
Abstract
Introduction
Barrett’s esophagus (BE), intestinal metaplasia of the distal esophageal epithelium, is likely the obligate precursor to the development of esophageal adenocarcinoma (EAC). Given that gastroesophageal reflux disease (GERD) is a known risk factor for EAC [Shaheen and Ransohoff, 2002; Lagergren et al. 1999] and BE [Conio et al. 2002; Lieberman et al. 1997], a causative role has been proposed for the contribution of acid reflux to the development of BE and to the subsequent progression of BE to EAC. Accordingly, it has become standard clinical practice to treat BE patients with proton-pump inhibitors (PPIs), with the goal of preventing further injury to the esophageal mucosa and thereby reducing the risk of neoplastic progression [Wang and Sampliner, 2008].
Despite the high prevalence of PPI use in patients with BE, it is unknown whether these medications actually decrease the risk of developing EAC. Further, by inhibiting acid production in the stomach, long-term PPI use can lead to increased serum gastrin levels, and can cause marked hypergastrinemia in a subset of patients [Jansen et al. 1990; Koop et al. 1990]. This effect is concerning, as several studies have shown gastrin to have tumorigenic effects, including increased cellular proliferation [Ferrand and Wang, 2006]. In addition, hypergastrinemia has been associated with an increased risk of developing certain human neoplasms, such as colorectal cancer [Georgopoulos et al. 2006; Thorburn et al. 1998].
More recently, our research group reported that in patients with BE, elevated serum gastrin is associated with a history of high-grade dysplasia or EAC [Wang et al. 2010]. Given the known proliferative and carcinogenic effects of gastrin, this finding suggests that hypergastrinemia may potentially contribute to the neoplastic progression of BE in a subset of patients. The present pilot study therefore aims to examine the correlation between serum gastrin and tissue staining with Ki-67, a well-studied marker for cellular proliferation, in nondysplastic BE patients on PPI therapy.
Methods
Study subjects
Subjects for the present study were chosen as a subset of patients enrolled as part of a prior study [Wang et al. 2010]. These patients, who were recruited from the clinical practices of two of the investigators (CJL and JAA), all had biopsy-proven BE and were already scheduled to undergo upper endoscopy. Additional inclusion criteria included at least daily PPI use at the initial diagnosis of BE and age ≥18 years. PPI dosage and frequency were confirmed to have remained unchanged during the 2 weeks prior to study enrollment. Exclusion criteria included history of gastric or esophageal surgery, or inability to provide informed consent. For the present study, only those patients with no history of dysplasia and who had serum and tissue collected on the same day were chosen for analysis.
Data were collected on patient age, gender, race and ethnicity, PPI use, and aspirin or other nonsteroidal anti-inflammatory drug (NSAID) use. The duration of PPI use in months was also recorded. Histological interpretation was performed by at least one pathologist experienced in BE, and the pathologists were unaware of the gastrin or Ki-67 results.
This study was approved by the Columbia University Institutional Review Board.
Sample collection
On the day of endoscopy, 10 ml of blood was drawn by sterile peripheral venipuncture. All patients fasted for at least 8 hours in preparation for upper endoscopy. During the endoscopy, BE length was measured and four quadrant random biopsies were taken every 1–2 cm along the length of BE for pathologic evaluation. Two random biopsies were taken from the gastric antrum to evaluate for the presence of Helicobacter pylori.
Sample processing and radioimmunoassay
Whole blood of subjects was centrifuged at 2700 rpm (1600 g) for 10 min to separate out serum, which was then stored at –80°C until shipment. Serum gastrin concentrations were determined by radioimmunoassay, as described previously [Nemeth et al. 1992]. Quantitative serum gastrin concentrations were reported in pM. The individuals performing the quantitative gastrin assays were blinded to the histological classification and Ki-67 index of the tissue samples.
Immunohistochemistry
The most distal level of esophageal biopsies that contained intestinal metaplasia was chosen for immunohistochemical analysis. Paraffin sections fixed in 10% formalin were incubated with primary Ki-67 antibody (Abcam 15580). Biotinylated secondary antibodies (Jackson Immunoresearch Laboratories Inc., West Grove, PA) and ABC avidin–biotin–DAB detection kit (Vector Labs) were used for detection and visualization according to supplied protocol. Epithelial cells were evaluated from five representative crypts containing goblet cells in each of five separate high-power fields. Ki-67 index was calculated by dividing the number of cells with positive nuclear staining by the total number of cells counted.
Statistical analysis
Categorical variables were evaluated using Fisher’s exact tests, and continuous variables were compared using Wilcoxon rank sum tests. A nonlinear relationship between Ki-67 and gastrin was apparent upon examination of a Q–Q plot. Therefore, logarithmic transformation of serum gastrin was performed, and Pearson’s correlation coefficient was calculated for the relationship between Ki-67 index and ln(gastrin). Linear regression modeling was performed to assess for associations between Ki-67 index and ln(gastrin), adjusted for potential confounders. Given the small sample size, only bivariate modeling was performed. All tests were two-sided, and statistical significance was defined as p < 0.05. All analyses were performed using STATA 11.1 (STATACorp, College Station, TX).
Results
Characteristics of study patients with nondysplastic Barrett’s esophagus.
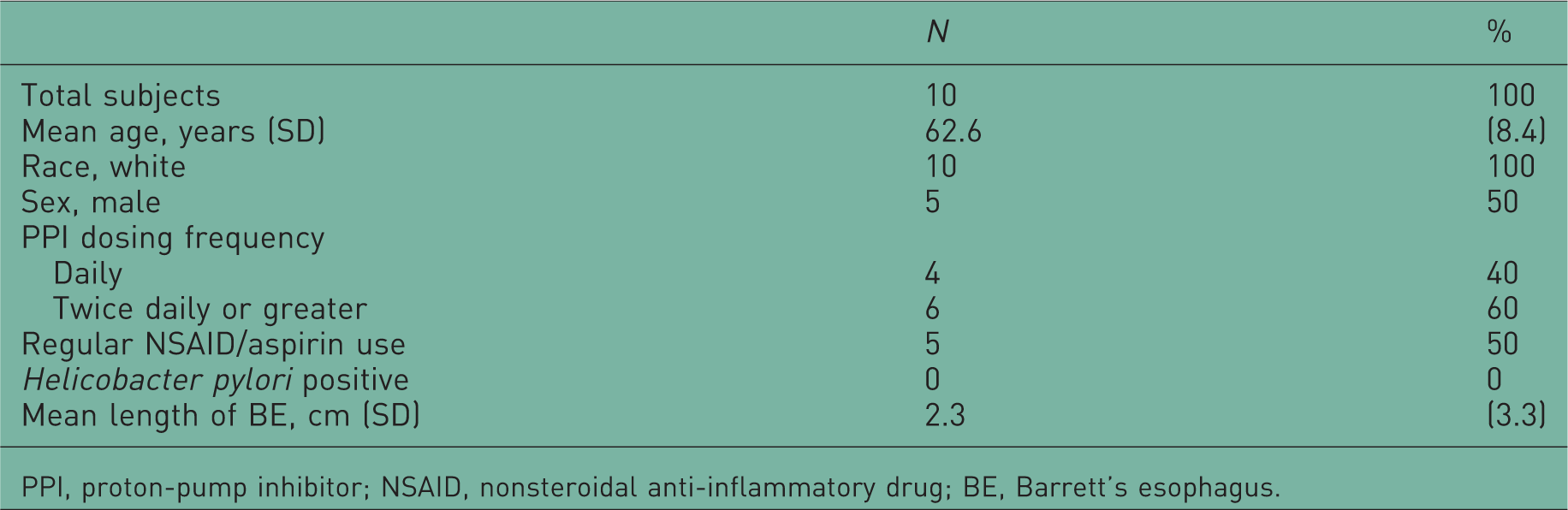
PPI, proton-pump inhibitor; NSAID, nonsteroidal anti-inflammatory drug; BE, Barrett’s esophagus.
The median serum gastrin level was 45.2 pM (IQR 23–64) and the median percentage of cells staining positive for Ki-67 nuclear antibody was 49.6% (IQR 45.6–55.8%) (Figure 1). There was no significant association between Ki-67 index and age, sex, PPI dose, duration of PPI use, aspirin/NSAID use, or BE length.
Photomicrograph of a representative Barrett’s gland stained with Ki-67 nuclear antibody.
There was a statistically significant correlation between Ki-67 index and ln(gastrin) (r = 0.64, p = 0.05) (Figure 2). This association was not altered qualitatively by adjusting for individual potential confounders, including age, sex, PPI dose, and duration of PPI use.
Significant correlation between Ki-67 index and ln(gastrin) in patients with nondysplastic Barrett’s esophagus.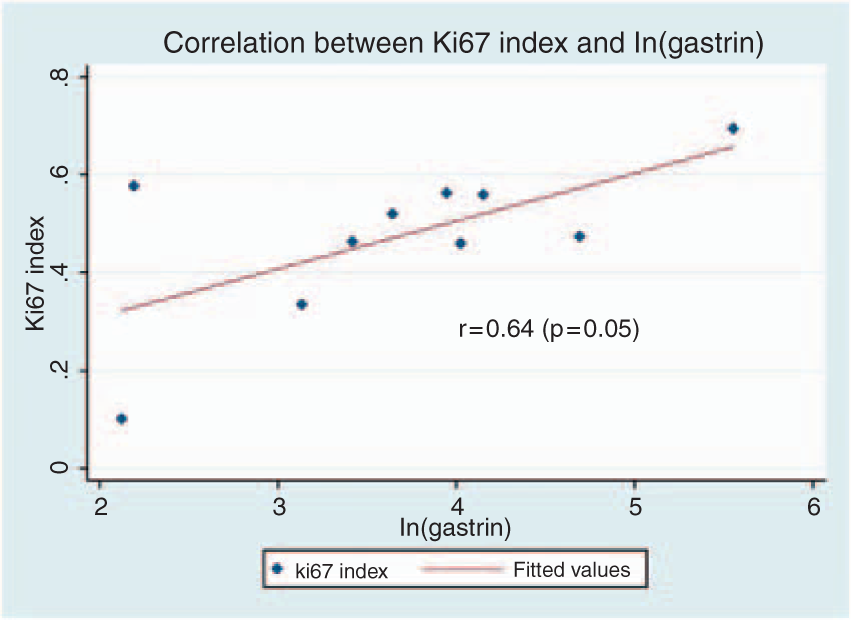
Discussion
In this pilot study we performed a cross-sectional analysis of patients with nondysplastic BE and found a significant positive correlation between serum gastrin levels and epithelial cell proliferation of Barrett’s tissue, suggesting that gastrin may directly stimulate cellular proliferation in BE.
Hypergastrinemia has been associated with advanced neoplasia in BE and other gastrointestinal premalignant and malignant conditions. In a case–control study comparing patients with colorectal adenomas to normal controls, serum gastrin levels were significantly higher in patients with adenomas, and hypergastrinemia (serum level >110 pg/ml) was also observed more frequently in these cases [Georgopoulos et al. 2006]. In a separate large case–control study, elevated gastrin (serum level >90 pg/ml) was associated with an increased risk of colorectal cancer (adjusted odds ratio [OR]: 3.9, 95% confidence interval [CI]: 1.5–9.7) [Thorburn et al. 1998]. The results of these studies parallel our recent findings in BE, in which subjects with the highest quartile of serum gastrin levels had a fivefold increased odds of high-grade dysplasia or adenocarcinoma [Wang et al. 2010]. The results of our current pilot study provide evidence for biological plausibility that gastrin may affect neoplastic progression in these patients.
Numerous investigational efforts have focused on identifying the role of gastrin in cancer. Gastrin has a demonstrated effect on loss of cell–cell adhesion, inhibition of apoptosis, invasion, and, most importantly, cellular proliferation [Ferrand and Wang, 2006]. Gastrin exerts its effects mainly through activation of the cholecystokinin-2 receptor (CCK2R) [Ferrand and Wang, 2006]. CCK2R is overexpressed in BE and EAC [Harris et al. 2004; Haigh et al. 2003], and gastrin likely stimulates proliferation of Barrett’s epithelium through activation of this receptor. Haigh and colleagues showed that Barrett’s tissue not only expresses twice the number of CCK2 receptors as normal squamous esophageal epithelium, but also that incubation of Barrett’s tissue with amidated gastrin induces increased cellular proliferation, which can be abolished by treatment with a CCK2R antagonist [Haigh et al. 2003]. Moreover, in vitro and in vivo, exogenously applied gastrins (G17, gly-G17, and progastrin) promote growth in various gastrointestinal cancer cell lines [Grabowska and Watson, 2007], and transgenic mice that overexpress amidated gastrin are more likely to develop gastric adenocarcinoma [Fox et al. 2003; Wang et al. 2000].
For the current study, the proliferative activity of the esophageal epithelial cells was estimated by staining with Ki-67, an antibody that recognizes a nuclear antigen present exclusively in proliferating cells [Gerdes et al. 1984]. Higher degrees of Ki-67 staining have been shown to correlate with increasing grades of dysplasia in Barrett’s tissue [Binato et al. 2009; Feith et al. 2004; Rioux-Leclercq et al. 1999; Polkowski et al. 1995]. In addition, a retrospective case–control study demonstrated that a Ki-67 index >20% in BE patients with low-grade dysplasia was associated with an increased risk of developing high-grade dysplasia or EAC [Sikkema et al. 2009], indicating that the proliferative rate of Barrett’s tissue not only increases with increasing stages of neoplastic progression, but that excessive proliferation may also be a marker for risk of progression.
The present study benefitted from carefully selected inclusion criteria for study subjects, which were designed to maximally reduce potential confounders. All patients had biopsy-proven BE, without any history of dysplasia, and they had all been taking PPIs for at least 2 weeks prior to enrollment. In addition, all serum samples were collected on the same day as tissue biopsies to ensure that tissue analysis coincided with current gastrin levels. Ki-67 is widely accepted as a good marker of tissue growth, and correlates well with other measures of cellular proliferation [Guzinska-Ustymowicz et al. 2009].
As a pilot study, there were certain limitations. The sample size of study subjects was small (n = 10). Nevertheless, the reported correlation was robust enough to show statistical significance despite the small sample size. Another potential limitation was the measurement of only a single serum gastrin level for each patient; the degree of variability of serum gastrin within an individual over time is unknown. For this study, gastric biopsies were only obtained from the antrum, and therefore some cases of H. pylori may have been missed.
In summary, the results of this pilot study demonstrate that serum gastrin appears to correlate with cellular proliferation in patients with nondysplastic BE. This finding suggests that a mechanism may exist by which elevated serum gastrin increases the risk of neoplastic progression in patients with BE. Larger studies are still needed to confirm these findings, and investigations are currently underway to examine the relationship between serum gastrin and gastrin precursors with histology and CCK2R expression in BE patients. Ultimately, longitudinal studies are needed to determine whether hypergastrinemia actually increases the risk of progression of BE to dysplasia and adenocarcinoma or can be used as a helpful biomarker for disease progression.
Footnotes
Funding
This study was supported in part by the Doris Duke Charitable Foundation (DAG), a Ruth L. Kirschstein National Research Service Award (CMM), the Digestive Disease Research Foundation (BJV), and the National Cancer Institute (JAA; grant number K07 CA 132892).
Conflict of interest statement
None declared.
Acknowledgment
The authors would like to thank Dr Andrea Varro for running the original gastrin assays.