
Abstract
Background:
Single balloon enteroscopy (SBE) is an important tool in the management of small bowel disease with limited data available on its performance in the elderly. We aimed to evaluate the safety, efficacy, diagnostic and therapeutic outcomes of SBE in the elderly.
Methods:
A retrospective review was performed on 366 patients undergoing 428 SBEs from 2010 to 2014. Patients were divided into different age groups: control <55, 55–64, 65–74 and ⩾75 years. Data on comorbidities, complications, findings, diagnostic and therapeutic yield were compared between groups.
Results:
Anterograde and retrograde SBE were performed in 340 and 49 patients, respectively, with 63 patients requiring more than 1 procedure. Diagnostic yield was significantly higher for age ⩾75 years compared with <55, 66.3% versus 50%, odds ratio (OR) 1.97 [95% confidence interval (CI) 1.14–3.41]. Therapeutic yield was significantly higher in all three older age groups compared with <55 years, 20.3%: 55–64 years, 44.4%, OR 3.13(95% CI 1.7–5.78); 65–74 years, 42%, OR 2.84 (95% CI 1.59–5.06); and >75 years, 47.5%, OR 3.55 (95% CI 1.96–6.43). No significant difference was seen between age groups in complications or failures. Our overall complication rate was 2.3% with 5 minor and 5 major complications. There was a higher yield of angioectasias in the elderly. Argon plasma coagulation (APC) and multipolar electrocoagulation were used more often in older age groups.
Conclusion:
SBE is safe in elderly patients and delivers higher diagnostic and therapeutic yields compared to younger patients. The elderly are more likely to have angioectasias and undergo APC and electrocoagulation.
Introduction
Since its development in 2006 and commercial introduction in 2007, single balloon enteroscopy (SBE) has emerged as an important tool, allowing gastroenterologists to inspect previously unreachable areas of the small bowel [Mauro et al. 2012]. The introduction of video capsule endoscopy (VCE) significantly altered the landscape of small bowel imaging by providing visualization of small bowel disease; however, its use as a diagnostic tool is limited without therapeutic potential. Balloon-assisted enteroscopy addresses the limitations of VCE, becoming one of the newest methods for treatment of small bowel disease.
The focus of most studies on SBE is to evaluate the diagnostic and therapeutic potential compared with double balloon enteroscopy (DBE) [Frantz et al. 2012; Upchurch et al. 2010; Ramchandani et al. 2009; Riccioni et al. 2011; Kawamura et al. 2008; Domagk et al. 2011; Tsujikawa et al. 2008; May et al. 2010; Lenz and Donagk, 2012]. The most common indication for SBE is the diagnosis and treatment of obscure gastrointestinal bleeding (GIB). Obscure bleeding accounts for about 5–10% of GIB events, with majority arising from the small bowel [Mauro et al. 2012]. One study performed by Kushnir and colleagues found that more than 50% of patients experienced no recurrent GIB 2 years after SBE [Kushnir et al. 2013]. However, despite the utility of SBE, procedural complexity, complication risks and long procedure times are obstacles to incorporating it into daily practice. The average examination time for anterograde SBE approaches 1 hour and the retrograde approach is even more time consuming at an average of 68.8 minutes [Lenz and Domagk, 2012].
While SBE has been found to be a relatively safe procedure, complications may arise including bowel perforation, mucosal tears, bleeding, aspiration pneumonia, pancreatitis and postprocedural abdominal pain [Kawamura et al. 2008]. Between 2010 and 2050, the United States is projected to experience rapid growth in the older population. The baby boomers are largely responsible for this increase in the older population and began crossing over into this category in 2011, with a projected population increase of more than double in the upcoming years [Vincent and Velfoff, 2010]. With an aging population, an increased number of endoscopies are performed in older patients with multiple comorbidities, placing them at an increased risk for sedation-related complications. Previous studies have established the safety of upper endoscopy, colonoscopy, endoscopic retrograde cholangiopancreatography (ERCP) and, most recently, DBE in older patients [van Kouwen et al. 2003; Clarke et al. 2001; Katsinelos et al. 2006; Seinelä et al. 1998; Lukens et al. 2009; Hedge et al. 2010; Byeon et al. 2012]. However, there are no published data evaluating the safety and utility of SBE in the elderly. In this study, we aimed to evaluate the safety and efficacy of SBE with comparison of outcomes in three older patient populations with patients younger than the age of 55.
Materials and methods
Patients
Following approval from the University of South Florida and the Tampa General Hospital Institutional Review Boards, the Digestive Diseases and Nutrition Department at Tampa General Hospital established a database of SBE procedures by performing a retrospective chart review of 366 patients undergoing 428 SBE since 2010. Data collected for this database included demographics, comorbidities, history of overt/occult gastrointestinal (GI) bleeding, procedure findings, therapeutic intervention and complications. Chart reviews were performed only by physicians. Data were entered into a Microsoft® Access database by a data analyst and ambiguities in any data points were discussed, researched, reviewed and corrected. Patients were divided into four different age groups: control <55 years, 55–64 years, 65–74 years and ⩾75 years. We analyzed SBE results including comorbidities, SBE route, diagnostic yield, therapeutic intervention and complications between age groups. Minor complications were defined as failure to advance the enteroscope, mild to moderate bleeding and heart arrhythmias that resolved intraprocedurally not requiring intensive care unit (ICU) admission. Major complications were described as those causing bowel perforation or significant balloon trauma, extensive GI bleeding, unplanned and/or emergent intubation, and the admission to the ICU postprocedurally.
SBE procedure
SBE was performed using a high-resolution endoscope (SIF-Q180; Olympus Medical, Center Valley, Penn). The enteroscope has a working length of 200 cm, is 9.2 mm in diameter, and contains a working channel of 2.8 mm diameter. The disposable overtube (ST-SB1; Olympus Medical) is 140 cm long with a 13.2 mm outer diameter. It is equipped with a latex-free balloon at the tip, with air inflation and deflation from a pressure-controlled pump system.
Immediately prior to each procedure, an anesthesiologist obtained an independent clinical history and examined each patient. The decision to proceed with the scheduled SBE or cancel the case was based on the patient’s physical state as assessed by the gastroenterologist and anesthesiologist assigned to the case. SBE was performed by one of four experienced endoscopists.
All procedures were performed under monitored anesthesia care using intravenous propofol administered by anesthesiologists. The procedure time was defined as the time between the insertion of SBE and the complete withdrawal of SBE. Fluoroscopy was not used. Antiplatelet and anticoagulation therapies were held at least the night prior to the procedure with a required an International Normalized Ratio (INR) of 1.5 or less. An overnight fast was used to prepare for the anterograde approach, whereas bowel preparation with a polyethylene glycol solution was utilized in cases of retrograde SBE. The performance of endotracheal intubation was based on the assessment of anesthesia risk by the anesthesiologists and gastroenterologists. Vital signs, oxygen saturation and end tidal carbon dioxide (CO2) concentration were monitored by an anesthesiologist or nurse anesthetist during SBE and in patients requiring intubation; bispectral index (BIS) status was also monitored. After SBE, all patients were monitored in a recovery room and examined by a gastroenterologist prior to discharge from the unit to determine if early complications were present.
Statistical analysis
All statistical tests performed were two-sided and declared at the 5% significance level. The primary outcomes were diagnostic and therapeutic yields. T-test and logistic regression assessed association between dependent and independent variables. For continuous data, the results were summarized as mean difference (MD) and standard deviation (SD). For dichotomous data, the results were summarized as the odds ratio (OR) and 95% confidence intervals (CI). Statistical analyses were performed with SAS 9.3 software.
Results
Patient characteristics
Table 1 displays the demographic characteristics of patients undergoing SBE. A total of 366 patients undergoing 428 SBEs were evaluated. Anterograde and retrograde SBE were performed in 390 and 49 patients, respectively, with 11 patients undergoing both procedures. The route of SBE was determined according to the presumed location of the lesion based on medical history and the location of any potential bleeding sources on capsule endoscopy. A total of 63 patients within this group underwent multiple SBEs, with 37, 21, 4 and 1 patient undergoing 2, 3, 4 and 5 SBEs, respectively. Older patients were more likely to undergo anterograde SBE while our younger group was more likely to undergo a retrograde approach (Table 1). A total of 16 SBE procedures were performed on patients hospitalized in the ICU, 152 SBE procedures were performed as general floor/inpatient, and 260 SBE procedures were outpatient.
Demographic characteristics of patients undergoing single balloon enteroscopy.

ASA, American Society of Anesthesiologists; CI, confidence interval; OR, odds ratio; RBC, red blood cell; SBE, single balloon enteroscopy.
The mean age of patients undergoing SBE was 63 ± 15.5 years (range 19–98 years). In Group 1, there were 101 patients ⩾75 years, Group 2 had 119 patients between the ages of 65 and 74 years, Group 3 had 90 patients between 55 and 64 years of age, and Group 4 had 118 patients 55 years of age or younger. There was a higher percentage of males in Groups 2 and 4 (p = 0.02, p = 0.002, respectively) (Table 1). There was no significant difference in the proportion of whites, blacks or other races across age groups. There was also no significant difference regarding history of abdominal surgeries or hospitalizations across age groups. Group 2 received significantly more transfusions than the other age groups (p = 0.042) (Table 1).
The American Society of Anesthesiologists (ASA) physical classification system was also observed across groups. The majority of our patients across all age groups were classified as ASA class III, ranging from 66.4% to 69.3% in comparison with our control group at 72%.
The Charlson Co-Morbidity Index (CCI) was used as a measure to evaluate comorbidities across age groups. With increasing age, there was a progressive increase in the CCI with all older age groups reaching statistical significance compared with the younger Group 1 (Table 1).
When evaluating the use of medications, there were also significant differences. Aspirin use was more common in Group 2, 22.2% (p < 0.0001), Group 3, 34.5% (p < 0.0001) and Group 4, 32.7% (p < 0.0001) compared with 4.2% in the control group younger than age 55 (Table 1). Anticoagulant use was more common in the older groups compared with to the control group 5.1%: Group 2, 16.7% (p = 0.011); Group 3, 14.7% (p = 0.025); Group 4, 14.9% (p = 0.02) (Table 1). The use of nonsteroidal anti-inflammatory drugs (NSAIDs) was not significantly different in the various age groups (Table 1).
Safety of SBE
There were very few complications associated with SBE. Across age groups, there was no statistically significant association of age with complications. Minor complications occurred in 0 patients in Group 3 (Table 2). There were 3 patients in the Group 1 and 1 patient each in Groups 2 and 4 who experienced minor complications with rates of 2.5%, 1.1% and 1%, respectively (Table 2). These events included bradycardia, supraventricular tachycardia and mild bleeding. Major complications occurred in a total of five patients across all groups. There were no major events in our control group, with a rate of 1.1%, 2.5% and 2% in Groups 2, 3, and 4, respectively (Table 2). Major complications included hemodynamic instability after extubation requiring admission to the ICU, bowel perforation and balloon trauma. One bowel perforation occurred in the duodenum, with the SBE procedure being difficult because of tortuosity of the area. There were no deaths related to SBE observed during this study period.
Complication data in single balloon enteroscopy.
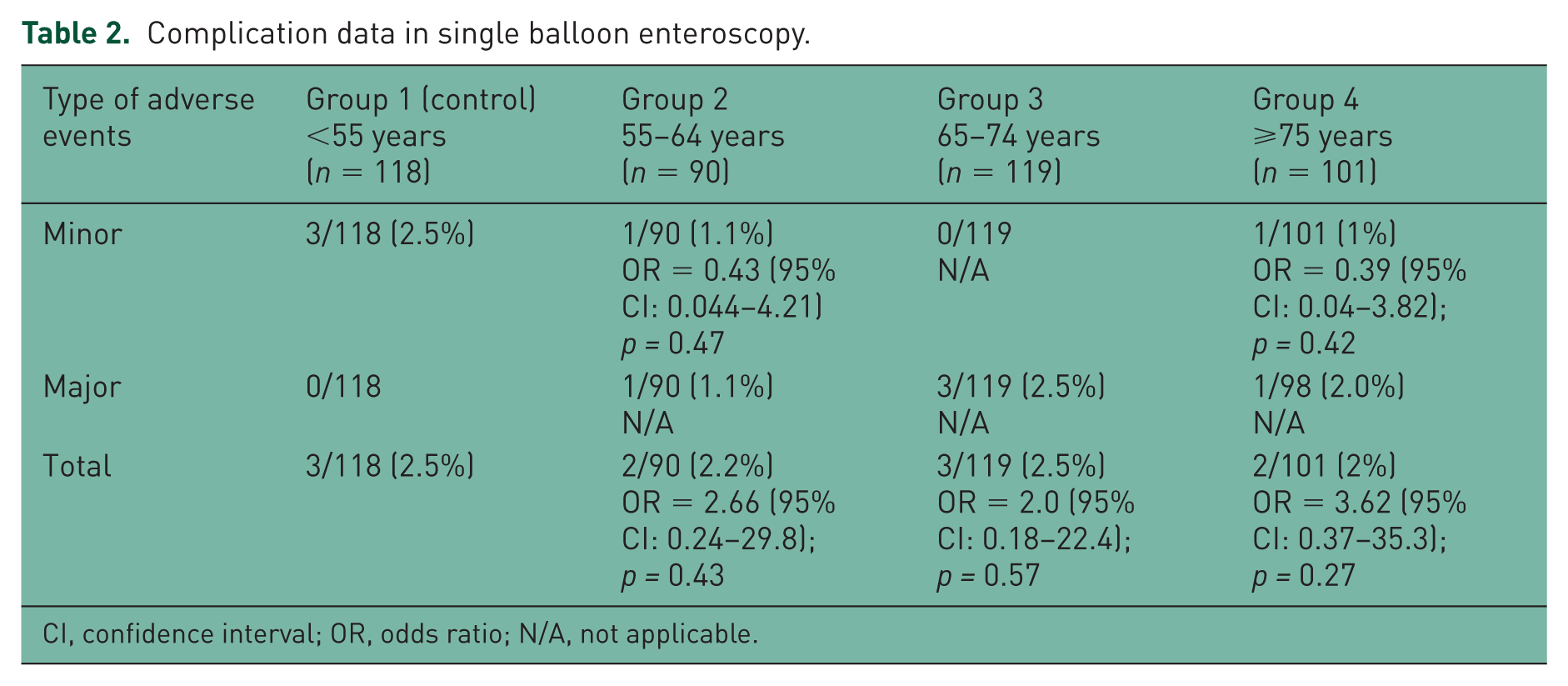
CI, confidence interval; OR, odds ratio; N/A, not applicable.
Indications for SBE
The most common indication for SBE was obscure GIB (Table 3). Obscure GIB was defined as occult or overt bleeding of unknown origin that persisted or recurred after an initial negative endoscopic evaluation including esophagogastroduodenoscopy (EGD) and colonoscopy. In 353 of our 428 patients, SBE (82.5%) was performed for suspected obscure GIB and the majority of the patients were older than age 55 years old with 90%, 90.8% and 94.1% of patients in Groups 2, 3 and 4, respectively, having obscure GIB (Table 3). Of these, about half (n = 178) were for overt GIB as defined as bleeding with visible blood loss manifested as melena or hematochezia, and 180 were performed for occult GIB defined as no visible blood loss; 28 % of patients in the control group with overt GI bleeding had positive endoscopic finding. In Groups 3 and 4, patients with overt GIB had a significantly higher rate of endoscopic findings with 48.7% in Group 3 (p = 0.001) and 46.5% in Group 4 (p = 0.005) (Table 3). In the occult GIB group, a significantly higher percentage of endoscopic findings were demonstrated in Groups 2, 3 and 4 compared with the control at 30.5% with 51.1% in Group 2 (p = 0.003), 42% in Group 3 (p = 0.003) and 47.5% in Group 4 (p = 0.01) (Table 3).
Indications for single balloon enteroscopy.
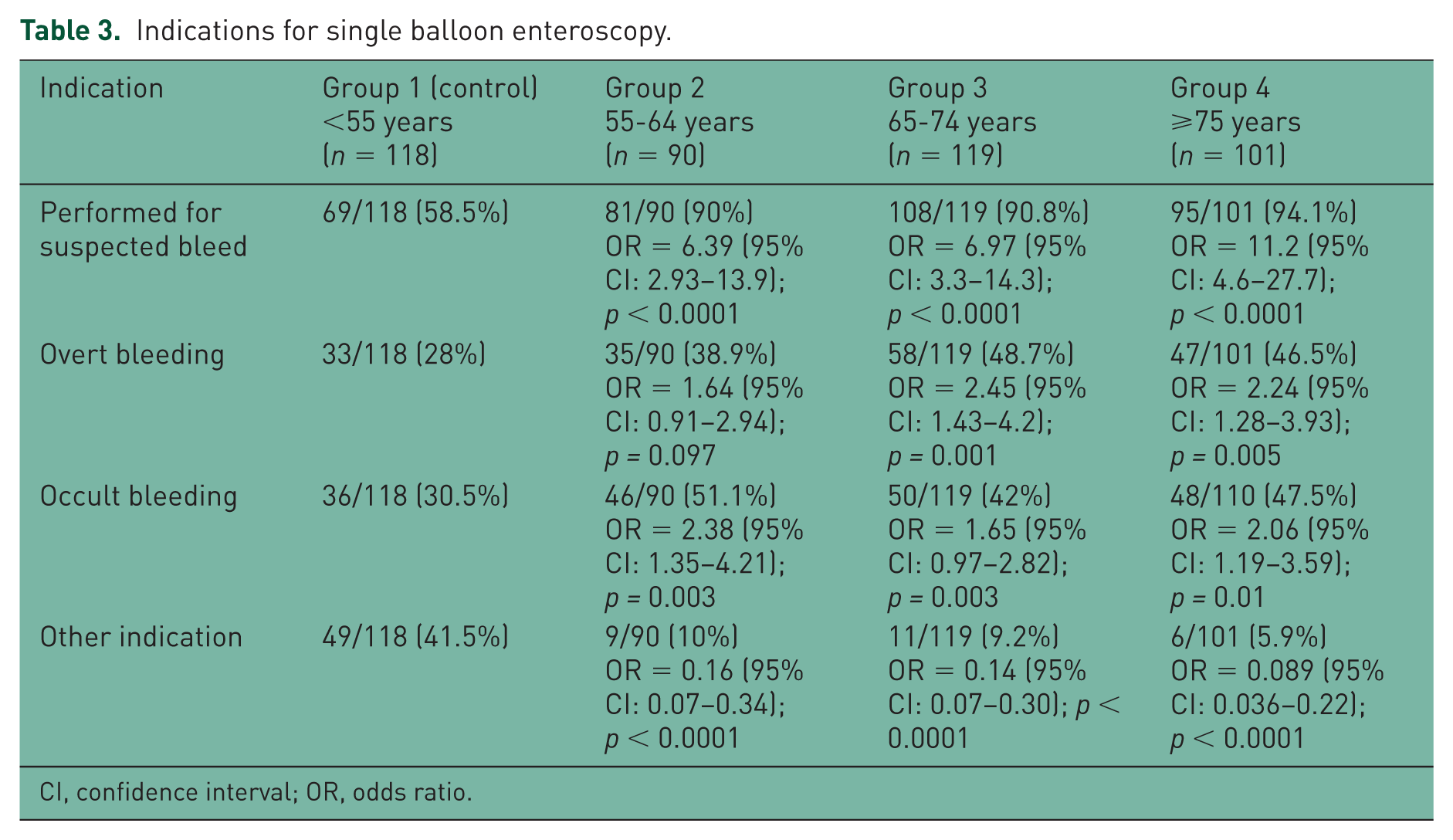
CI, confidence interval; OR, odds ratio.
Other indications such as abdominal pain, indeterminate colitis, abnormal imaging or evaluation for malignancy made up 17.5% of our patients, which included 41.5% in patients younger than 55 years and a progressive decrease with older age: Group 2 10% (p < 0.0001), Group 3 9.2% (p < 0.0001), Group 4 5.9% (p < 0.0001) (Table 3).
SBE findings and therapy
Our diagnostic and therapeutic yields in SBE are displayed in Table 4. When examining the site of diagnostic findings in the small bowel, the jejunum by far had the most findings, with the duodenum being second and the ileum last (Table 4). The jejunum was also the only area where findings differed significantly by age group. In comparison with our control group with a 14.4% rate of positive jejunal findings, there were an increasing number of findings in the jejunum with increasing age including 28.9% in Group 2 (p = 0.012), 32.8% in Group 3 (p = 0.001) and 33.7% in Group 4 (p = 0.001) (Table 4).
Diagnostic and therapeutic yields in single balloon enteroscopy.

CI, confidence interval; N/A, not applicable; OR, odds ratio; SBE, single balloon enteroscopy; VCE, video capsule endoscopy.
Angioectasias were the most common finding across all age groups (Table 4). The percentage of angioectasias found progressively increased with age from 13.6% in our control group to 30%, 37% and 39.6% in Groups 2, 3, and 4, respectively (p = 0.005, p <0.0001, p < 0.0001, respectively) (Table 4). Polyps and then small bowel ulcerations/erosions were the second and third most common finding among patients (Table 4). Strictures, atrophic villi, dieulafoy lesions and varices were less common findings (Table 4).
Argon plasma coagulation (APC) and multipolar electrocoagulation (Gold Probe®) were the most common methods of endoscopic therapy and were used significantly more often in the older age groups compared with the control group [APC: Group 1, 6.8%; Group 2, 21.1% (p = 0.004); Group 3, 19.3% (p = 0.006); Group 4, 17.8% (p = 0.015) and multipolar electrocoagulation: Group 1, 6.8%; Group 2, 15.6%, (p = 0.047); Group 3, 18.5% (p = 0.009); Group 4, 23.8% (p = 0.001)] (Table 4). Endoscopic therapy such as clips, dilation, polypectomy and dual therapy were less commonly used methods (Table 4).
Concordance between SBE and VCE
The concordance between SBE and VCE was also evaluated in our study. A total of 247 patients underwent VCE prior to SBE. Concordance was achieved when a VCE finding corresponded to the primary diagnostic finding in SBE in etiology and location. This occurred more often in our younger patient population of less than 55 years old (52.3%), with our overall concordance being 23.6%. However, there was no statistically significant difference in concordance among our younger and older age groups between SBE and VCE (Table 4).
Diagnostic and therapeutic success of SBE
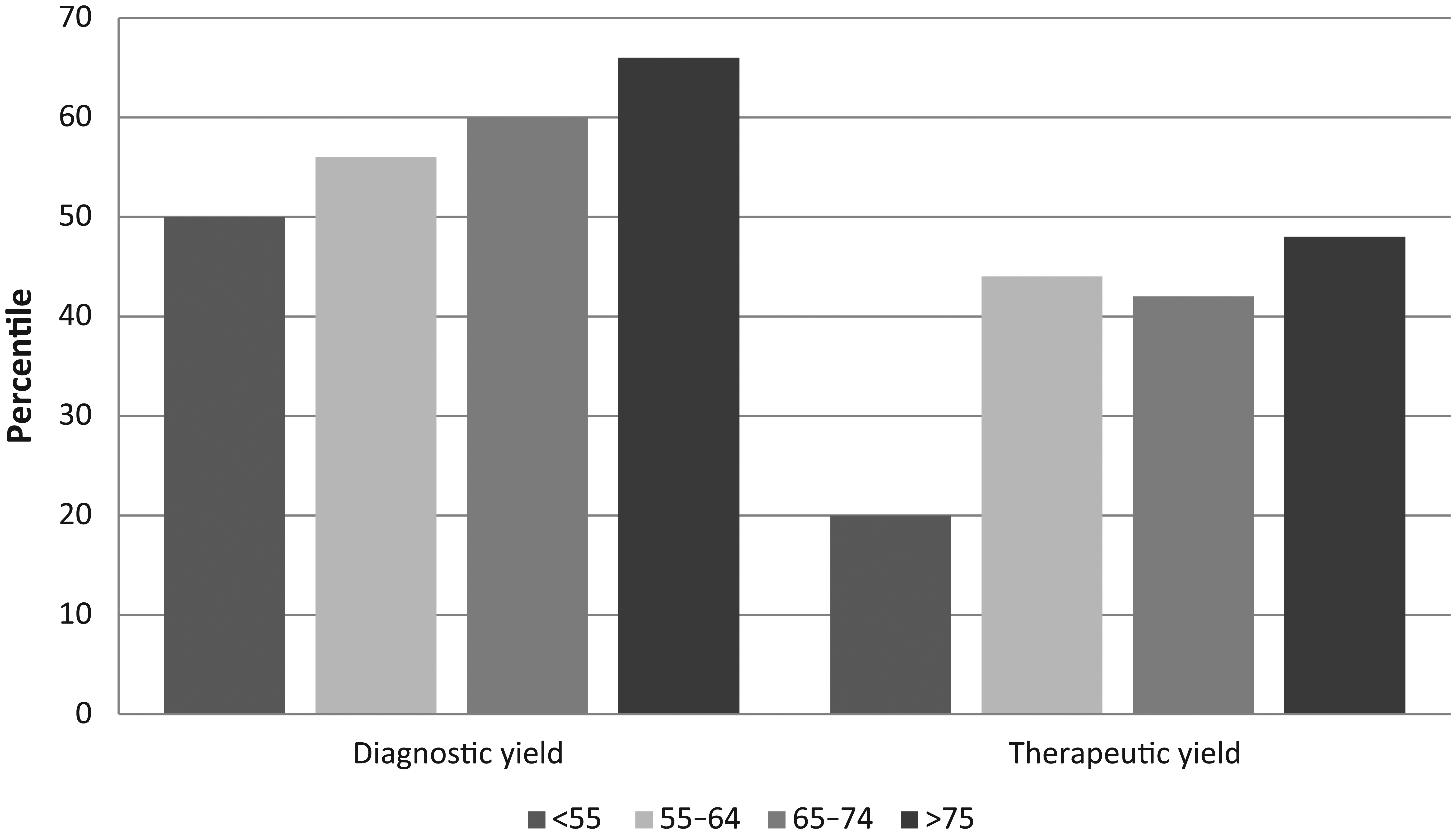
Table 4 and Figure 1 show data on the diagnostic and therapeutic yields of SBE. The diagnostic yield was significantly higher for the elderly ⩾75 years compared with <55 years, 66.3% versus 50%, respectively; OR 1.97 (95% CI 1.14–3.41; p = 0.015) (Table 4). Endoscopic therapy was used significantly more often in all 3 older age groups compared with our Group 1 patients, 20.3%: Group 2 44.4%, OR 3.13 (95% CI 1.7, 5.78; p < 0.0001); Group 3 42%, OR 2.84 (95% CI 1.59,5.06; p < 0.0001); and Group 4 47.5%, OR 3.55 (95% CI 1.96,6.43; p < 0.0001) (Table 4).
Diagnostic and therapeutic yields in single balloon enteroscopy.
Discussion
Endoscopic evaluation of the small bowel has traditionally been challenging for gastroenterologists. The advent of VCE helped resolve this diagnostic challenge by allowing complete visualization of the small bowel, yet does not offer a therapeutic option. Balloon-assisted enteroscopy has since filled this void as an important diagnostic and therapeutic tool in the management of small bowel disease. Among this group, SBE is the newest method, with limited data on the utilization and outcomes of this endoscopic modality. This is the first study to our knowledge evaluating the efficacy and safety of SBE in the elderly.
We demonstrated that SBE can be performed with adequate safety in older patient populations. Our complication rate was minimal with rates of 1% for minor adverse events and 1% to 2.5% for major adverse events in the elderly with only 1 perforation occurring in 428 SBEs. Aktas and colleagues evaluated the complications of SBE in 166 SBE procedures in 105 patients and also reported a low incidence of complications [Aktas et al. 2010]. No complications were reported in the 145 diagnostic procedures and only 1 perforation occurred in the 21 therapeutic SBE procedures during dilation of a stricture [Aktas et al. 2010]. Other studies have confirmed these findings with only 1 perforation (0.24%) out of a total of 412 SBE procedures [Manno et al. 2010]. These findings are comparable with complication rates of DBE ranging from 0.9% to 3.7% in the elderly, 0.8% in diagnostic DBE and 3.4–4.3% in therapeutic DBE in the overall population [Hedge et al. 2010; Byeon et al. 2012; Mensink et al. 2007; May et al. 2007]. Our study also performed a comparative analysis of the safety of SBE in younger patients compared with older individuals and showed no significant statistical difference despite the fact elderly patients are more likely to have significant comorbidities. Overall, we feel that SBE can be performed safely in the elderly; however, appropriate clinical judgment should always be utilized when selecting patients based on comorbidities and overall health when undergoing anesthesia for long endoscopic procedures
Our data demonstrate a higher diagnostic and therapeutic yield in the elderly. Our diagnostic yield in the elderly was higher compared with previous studies for SBE at 66.3% and reached statistical significance in comparison with the control group at 55.6%. Previous studies performed on SBE in all age groups report diagnostic yields ranging from 40.7% to 60% [Frantz et al. 2010; Upchurch et al. 2010; Ramchandani et al. 2009; Kawamura et al. 2008; May et al. 2010; Parikh et al. 2013]. Our higher diagnostic yield in the elderly patients is most likely due to the higher number of vascular lesions present in the elderly in comparison with the total population. We also found a significantly higher therapeutic yield in the elderly in comparison with younger patient populations. These results further support the use of SBE in the elderly given the higher therapeutic potential in this age group. All three older groups had higher therapeutic yields compared with our control group. This is consistent with other studies reporting therapeutic yields of 42–48% in the general population for SBE and is also comparable with a reported therapeutic yield of 46.8% for DBE in the elderly [Frantz et al. 2010; Upchurch et al. 2010; May et al. 2010; Hedge et al. 2010].
Angioectasias were the most common finding on SBE, which is consistent with previous reports on SBE in the general population [Frantz et al. 2010; Upchurch et al. 2010; Ramchandani et al. 2009; Riccioni et al. 2011; May et al. 2010; Sethi et al. 2014; Parikh et al. 2013]. Angioectasias are also more common in the elderly comparable with the data with DBE [Hedge et al. 2010; Byeon et al. 2012]. With increasing age, there was a progressively higher number of angioectasias with 13.6% in <55 years, 30% in 55–64 years, 37% in 55–74 years and 39.6% in ⩾75 years. The elderly were also more likely to undergo endoscopic therapy, which is likely related to the higher rate of angioectasias seen in this population. APC and multipolar electrocoagulation (Gold Probe®) were the most common therapeutic interventions. These two therapeutic interventions were performed more often with combined rates of 13.6% for both APC and multipolar electrocoagulation (Gold Probe®) in our younger control group and reached statistical significance with combined rates of 36.7%, 37.8% and 41.6% for 55–64 years, 65–74 years and ⩾75 years, respectively.
When evaluating diagnostic yield in the small bowel, the jejunum was the most common site of positive findings in all three older age groups. This is consistent with data from Bollinger and colleagues demonstrating that angioectasias occurred most commonly in the jejunum in Western society, with an incidence of 80% in this location [Bollinger et al. 2012]. In general, elderly patients are more likely to present with angioectasias, experience more lesions in the jejunum, and require more endoscopic therapy supporting the use of SBE in the elderly. Obscure GIB was the most common indication for SBE in the elderly population. Higher diagnostic yields were found for overt and occult GIB when the age group over the age of 65 was compared to the younger population. Our younger population was more likely to undergo SBE for evaluation of non-GIB lesions. These data are not surprising given that the elderly are more likely to have vascular lesions than younger patients as reported previously in the literature [Sharma and Gorbien, 1995; Zhang et al. 2012; Meyer et al. 1981].
The comparative diagnostic yield of VCE and SBE is also one area of interest with many comparative studies available. We found there was no statistical significant difference in concordance among our younger and older age groups between SBE and VCE, and an overall low concordance with VCE of 23.6%. One potential reason for these findings is a significant number of VCEs were performed at outside institutions and the level of expertise of the outside providers is unknown. These findings are consistent with those found in the elderly undergoing DBE [Hedge et al. 2010]. Some research has focused on the utility of prior small bowel evaluation by VCE, revealing a significantly higher diagnostic yield in SBE when it was preceded by a positive VCE [Sethi et al. 2014; Parikh et al. 2013]. VCE appears to be an ideal initial tool for the diagnosis of small bowel disease and should be considered complementary to SBE providing guidance regarding the best route for SBE (antegrade versus retrograde), and identifying the presence, nature and approximate location of lesions. Hedge and colleagues hypothesized that the low concordance rates between VCE and enteroscopy may be related to the inconsistency associated with the discontinuation of antiplatelet and anticoagulant medications prior to enteroscopy, but not for VCE [Hedge et al. 2010]. These medications may promote mucosal abnormalities such as angioectasias, which resolve or become less apparent on cessation of these medications. It appears that further investigation of this hypothesis is warranted.
While there were many significant findings in our study, we also recognize there are some potential limitations. Our study has the same limitations that any retrospective, single institution study may have, and our study is also lacking in long-term outcome data. Many of the patients in this study had their VCE performed at another institution before being referred for enteroscopy, which may have led to a lowering of the concordance rates between VCE and SBE. Finally, the number of patients excluded from undergoing SBE is unknown.
Conclusion
In summary, SBE is a safe and effective procedure in the elderly and can be of great diagnostic and therapeutic value. We found a minimal complication rate that was not significantly different in comparison with a younger patient population. Because the elderly are more likely to have higher diagnostic and therapeutic yields than a younger patient population, our data support the use of balloon-assisted enteroscopy, including SBE, in the management of obscure GIB in this age group.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The authors declare no conflicts of interest in preparing this article.