. 1994; Patel et al. 1995; Yamamoto et al. 2005]. Such inflammatory activities are thought to be secondary the development of pouchitis.
In Japan since April 2000, the Adacolumn (JIMRO, Takasaki, Japan) has been introduced for selectively depleting elevated granulocytes and monocytes in patients with ulcerative colitis (UC) [Shimoyama et al. 2001; Hanai et al. 2003]. The Adacolumn is filled with cellulose acetate beads of 2 mm in diameter as adsorptive leukocytapheresis carriers. The carriers adsorb approximately 65% of neutrophils and 55% of monocytes, together with a significant fraction of platelets from the blood in the column [Saniabadi et al. 2003, 2005]. Lymphocytes are spared and show a sustained increase in the post Adacolumn leukocytapheresis period [Saniabadi et al. 2003]. Granulocyte and monocyte apheresis (GMA) with the Adacolumn has shown therapeutic efficacy in patients with active UC by modulating systemic and local inflammatory activities [Yamamoto et al. 2010; Passalacqua et al. 2011; Sacco et al. 2013; Yokoyama et al. 2015; Dignass et al. 2016]. Further, several studies have reported that depleting granulocytes and monocytes by GMA leads to a diminished inflammatory profile in the intestinal mucosa, and remission of clinical symptoms in patients with active UC [Muratov et al. 2006; Yamamoto et al. 2006; Matsuda et al. 2009].
With the above background in mind [Gionchetti et al. 1994; Patel et al. 1995; Yamamoto et al. 2005; Muratov et al. 2006; Yamamoto et al. 2006; Matsuda et al. 2009], we thought that in patients with pouchitis after proctocolectomy for UC, GMA might produce immunological effects in the intestinal mucosa, and improve clinical symptoms. In the past, the therapeutic efficacy of GMA in patients with pouchitis has not been evaluated, except in a few case reports [Yanaru-Fujisawa et al. 2005]. This study was designed to evaluate the efficacy of GMA with Adacolumn in patients with antibiotic-refractory pouchitis after total proctocolectomy with ileal pouch-anal anastomosis (IPAA) for UC.
Patients and methods
Study design
This was an open-label, prospective, single arm, multicentre study conducted at four independent institutes in Japan, which regularly receive patients with inflammatory bowel disease (IBD). The study was registered at University Hospital Medical Information Network (UMIN) Clinical Trials Registry (registration identification: UMIN000010207).
In this prospective, noncomparative, pilot trial, the sample size was determined to be 20 during 1 year of the scheduled study period (from February 2013 to January 2014) based on our past experience (total number of IPAAs, incidence of antibiotic-refractory pouchitis and GMA efficacy for active UC).
Patients
The inclusion criteria were: (1) patients who had ileostomy closed after total proctocolectomy with IPAA for histologically diagnosed UC; (2) patients with a current episode of pouchitis defined as a pouchitis disease activity index (PDAI) [Sandborn et al. 1994] of >7; (3) patients with endoscopically detectable lesions in the pouch; and (4) patients with pouchitis unresponsive to 2 weeks of antibiotic therapy. Likewise, exclusion criteria were: (1) patients with a leukocyte count of <2000/µl; (2) patients with serious infection; and (3) those with serious concomitant cerebral, pulmonary, cardiac, hepatic or renal disorders, bleeding complication, or a history of hypersensitivity reaction to an anticoagulant used during extracorporeal circulation, which includes apheresis. During June 2013 and November 2015, 13 patients met the inclusion criteria and were included in this study. Table 1 shows baseline demographic variables of the included patients.
Baseline demographic variables of the study patients (n = 13).

GMA therapy
Each patient received 10 GMA sessions at 2 sessions/week over 5 consecutive weeks. One GMA session was set to be 60 min at 30 ml/min as previously described [Saniabadi et al. 2003]. Patients who were receiving antibiotics, (oral or topical) 5-aminosalicyic acids (5-ASAs), (oral or topical) corticosteroids, immunosuppressants or biologics at entry for an appropriate length of time could continue at the same dosage. However, patients were not allowed to receive new therapeutic drugs for pouchitis during the course of the GMA therapy.
Efficacy assessment
Clinical efficacy and safety assessments were made at entry and at set time points during the treatment. Adverse reactions, stool frequency, rectal bleeding, faecal urgency, abdominal cramps, and fever were recorded. PDAI score (maximum: 18) was compared at entry and after the GMA therapy (within 4 weeks after the last GMA session). The clinical response and remission were defined as a decrease of ⩾3 points in the PDAI score and a PDAI score of <4, respectively. PDAI endoscopy subscore (maximum: 6) was also compared at entry and after the GMA therapy. Endoscopic healing was defined as a PDAI endoscopy subscore of 0.
Peripheral blood samples were collected for the measurement of white blood cell (WBC) count and C-reactive protein (CRP) before and after the GMA therapy. Patients provided a stool sample for the measurement of calprotectin and lactoferrin before and after the treatment. The faecal samples were stored at room temperature for immediate assay at the Kyoto Medical Science Laboratory (Kyoto, Japan). Faecal calprotectin was measured by an IDKR calprotectin enzyme-linked immunosorbent assay kit (Immundiagnostik, Bensheim AG, Germany). Faecal lactoferrin was determined by a sandwich enzyme-linked immunosorbent assay [Hirata et al. 2007]. Laboratory personnel were blinded to the clinical data.
Study endpoints
The primary endpoints were response and remission. Secondary endpoints include reduction of WBCs, CRP and faecal markers (calprotectin and lactoferrin), improvement of endoscopic index reflecting healing of pouchitis lesions (reduction of the PDAI endoscopy subscore), and tolerability of GMA therapy.
Statistics
Comparisons of frequencies were analysed using the Chi-square test with Yates’ correction. Continuous data are presented as the median values and range. Differences between median values were compared using the Mann–Whitney U test. The change in median values with time was evaluated by the Wilcoxon signed rank test. A p value <0.05 was considered to be statistically significant.
Ethical considerations
Prior to initiating this investigation, our study protocol was reviewed and approved by the Institutional Review Boards at the four study centres: Yokkaichi Hazu Medical Centre, The University of Tokyo, Yokoyama Gastrointestinal Hospital, and Hyogo College of Medicine. Consent was obtained from all included patients after they were informed of the study purpose and the nature of the procedures involved. Further, adherence was made to the Principle of Good Clinical Practice and the Helsinki Declaration at all times.
Results
The changes in the PDAI score during the GMA therapy in all patients are presented in Figure 1. The median PDAI score was 11 (range, 9–15) at entry and 9 (range, 6–13) after the GMA therapy, reflecting a significant decrease in disease activity following a course GMA therapy (p = 0.02). The median decrease in the PDAI score was 2 (range, –3 to 7). A total of six patients (46%) responded to the treatment, but at the time point we had set for the final efficacy assessments, none of the patients had achieved remission in terms of PDAI. The changes in the endoscopic subscore before and after the GMA therapy in all patients are shown in Figure 2. The median subscore was 5 (range, 4–6) at entry and 5 (range, 1–6) after the course of GMA therapy, reflecting no endoscopic changes (p = 0.10). Therefore, no patient achieved endoscopic healing.

The changes in the PDAI score during the GMA therapy in all patients. The median PDAI score was 11 (range, 9–15) at entry and 9 (range, 6–13) after the GMA therapy (p = 0.02).

The changes in the endoscopic subscore before and after the GMA therapy in all patients. The median subscore was 5 (range, 4–6) at entry and 5 (range, 1–6) after the treatment (p = 0.10).
Regarding laboratory measurements, neither WBC count nor CRP level significantly changed during the GMA therapy (Table 2). Similarly, neither faecal calprotectin nor lactoferrin levels significantly changed during the treatment (Table 2).
Changes in blood and faecal markers during the GMA therapy.

Data represent the median (range).
CRP, C-reactive protein; GMA, granulocyte and monocyte apheresis; WBC, white blood cell.
Predictive factors for clinical and endoscopic responses to GMA therapy were investigated (Table 3). The PDAI score and CRP level at entry were significant factors for clinical response. Patients with a higher PDAI score and those with a higher CRP level responded well to GMA therapy in the clinical assessment. Age, sex, duration from pouch construction to entry, endoscopic subscore, WBC count, and faecal calprotectin and lactoferrin levels did not appear to affect the response to GMA.
Correlation between responsiveness to GMA therapy and clinical and laboratory parameters.
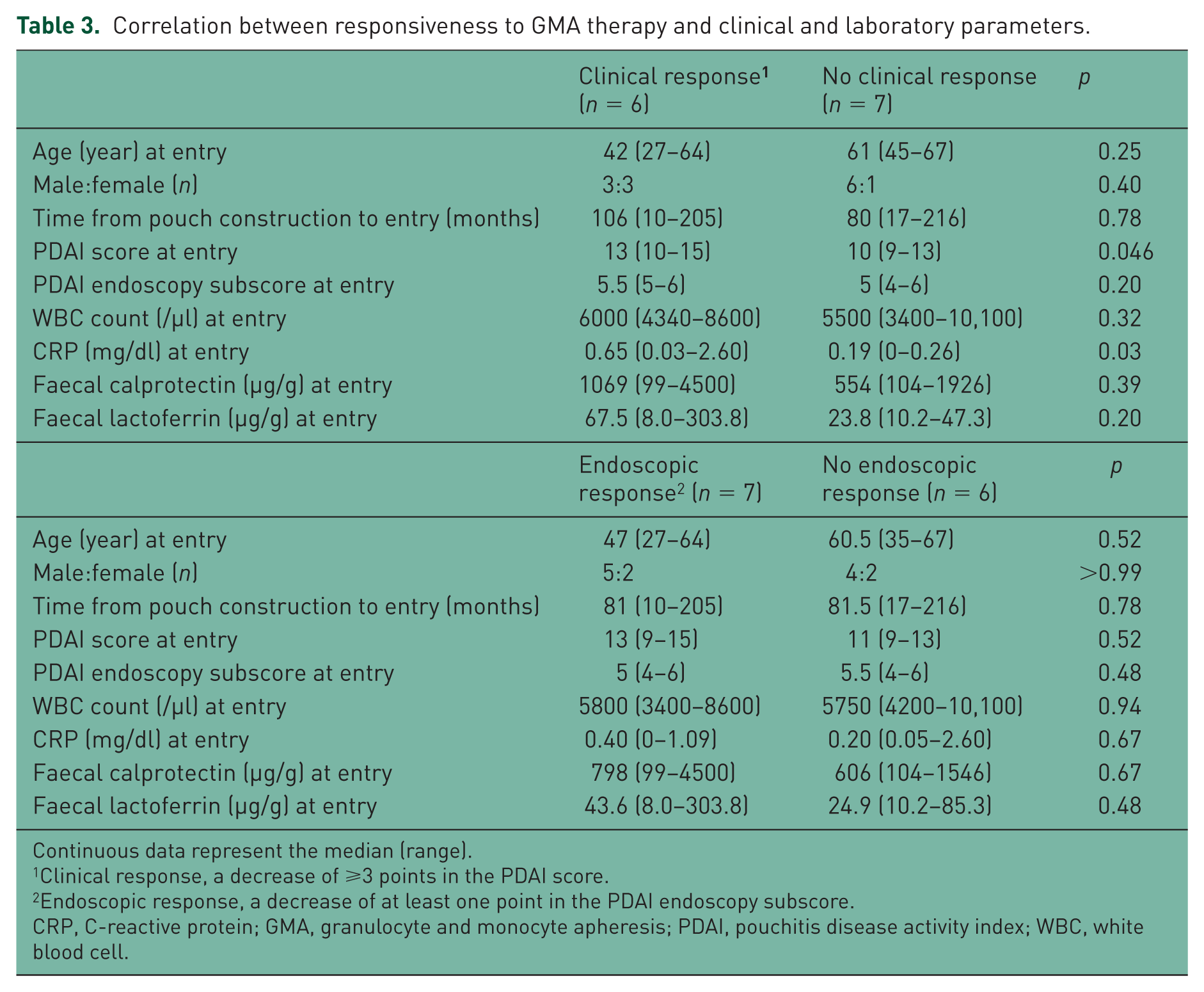
Continuous data represent the median (range).
Clinical response, a decrease of ⩾3 points in the PDAI score.
Endoscopic response, a decrease of at least one point in the PDAI endoscopy subscore.
CRP, C-reactive protein; GMA, granulocyte and monocyte apheresis; PDAI, pouchitis disease activity index; WBC, white blood cell.
Adverse events (AEs) were observed in two patients (15%), dyspnoea in one and transient headache in one during GMA therapy. These AEs were not serious, and all patients completed their 10 GMA sessions during this study. Patient compliance was 100%.
Discussion
Up to half of the patients who undergo IPAA may develop pouchitis as a serious complication of IPAA, and an additional morbidity factor in patients with IBD. Although the majority of patients with pouchitis respond favourably to antibiotic therapy, particularly in the initial stage of the disease, but in the longer term, in many patients pouchitis becomes refractory to conventional antibiotic therapy [Hurst et al. 1998; Shen and Lashner, 2008]. In a clinical practice setting, antibiotic-refractory pouchitis is often difficult to treat and is a common cause of pouch failure. Additionally, patients with antibiotic-refractory pouchitis may need to opt for salicylates, corticosteroids, immunosuppressive drugs, or anti-TNF biologics [Uchino et al. 2013; Herfarth et al. 2015]. However, corticosteroids, immunosuppressants and biologics are associated with serious adverse effects, potentially adding complexity to the underlying IBD [Toruner et al. 2008; Naganuma et al. 2013]. Given that pouchitis is a nonspecific inflammatory condition and elevated or activated myeloid lineage leucocytes are known sources of inflammatory cytokines [Yamamoto et al. 2006; Saniabadi et al. 2014], we thought that GMA, which selectively depletes myeloid lineage leukocytes might produce efficacy in patients with pouchitis. Generally, GMA with the Adacolumn is very much favoured by our patients for its good safety profile as well as for being a nonpharmacological intervention. Accordingly, in patients with active IBD, GMA has been applied to spare the patients from pharmacologics [Yamamoto et al. 2010; Dignass et al. 2016; Muratov et al. 2006; Yamamoto et al. 2006; Saniabadi et al. 2014].
However, to our knowledge, this is the first clinical trial with a major focus on evaluating the efficacy of GMA with the Adacolumn in patients with pouchitis after IPAA for UC. Although the sample size was small, a well-defined homogeneous group of patients with chronic antibiotic-refractory pouchitis was investigated. The median duration from pouch surgery to study entry was 81 months. In addition to antibiotics, the majority of the patients had active pouchitis while on conventional medical therapy including corticosteroids, amino-salicylates and anti-TNF biologics. Therefore, the included patients were among the most difficult to treat. Nonetheless, we found that the PDAI score was significantly decreased during the GMA therapy. Nearly half of the patients (46%) responded to the treatment, but without achieving complete remission. Patients with a higher PDAI score and those with a higher CRP level at entry appeared to respond well to GMA; however, these results should be confirmed in a large-scale study. Also, the endoscopic subscore was not significantly improved and none of the patients achieved complete endoscopic healing. Faecal and inflammatory biomarkers did not significantly decrease during the treatment. These were the outcomes in patients with drug-refractory pouchitis, and it may be interesting to investigate the efficacy of GMA in patients with pouchitis before the disease has become refractory to pharmacologics. This assertion is consistent with the observations made in patients with IBD when steroid naïve patients responded well, while the response in patients with drug refractory IBD was poor [Hanai et al. 2003; Suzuki et al. 2004; Yamamoto et al. 2007], or GMA was most effective when applied soon after a clinical relapse [Yokoyama et al. 2015; Saniabadi et al. 2014; Yamamoto et al. 2012].
One study evaluated the efficacy of another type of leukocytapheresis with Cellsorba filter column (LCAP) in active pouchitis [Araki et al. 2008]. A total of eight patients received LCAP weekly for 5 weeks along with baseline therapy including an antibiotic (metronidazole), probiotics, 5-ASA or corticosteroids. The median PDAI score significantly decreased from 9.5 (range, 8–10) to 4.0 (range, 2–9) during the LCAP therapy. Overall, six of the eight patients (75%) achieved remission defined as PDAI score of ⩽4. The inflammation in the pouch markedly improved after the treatment (endoscopic subscore not reported). No AE was observed. Therefore, there appears to be considerable difference in the efficacy of GMA and LCAP therapy; remission rate was 0% versus 75%. This may be due to the difference in type (clinical course) and severity of pouchitis between the two studies, and may not be due to the difference in apheresis devices. In our study with GMA, all patients had chronic refractory pouchitis. In contrast, in the other study with LCAP, the type of pouchitis was not clearly documented but we assume that the majority of their patients had treatment-responsive pouchitis [Araki et al. 2008]. Further, the median PDAI score at entry was higher in our study with GMA (11 versus 9.5).
In this study, GMA had a good safety profile, which is in line with the previous reports in patients with IBD [Hanai et al. 2003; Yokoyama et al. 2015; Saniabadi et al. 2014; Suzuki et al. 2004; Yamamoto et al. 2007, 2012]. Transient AEs during GMA therapy were a headache in one patient and dyspnoea in another patient, but both cases completed the GMA therapy as per the protocol. Therefore, in our small cohort of patients, compliance was 100%.
A major limitation of the current study was the small sample size. We extended the study duration from 1 year to 2.5 years; however, only 13 patients met the inclusion criteria even in these high-volume IBD centres. Most patients with pouchitis responded favourably to antibiotic therapy. Another limitation was its open-label and noncomparative study design. To rigorously evaluate the efficacy of GMA therapy for antibiotic-refractory pouchitis, a large-scale controlled study, preferably with a sham controlled group is warranted.
In conclusion, nearly half of our patients with chronic refractory pouchitis responded to the GMA treatment, but without achieving complete remission. Further, the endoscopic score was not significantly improved during the treatment. On the basis of these results, the efficacy of GMA therapy appears to be limited in the management of chronic refractory pouchitis. However, a large controlled study should be conducted to evaluate the efficacy of GMA therapy in patients with pouchitis in an earlier clinical stage, before the disease has become refractory to conventional medical therapy. Such a study should suit those who wish to be treated without drugs.
Footnotes
Acknowledgements
The authors would like to thank all colleagues who helped in conducting this study.
Takayuki Yamamoto was involved in the study design, as well as in the planning, conducting, and collection and interpretation of data for this study and in drafting/editing the manuscript. Toshiaki Tanaka, Tadashi Yokoyama, Takahiro Shimoyama, Hiroki Ikeuchi and Motoi Uchino were involved in the planning, collection and interpretation of data for this study, and in drafting the manuscript. Toshiaki Watanabe was involved in editing the manuscript. All the above-mentioned authors have approved the final draft submitted.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
Tadashi Yokoyama received consultancy fees and research funding from EA Pharmaceuticals Co. Ltd. (Tokyo, Japan). Takayuki Yamamoto, Toshiaki Tanaka, Takahiro Shimoyama, Hiroki Ikeuchi, Motoi Uchino and Toshiaki Watanabe have no conflict of interest to disclose.