
Abstract
Advanced imaging techniques used in the management of Barrett’s esophagus include electronic imaging enhancement (e.g. narrow band imaging, flexible spectral imaging color enhancement, and i-Scan), chromoendoscopy, and confocal laser endomicroscopy. Electronic imaging enhancement is used frequently in daily practice, but use of the other advanced technologies is not routine. High-definition white light endoscopy and random four quadrant biopsy remain the standard of care for evaluation of Barrett’s esophagus; this is largely due to the value of advanced imaging technologies not having been validated in large studies or in everyday practice. A new advanced imaging technology called volumetric laser endomicroscopy is commercially available in the United States. Its ease of use and rapid acquisition of high-resolution images make this technology very promising for widespread application. In this article we review the technology and its potential for advanced imaging in Barrett’s esophagus.
Introduction
Esophageal adenocarcinoma is the predominant esophageal cancer in North America and Europe [Ingelfinger et al. 2014]. In the past few decades its incidence has increased sharply, more than any other malignancy [Pohl and Welch, 2005]. The culprit precursor lesion for this tumor is Barrett’s esophagus, which is defined as the presence of specialized (or goblet cell) intestinal metaplasia confirmed on biopsy of the tubular esophagus. The presence of Barrett’s esophagus increases the risk of esophageal cancer by 30–50 fold [O’Connor et al. 1999; Sharma et al. 2006; Wani et al. 2009]. The presence of dysplasia in Barrett’s esophagus significantly increases the risk of progression to neoplasia. Therefore screening and surveillance recommendations have been endorsed for patients with Barrett’s esophagus to survey for dysplasia [Shaheen et al. 2016]. Despite these guidelines, the incidence of esophageal cancer continues to rise [Pohl and Welch, 2005]. Many patients diagnosed with esophageal cancer have never experienced the symptoms of gastrointestinal reflux, and therefore they have never been screened with an upper endoscopy or received a diagnosis of Barrett’s esophagus [Rubenstein and Thrift, 2015]. However, even patients with a known diagnosis of Barrett’s esophagus and who have had endoscopies showing nondysplastic intestinal metaplasia can develop high-grade dysplasia or cancer. In a large multicenter cohort of 1376 patients who developed high-grade dysplasia or cancer, half of them had two prior consecutive endoscopies showing nondysplastic Barrett’s esophagus [Sharma et al. 2006]. This implies that the current standard for detecting dysplasia is not optimal.
The accepted standard for tissue acquisition for detecting dysplasia is the Seattle protocol, where four-quadrant forceps biopsies are taken every 1–2 cm throughout the length of the Barrett’s esophagus segment, which is characterized by salmon-colored mucosa [Levine et al. 1993]. Although this approach can increase the yield of diagnosis of early neoplasia compared with other sampling methods, it is prone to sampling error and is both time consuming and costly [Falk et al. 1999; Gonzalez-Haba and Waxman, 2015]. Therefore, advanced imaging technology in Barrett’s esophagus to identify ‘red flag lesions’ is needed to reduce or even eliminate random biopsies and focus sampling instead on targets suspicious for dysplasia and neoplasia. Advanced imaging techniques are coined ‘red flag technology’ because lesions detected draw the attention of the endoscopist to targets for sampling or even endoscopic removal [Gonzalez-Haba and Waxman, 2015].
Currently available advanced imaging techniques include confocal laser endomicroscopy (CLE) and various forms of chromoendoscopy [Qumseya et al. 2013; Sharma et al. 2015]. Although these technologies have been shown to increase the yield of dysplasia detection, they are not widely recommended in current guidelines. The main reason for this is that these results have only been achieved in tertiary care settings and in small cohorts [Sharma et al. 2015]. In addition, CLE only provides a small field of view and thus requires extensive time to visualize a large segment of Barrett’s esophagus. Further, a limited time for mucosal evaluation is available before the fluorescein dye injected intravenously infiltrates the mucosa and obscures further tissue inspection. Thus, an optimal tool would be a red flag technology that can evaluate a large field of view at a high level of resolution [Anandasabapathy, 2013].
Volumetric laser endomicroscopy (VLE) is a second-generation optical coherence tomography (OCT) imaging technique that has the potential to be the optimal red flag technology for providing a high-resolution large field of view in order to detect dysplasia and neoplasia. In this review, we discuss the science of VLE, along with recent data on the value and clinical utility of VLE for imaging Barrett’s esophagus.
OCT and VLE
OCT can produce high-resolution cross-sectional images of the esophagus. It is very similar to endosonography but uses infrared light instead of an acoustic signal [Evans et al. 2006; Poneros et al. 2001]. The axial resolution of OCT (10 µm) is 10 times better than that of high-frequency (100 µm) endoscopic ultrasound (EUS) [Poneros et al. 2001; Sergeev et al. 1997; Tearney et al. 1996, 1997]. Although the resolution is superior to EUS, the depth of tissue penetration is less. Light reflectivity of esophageal tissue is measured, using an OCT probe that is passed through the endoscope channel and contacts the mucosa. This creates real-time images that allow the detection of mucosal surface changes and glandular architecture on a microscopic scale, facilitating detection of intestinal metaplasia [Brand et al. 2000; Sivak et al. 2000].
Recently, the second-generation OCT system, VLE, has become commercially available (NinePoint Medical Inc., Bedford, MA, USA). It is a balloon-based frequency domain OCT that contains a probe for faster real-time imaging. The balloon allows the centering of the probe while helically scanning optics. Based on the scattering of light from different structures within the wall of the esophagus, an image can be created. VLE can scan a 6 cm length of the esophagus in approximately 90 seconds, providing surface and subsurface wide-field cross-sectional imaging with a resolution as low as 7 mm, and to a depth of 3 mm. This allows for high-resolution imaging of the entire mucosal and submucosal layers of the esophagus within a short period of time [Bouma et al. 2000; Suter et al. 2008; Vakoc et al. 2007]. Figure 1 shows a schematic of how this technology functions to produce the image.
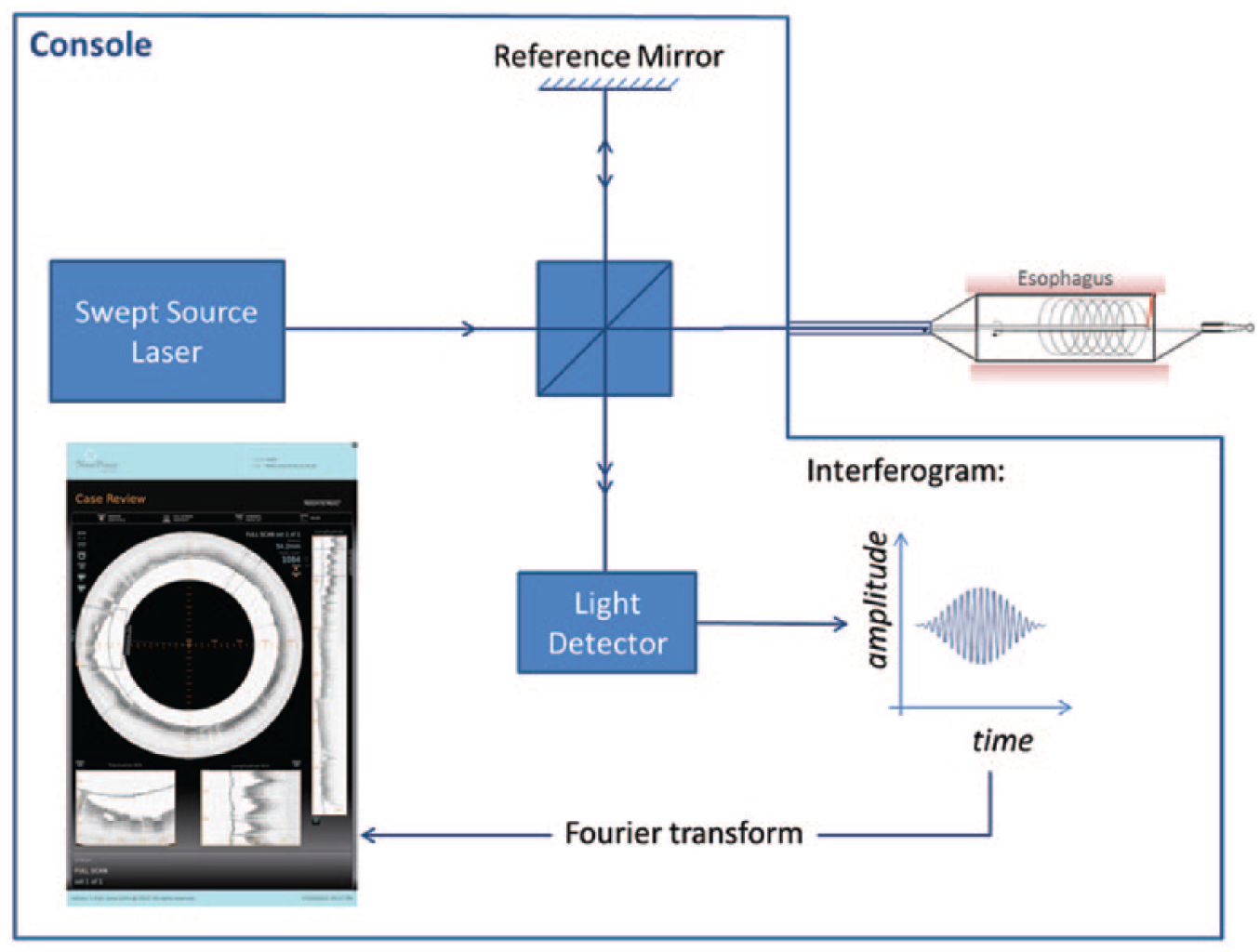
Schematic depicting how VLE functions to obtain a high-resolution image of the esophagus.
The safety and feasibility of VLE was recently evaluated in a prospective multicenter trial of 100 patients [Wolfsen et al. 2015]. VLE could be performed in 87% of the cases, while 13% could not be performed secondary to probe and console issues. However this study was performed using an older version of the console and probe, and our experience suggests completion rates higher than this. More importantly, this study showed VLE was well-tolerated and able to visualize the mucosa and submucosa in the patients when VLE was performed.
Image acquisition of VLE
The VLE imaging system consists of a console, monitor, and optical probe (Figure 2a). The optical probe is designed to fit in a standard adult gastroscope channel (Figure 2b). The probe is commercially available in 14 mm, 17 mm, and 20 mm diameter balloons that are 6 cm in length. In our practice, if the esophagus is not tortuous or if there is no stricture, a 20 mm balloon can be used in all cases. The balloon is positioned such that the distal margin of the balloon and scan is located 1 cm distal to the gastroesophageal (GE) junction. This allows a single scan to image the gastric cardia, the GE junction, and the distal esophagus. After the balloon is positioned so that it is straight and there is no kink, it is inflated to around 10–15 psi, depending on the anatomy. A scout scan is obtained to allow for repositioning longitudinally. If the balloon is not centered optimally, the balloon pressure can be increased to as high as 25 psi; however in the presence of a stricture, the physician’s discretion must be used, given the risk for perforation. Imaging is performed by automatic helical pullback of the probe from the distal to proximal end of the balloon over a 90 second period, creating real-time 360° volumetric images. A total of 1200 cross-sectional scans are generated over the 6 cm segment. VLE scans are viewed by using a software interface that allows real-time viewing of cross-sectional transverse and longitudinal views.

(a) Nvision volumetric laser endomicroscopy console. (b) Nvision VLE optical probe with the centering balloon. (c) schematic of the balloon inflated in the esophagus with the probe imaging.
A registration line is seen on the balloon and its orientation is matched up with the registration line seen on the cross-sectional imaging (viewed as a thin shadow line) to allow clock face orientation and therefore targeting of any abnormalities seen. Lesions are localized via triangulation, using both the relation of the lesion to the GE junction and the registration line. If multiple scans are required to visualize a long segment of Barrett’s esophagus, unique targets are visualized on both scans to overlap them accurately. Some endoscopists place electro cautery marks along the length of the Barrett’s segment that can be visualized on the VLE scan. This is done in an effort to align multiple scans accurately to help target lesions. The safety of this technique has not been evaluated.
Once lesions are detected on the VLE scan that are suspicious for dysplasia, the corresponding endoscopic area can be biopsied. Endoscopic mucosal resection can be considered if the abnormal area on the VLE scan is located deeper below the mucosal surface.
Development of a laser-marking device will make targeting more precise [Suter et al. 2014]. The technology will be updated to allow placement of a cautery mark adjacent to an abnormal area to be targeted by the endoscopist. This will allow more precise targeting of a pathologic lesion, and may make a decision to perform endoscopic mucosal resection easier and less concerning to the physician.
VLE features of gastric cardia, esophageal squamous mucosa, and intestinal metaplasia
VLE is able to differentiate between normal gastric mucosa, normal squamous mucosa, and intestinal metaplasia [Sauk et al. 2013]. VLE features of normal gastric cardia include vertical pit and crypt architecture, high surface reflectivity, poor image penetration, and presence of rugal folds (Figure 3). VLE features of esophageal squamous mucosa include layered horizontal architecture without glands in the epithelium (Figure 4). The GE junction can be visualized on VLE imaging at the interface between these two types of features. VLE features of intestinal metaplasia include (1) loss of layered architecture in the setting of no surface pits and crypts (Figure 5a) or (2) glands seen in the epithelium (Figure 5b) [Evans et al. 2007].
VLE image of the gastric cardia showing vertical pit and crypt architecture, high surface reflectivity, poor image penetration, and presence of rugal folds. Scale bar is 1 mm. Reprinted from Wolfsen and colleagues [Wolfsen et al. 2015] with permission from Elsevier.
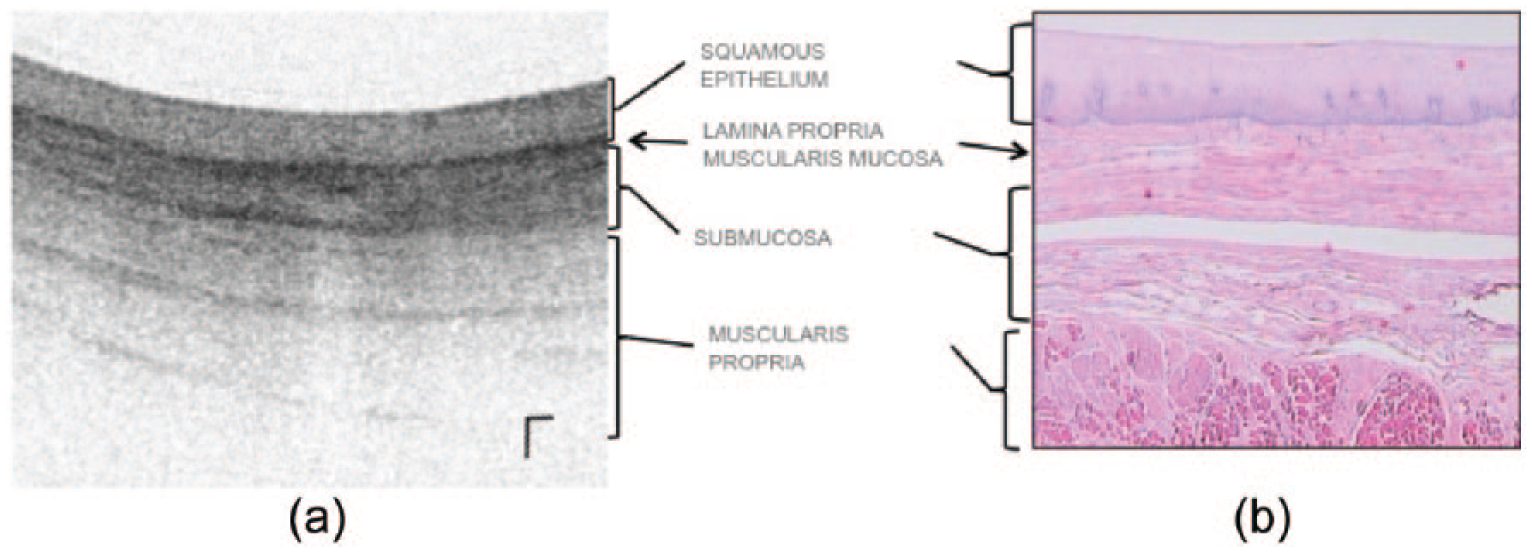
(a) VLE image of normal squamous mucosa with the layered architecture without glands. Scale bar is 1 mm vertical and horizontal. (b) Corresponding normal histology (not from the same patient).

(a) VLE image showing loss of layered architecture in the setting of no surface pits and crypts. The red arrow points to complete effacement. The green arrow points to partial effacement. (b) Atypical glands (yellow arrows) with loss of layered architecture. Scale bar is 1 mm vertical and horizontal.
Dysplasia detection
The goal of red flag imaging is to help locate and target dysplasia so that ablation therapies can be employed to reduce the risk of progression to esophageal adenocarcinoma. There is level-one evidence that ablation of low grade and high grade dysplasia can eliminate the progression to esophageal cancer [Phoa et al. 2014; Shaheen et al. 2009]. However the challenge can be finding focal dysplasia and neoplasia, especially in a long segment of Barrett’s esophagus. Without locating these abnormalities, ablative endoscopic therapy cannot be provided.
There are features of OCT imaging that can help target dysplasia. Glandular architecture and signal intensity are two main components to determining whether dysplasia is present [Evans et al. 2006; Leggett et al. 2015]. An OCT scoring index (OCT-SI) was created in 2006 to aid in the OCT diagnosis of Barrett’s esophagus-associated dysplasia. The scoring system weights the two components to obtain the score. The scoring system is outlined in Figure 6. A score greater than or equal to 2 is associated with a sensitivity of 83% and a specificity of 75% for dysplasia.
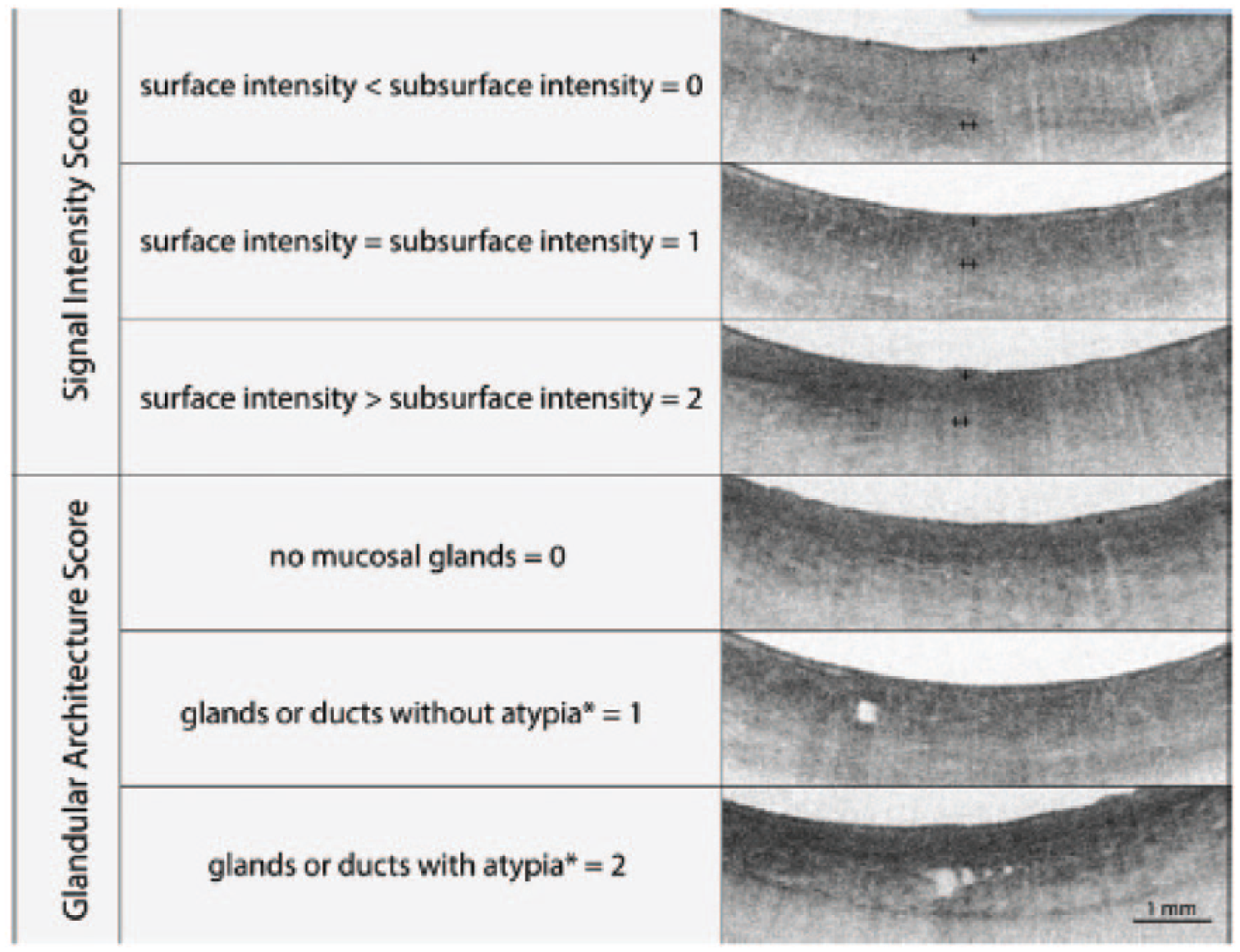
OCT scoring index (OCT-SI). A score greater than or equal to 2 is associated with a sensitivity of 83% and a specificity of 75% for dysplasia. The surface intensity is designated by a + and the subsurface intensity by ++. Reprinted from Leggett and colleagues [Leggett et al. 2015] with permission from Elsevier. *Glandular atypia is defined by the presence of irregular and/or dilated glands.
Recently, Leggett and colleagues devised a new algorithm for the detection of dysplasia based on ex vivo endoscopic mucosal resection specimens scanned with VLE. This index is called the VLE diagnostic algorithm (VLE-DA) [Leggett et al. 2015]. The algorithm is outlined in Figure 7. The algorithm first determines the degree of mucosal effacement (partial versus full loss of layered mucosal architecture). If complete effacement is seen and the surface intensity is greater than the subsurface, then dysplasia is suspected. If partial effacement is seen with greater than five atypical glands, then dysplasia also is suspected. This study highlights a new finding; partial effacement and the number of atypical glands may be associated with the presence of dysplasia on VLE. This VLE-DA had a sensitivity of 86% (95% CI 69–96) and a specificity of 88%. (95% CI, 60–99). In vivo studies using the VLE-DA need to be performed to confirm this high sensitivity and specificity for diagnosing dysplasia.

VLE diagnostic algorithm (VLE-DA) index. This VLE-DA had a sensitivity of 86% (95% CI 69–96) and a specificity of 88%. (95% CI, 60–99). Reprinted from Leggett and colleagues [Leggett et al. 2015] with permission from Elsevier.
Although the OCT-SI was created based on in vivo imaging and correlation to histology from biopsy samples from patients in a clinical setting, this has yet to be performed with VLE. The VLE-DA by Leggett and colleagues is based on ex vivo imaging [Leggett et al. 2015]. Thus, a limitation of VLE is the correlation of in vivo images in current practice to histology of low-grade dysplasia, high-grade dysplasia, or cancer.
Current practice of VLE
VLE is currently cleared by the Food and Drug Administration (FDA) for use in the esophagus in the United States. In our practice, we use it routinely for advanced imaging during surveillance of nontreated disease or Barrett’s segments soon to be treated. In addition, we use it after post-ablation therapy for surveillance to target suspected intestinal metaplasia or dysplasia. VLE is able to identify subsquamous glands and subsquamous intestinal metaplasia [Leggett et al. 2014; Swager et al. 2016], making it a promising tool for surveillance following endoscopic ablation.
We recently published a case of a patient that underwent surveillance endoscopy twice for management of a long segment of Barrett’s esophagus where the pathology from random biopsies were indefinite for dysplasia [Trindade et al. 2015]. This patient had no areas to target based upon inspection with narrow-band imaging and high-definition white light endoscopy. The patient was referred for endoscopy with VLE. VLE showed an area where there was a loss of layered architecture, complete effacement of the mucosal layer, a surface intensity greater than the subsurface, and atypical glands (Figure 8). Both the OCT-SI and VLE-DA would indicate this area had a high suspicion for dysplasia. VLE-targeted biopsies were performed with a jumbo biopsy forceps, and the histology was consistent with high-grade dysplasia. Random biopsies performed during the same endoscopy following the Seattle Protocol were negative for dysplasia. VLE provided a diagnosis of neoplasia and thus an indication for radiofrequency ablation. Leggett and colleagues published a case in which VLE targeted a subsquamous Barrett’s adenocarcinoma after post-ablation therapy [Leggett et al. 2014]. VLE was able to image this abnormality while CLE or white light endoscopy could not. These two cases show the utility of VLE for targeting neoplasia, both before and after endoscopic treatment of Barrett’s esophagus.
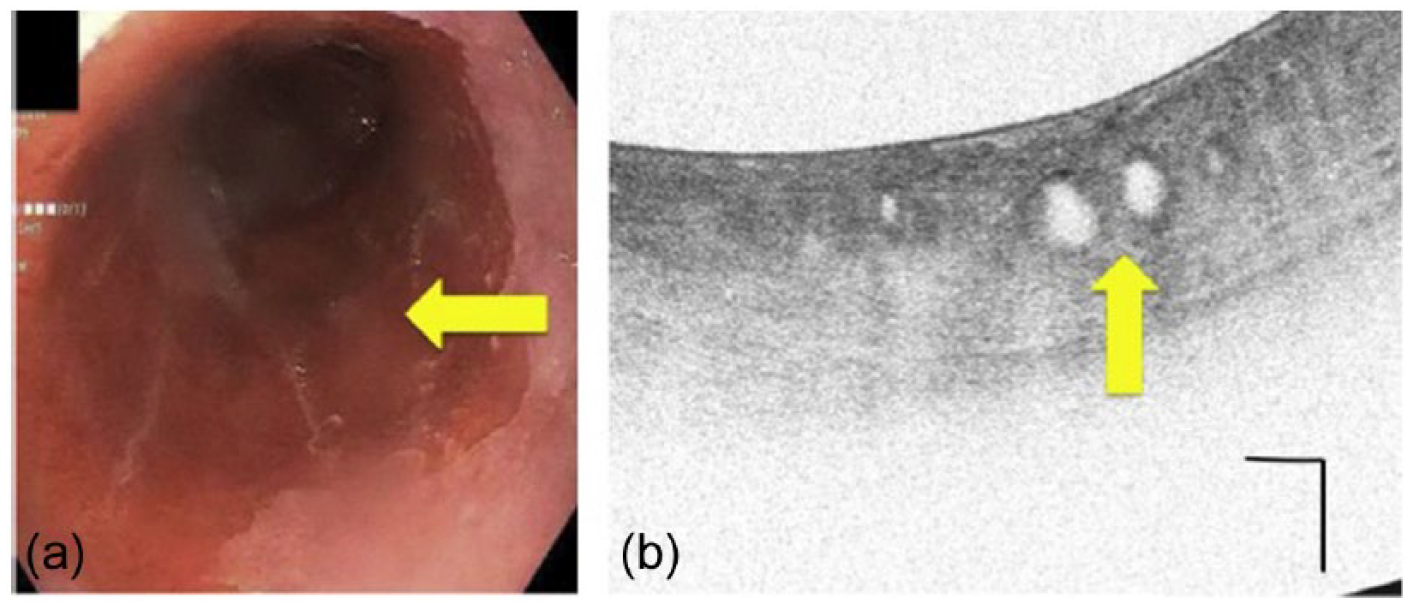
Case showing a long segment of Barrett’s esophagus (a) that was previously biopsied twice and showed indefinite for dysplasia. VLE was performed that showed the focal abnormality (b) that allowed a targeted biopsy. The yellow arrows correspond to the area on endoscopy (a) and atypical glands on VLE (b). Scale bar is 1 mm vertical and horizontal in panel b. Reprinted from Trindade and colleagues [Trindade et al. 2015] with permission from Elsevier.
Research studies are needed to confirm these clinical experiences. As mentioned earlier, in vivo image correlation of the grade of neoplasia to histology is needed. Studies are needed to assess the sensitivity and specificity of VLE compared with histology. Ideally, a prospective study comparing VLE-targeted versus random biopsies for dysplasia yield is needed to support the use of VLE on a larger scale. It is expected that these studies will be performed once improved targeting via laser marking is in active use. There is an ongoing national registry for VLE in the United States that will help answer some questions on yield, sensitivity, and specificity of VLE. Moreover, analyses will need to be performed to determine if this new technology is cost-effective for everyday use.
As a relatively new technology with limited available data in the peer-reviewed literature, VLE is not currently recommended for routine widespread clinical use in published clinical guidelines for the management of Barrett’s esophagus [Shaheen et al. 2016]. It should be noted that the guidelines do not recommend other advanced imaging modalities, despite studies showing increased yield in diagnosis of dysplasia [Qumseya et al. 2013; Sharma et al. 2015]. This is due to these techniques not being validated in larger cohorts or in a community setting since most advanced imaging is performed in tertiary centers. However, expert panels do condone the use of advanced imaging in the centers that perform advanced imaging with good diagnostic accuracy [Sharma et al. 2015].
Conclusion
VLE is a new advanced imaging technology for Barrett’s esophagus with considerable promise given its ease of use, ability to quickly obtain high-resolution images quickly, and the wide field of imaging obtained in a single scan. If future studies show that VLE increases dysplasia yield with an acceptable sensitivity and specificity, this technique may become a popular choice for an approach to advanced imaging of Barrett’s esophagus. For the near future, use of VLE will be restricted to tertiary centers until larger studies are available that support its use in the community.
Footnotes
Acknowledgements
We are grateful to the authors whose figures (Figures 3, 6, 7, and 8) were used with permission by Elsevier publishing. The conception and design of this article was conducted by A. Trindade and D. Pleskow; all other aspects of the article production, review and data analysis were contributed to equally by all authors.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The authors declare no conflicts of interest in preparing this article.