
Abstract
Systemic sclerosis is a rare autoimmune disorder that affects multiple organ systems, including the lungs, kidneys, and liver, and often leads to fatal complications. Adrenocortical adenoma, a benign tumor, can secrete hormones such as cortisol, resulting in symptoms including hypertension, diabetes, and obesity, although it can also be asymptomatic. This article presents a case of a patient with systemic sclerosis and adrenocortical adenoma, detailing the diagnostic and therapeutic journey before and after laparoscopic adrenal tumor resection. It offers insights into the clinical management of such cases and analyzes how surgical removal of the adenoma affects the treatment and prognosis of systemic sclerosis. This study aimed to provide valuable knowledge to healthcare professionals managing patients with this dual diagnosis, further contributing to the medical understanding of treatment outcomes in such cases.
Keywords
Introduction
Systemic sclerosis (SSc) is an immune-mediated rheumatic disease characterized by fibrosis of the skin and internal organs, along with vascular abnormalities. 1 It can be classified into limited and diffuse subsets, with the limited cutaneous SSc subset being more prevalent than the diffuse form. 2 Raynaud’s phenomenon typically manifests as the initial symptom and affects approximately 90% of patients with SSc, often followed by complications involving the skin, bones, joints, muscles, blood vessels, and internal organs. SSc is marked by altered T- and B-lymphocyte function, autoantibody production, and vascular damage, resulting in peripheral tissue hypoxia and extensive fibrosis. 3 Consequently, individuals with SSc may suffer progressive endothelial injury, marked by substantial collagen deposition in the skin and visceral organs, leading to organ dysfunction. 3 Patients with SSc exhibit heightened risks during surgical procedures due to vascular damage and soft tissue encapsulation defects. Conditions such as oral stenosis resulting from skin and vascular sclerosis, interstitial lung disease, and pulmonary hypertension further increase the risks associated with anesthesia. These factors also raise the likelihood of wound healing complications and enhance susceptibility to infections. 4 Adrenocortical adenoma is among the more prevalent types of adrenal tumors; nonfunctional adenomas and those producing mild hormones may remain asymptomatic. Nonfunctional and small adenomas generally do not necessitate additional treatment. However, unilateral adrenalectomy may be indicated in cases of functional adenomas causing clinically significant hormone overproduction. Surgical intervention is recommended for any indeterminate nodule larger than 4 cm on imaging. 5 This article presents a clinical case of a patient diagnosed with SSc and adrenocortical adenoma, offering insights into the management of such complex medical scenarios.
Case presentation
A 34-year-old male patient presented with generalized tan patches and hypopigmentation accompanied with skin hardening that lasted over a year. He was diagnosed with SSc in January 2024 following skin ulceration of the hand joints at another hospital and was subsequently admitted to our dermatology department. Computed tomography (CT) revealed a left adrenal gland measuring approximately 1.6 × 1.9 × 2.1 cm. He was prescribed topical creams (cumquat chloride ointment and dinex ointment) and received methylprednisolone (60 mg daily for 7 days). Upon discharge, the doctors at the previous hospital recommended further evaluation of the adrenal gland in a specialized facility, leading to his referral to our hospital. In late February 2024, he underwent a follow-up CT at the Yunnan Cancer Hospital, which revealed a slightly hypodense nodule in the outer branch of the left adrenal gland measuring approximately 2.2 cm × 1.7 cm. The nodule exhibited a clear boundary and uneven enhancement (Figure 1). CT diagnosis indicated a benign nodule in the outer branch of the left adrenal gland with the possibility of adenoma, suggesting additional assessment through clinical examinations and magnetic resonance imaging. The patient reported a 2-kg weight gain over the past month. He had a 15-year history of smoking and an 8-year history of alcohol consumption, and the patient is currently abstinent. No other abnormalities were observed in the patient.
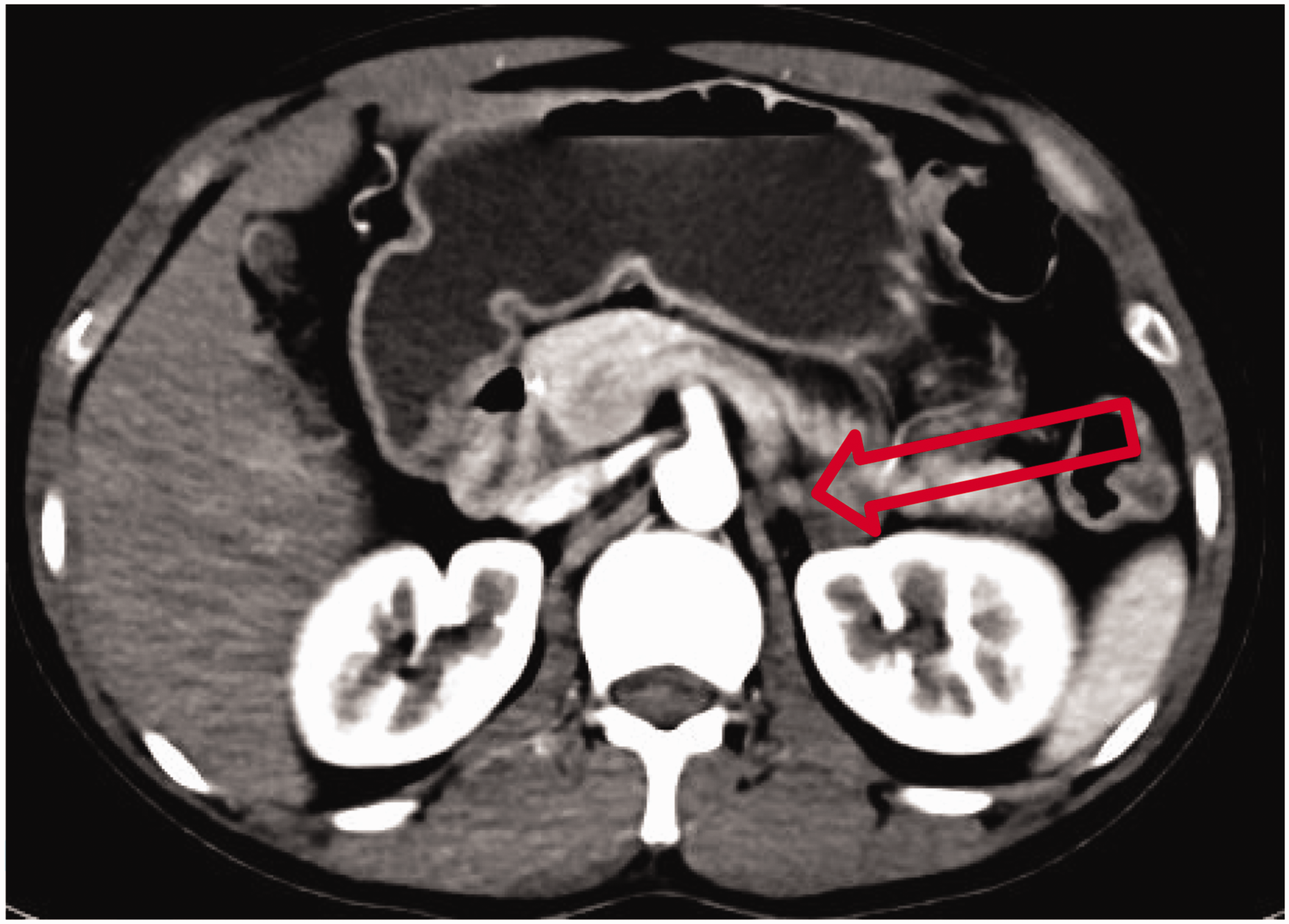
Preoperative computed tomography demonstrating a mildly hypodense nodule in the left lateral adrenal branch with heterogeneous enhancement (arrow indicates the lesion location).
Upon examination, the skin across the entire body appeared leathery and highly tense. The nasolabial folds on the face were shallow, resulting in stiff facial expression. The joints of both hands showed crust formation, with limited movement of the fingers resembling an “eagle’s claw” (Figure 2). There were patches of brownish plaques with hypopigmentation visible on the fingers and abdomen, whereas the remainder of the body showed no significant abnormalities. Laboratory tests revealed the following results: (a) C-reactive protein: 7.26 mg/mL (reference range: <6.0 mg/mL); (b) prothrombin activity: 150 (reference range: 70–120); (c) estradiol: 15.61 pg/mL (reference range: 21–62 pg/mL); (d) white blood cells: 17.86 × 109/L (reference range: 3.5–9.5 × 109/L); (e) anti-ribonucleoprotein (RNP) antibodies: positive (reference range: negative); (f) anti-nuclear antibody: positive (reference range: negative); and (g) anti-Scl-70 antibody assay: positive (reference range: negative). The preoperative blood pressure was within normal limits.

The skin exhibited severe sclerotic changes before surgery. The patient’s fingers were in a claw-like posture, preventing normal flexion and extension of all five fingers, even with external assistance (arrow indicates the patient’s hand).
The patient underwent transabdominal laparoscopic resection of the left adrenal tumor in March 2024 following a multidisciplinary consultation. Owing to the patient’s highly sclerotic skin and unclear radial artery pulsation, right femoral artery puncture tubing was used for pulse blood pressure monitoring during the operation (Figure 3). The blood pressure spiked to 280/120 mmHg during tumor separation. The procedure proceeded smoothly, with complete tumor resection, and no active intraoperative bleeding was observed. Postoperatively, the patient was transferred to the intensive care unit (ICU) for further evaluation and care. On the first postoperative day, the patient abruptly lost consciousness upon transitioning from the lying to sitting position. He exhibited signs of anemia, unstable circulation, cold extremities, and hemorrhagic drainage totaling approximately 350 mL. Further examination indicated an ongoing hemoglobin decline, suggesting active abdominal cavity bleeding. Emergency exploratory surgery revealed a bleeding volume of approximately 3500 mL from a ruptured small branch of the splenic artery. Suturing was challenging because of skin sclerosis (Figure 4(a)). Following surgery, the patient returned to the ICU for management, including rehydration, circulatory stabilization, and electrolyte balance maintenance. The postoperative incision showed mild redness, swelling, fluid and partial blood oozing, and delayed healing (Figure 4(b),(c),(d)). In severe cases, incisional dehiscence and hernia occurred, necessitating repeated partial suturing, placement of two subcutaneous drainage tubes, and intensified infection control measures. A postoperative pathological examination (Figure 5) confirmed adrenocortical adenoma involving the left adrenal gland. The specific stains showed VG: + AG: +.

During anesthesia, due to the patient’s extensive sclerotic skin and the lack of clear arterial vascular pulsation, routine procedures such as radial artery puncture were impracticable. Consequently, ultrasound-guided femoral artery puncture and cannulation were performed.

Incisions at various stages post-surgery; (a) Patient with highly sclerotic skin at the incision site, making suturing challenging and requiring intermittent use of silk sutures; (b) at 39 days post-second operation, some sutures were removed, with delayed removal in poorly healed areas; (c) at 41 days post-second operation, all sutures were removed, showing poorly healed incisions and (d) at 58 days post-second operation, incisions were healing slowly, with incomplete closure.

Postoperative pathological diagnosis of adrenocortical adenoma. (a) Image at 40× magnification and (b) image at 100× magnification.
He was hospitalized for 28 days, during which he received methylprednisolone sodium succinate, prednisolone tablets, antibiotic therapy, and various symptomatic supportive treatments. Upon discharge, his physical examination revealed leathery skin changes with slightly improved skin tension compared with that at admission. His facial nasolabial folds became shallower, but his facial expression remained stiff. Scabs were visible in the joints of both hands, with a partial limitation in finger movement, which significantly improved compared with that at admission (Figure 6). Flaky tan plaques and noticeable hypopigmentation were observed in the fingers and abdomen. Owing to slow healing of the postoperative incision, the patient was discharged with instructions for regular outpatient incision care and dressing changes for the fistula wound. Eventually, his incision fully healed 3 months postoperatively, and he continued to receive standardized treatment for SSc at an external hospital.

At 28 days post-operation, finger mobility and skin tension showed improvement compared with the preoperative condition (arrow indicates the patient’s hand).
Discussion
Adrenocortical adenoma is a tumor derived from adrenocortical cells, which can be hormonally inactive or can produce and release cortisol hormones, leading to either subclinical or overt clinical symptoms. 6 SSc primarily affects young and middle-aged women, often resulting in generalized skin thickening and internal organ lesions within 2 years. This disease substantially affects patients’ quality of life, with a 50% mortality rate over 3 years. 7 Laboratory tests typically reveal positive results for anti-ribosomal P protein antibodies, anti-nuclear antibodies, and anti-Scl-70 antibodies. The patient had previously been diagnosed with SSc at another hospital, and our CT findings and postoperative pathology confirmed the presence of adrenocortical adenoma.
This patient presented with an adrenocortical adenoma concomitant with SSc. Although preoperative blood pressure monitoring showed no obvious abnormalities, significant blood pressure fluctuations were observed during surgery, peaking at 280/120 mmHg during tumor isolation, suggesting that the adenoma was functional. Functional adrenocortical adenomas can secrete hormones such as cortisol. Initially, the patient showed no specific clinical symptoms, revealing that hormone secretion may have maintained homeostasis regulated by the hypothalamic–pituitary–adrenal (HPA) axis. SSc treatment typically involves long-term glucocorticoid therapy. However, excessive glucocorticoids can suppress the HPA axis via negative feedback, potentially disrupting homeostasis or promoting tumor malignancy. Hence, adrenal tumor resection was deemed necessary for managing SSc effectively. The decision for surgery was further supported by significant postoperative improvements observed in skin tension and finger mobility compared with the preoperative levels.
Vascular injury and dysfunction represent the early defining features of SSc, which is a progressive connective tissue disorder characterized by vascular abnormalities and widespread fibrosis affecting both skin and internal organs. 8 Owing to severe skin sclerosis, incision, suturing, and wound healing are exceptionally challenging for patients with SSc. Abnormal vascularization of the terminal vessels complicates postoperative wound healing, often necessitating multiple partial closures and increasing susceptibility to incisional herniation and wound infection. Following surgery, the patient diligently adhered to the dressing changes, resulting in a relatively prolonged but ultimately successful recovery period.
Owing to the extraperitoneal location of the adrenal gland, laparoscopic resection of adrenal tumors typically involves a retroperitoneal approach. However, due to the patient’s highly sclerotic skin, the planned retroperitoneal approach necessitated a 90° lateral position and elevation of the renal bridge, posing risks of muscle and skin damage. Consequently, the transabdominal approach was chosen. The surgery proceeded smoothly, and no active bleeding was observed upon thorough postoperative examination. Nevertheless, the patient exhibited shock symptoms on the first postoperative day, prompting the identification of a small branch rupture of the splenic artery, which led to subsequent surgical laparotomy. The patient presented with adrenocortical adenoma combined with SSc, posing higher anesthetic risks than typical adenoma cases. Therefore, continuous monitoring of ambulatory blood pressure and blood gases throughout the procedure is considered crucial. Although radial artery cannulation is routinely used for this purpose, the patient’s highly sclerotic skin obscured the radial artery pulsation. Consequently, ultrasound-guided puncture cannulation of the right femoral artery was performed for arterial blood pressure and blood gases monitoring during surgery. SSc involves dense inflammatory cell infiltration of the microvascular system and extensive collagen deposition. 9 Moreover, the patient had a history of long-term hormone therapy, which affects the heart and vasculature via glucocorticoid and mineralocorticoid receptors, as well as altering local glucocorticoid metabolism through 11β-hydroxysteroid dehydrogenase. These factors contribute to intravascular damage, affecting vascular function and predisposing patients to atherosclerosis and vascular remodeling. 10 Both SSc and glucocorticoid use alter normal vascular structure, thereby increasing bleeding risks during surgery and anesthesia, which can impact various organs and exacerbate postoperative bleeding risks.
Currently, various treatment methods are available for SSc, with both traditional Chinese medicine and Western medicine offering consistent approaches. Immunosuppressive agents are commonly used to effectively treat symptoms such as skin sclerosis caused by scleroderma and slow the progression of the disease. Various immunosuppressive agents, such as methotrexate, corticosteroids, and cyclophosphamide, are commonly used to treat fibrosis. Although drugs and approaches such as mycophenolate mofetil, intravenous immunoglobulin, B-cell-depleting agents, anti-interleukin 6 receptor antibodies, autologous hematopoietic stem cell transplantation, rapamycin, pirfenidone, and imatinib mesylate have potential, their efficacy in treating SSc has not yet been fully demonstrated. 11 Targeting transforming growth factor-1 and its signaling pathway or modulating the imbalance between T-helper cell 1 and 2 immune responses are also promising therapeutic options. SSc-associated interstitial lung disease (SSc-ILD) and SSc-associated pulmonary hypertension are the leading causes of SSc-related mortality, which can be managed with nidazanib and tolizumab. Autologous hematopoietic stem cell transplantation may be considered for refractory progressive SSc with ILD. 12 Chinese medicine also plays a significant role in SSc treatment, alleviating symptoms and reducing the need for glucocorticoids to minimize associated side effects. Institutional Chinese medicine treatments, such as tai chi, Gui Zhi Fu Ling pills, and Yi Qi and blood recipes, effectively address physical imbalances such as Yang deficiency, Qi deficiency, and blood stasis caused by SSc. 13 Tripterygium wilfordii or Paeonia lactiflora tip and black phosphorous–hydrogel base microneedles have shown promise in SSc treatment. 14
Conclusions
No curative therapies have been developed for SSc, and the risk of death remains high. SSc is typically diagnosed at advanced stages and is characterized by cutaneous fibrosis, significant organ involvement, and occlusive vascular lesions. However, early detection of the disease and initiation of treatment before the occurrence of irreversible visceral organ damage remain significant challenges for clinicians. 15 Due to autoimmune dysregulation and the necessity of chronic immunosuppressive therapy, patients experience severe functional impairments. Prolonged clinic visits further impact their physical and mental health, reducing their overall quality of life. 16 In cases involving concurrent adrenal tumors or other endocrine tumors, clinicians must make treatment decisions based on comprehensive assessments. Early disease-stage diagnosis, risk stratification of organ involvement, and timely pharmacological interventions are crucial to slowing disease progression, enhancing quality of life, and extending patient survival.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605251326822 - Supplemental material for Management of adrenocortical adenoma in systemic sclerosis: A case report
Supplemental material, sj-pdf-1-imr-10.1177_03000605251326822 for Management of adrenocortical adenoma in systemic sclerosis: A case report by Zongyan Luo, Yuanlong Shi, Jinye Yang, Yuanpeng Duan, Qiao Wang, Can Li, Sinan Yang, Bo Peng, Kun Zhang, Libo Yang, Bin Zhao and Chengwei Bi in Journal of International Medical Research
Supplemental Material
sj-pdf-2-imr-10.1177_03000605251326822 - Supplemental material for Management of adrenocortical adenoma in systemic sclerosis: A case report
Supplemental material, sj-pdf-2-imr-10.1177_03000605251326822 for Management of adrenocortical adenoma in systemic sclerosis: A case report by Zongyan Luo, Yuanlong Shi, Jinye Yang, Yuanpeng Duan, Qiao Wang, Can Li, Sinan Yang, Bo Peng, Kun Zhang, Libo Yang, Bin Zhao and Chengwei Bi in Journal of International Medical Research
Supplemental Material
sj-pdf-3-imr-10.1177_03000605251326822 - Supplemental material for Management of adrenocortical adenoma in systemic sclerosis: A case report
Supplemental material, sj-pdf-3-imr-10.1177_03000605251326822 for Management of adrenocortical adenoma in systemic sclerosis: A case report by Zongyan Luo, Yuanlong Shi, Jinye Yang, Yuanpeng Duan, Qiao Wang, Can Li, Sinan Yang, Bo Peng, Kun Zhang, Libo Yang, Bin Zhao and Chengwei Bi in Journal of International Medical Research
Footnotes
Acknowledgments
We are grateful to the patients who provided messages for this study.
Author contributions
ZL, YS, JY, and YD equally contributed to data collection and article writing. QW, CL, SY, BP, KZ, and LY contributed to article checking and literature formatting. BZ and CB provided full guidance and supervised article writing. All authors have read and approved the final manuscript.
Declaration of conflicting interests
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Data availability statement
The original data of the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding authors.
Informed consent statement
Informed consent was obtained from the patient.
Funding
This study was supported by grants from the Yunnan Provincial Science and Technology Department, Kunming Medical University Joint Special Fund for Applied Basic Research (202001AY070001-069), Scientific Research Fund of Yunnan Provincial Department of Education (2020J0207), Teaching Alliance Undergraduate Education Teaching Research Project of the Third Affiliated Hospital of Kunming Medical University in 2023 (JXYJ20230211), and Kunming Medical University 2024 Graduate Education Innovation Fund (2024S341 and 2024S342).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.