
Abstract
Objectives:
Caffeine consumption is reported to be associated with reduced hepatic fibrosis in patients with chronic liver diseases. We performed a systematic review and meta-analysis to assess the association between caffeine consumption and prevalence or hepatic fibrosis of nonalcoholic fatty liver disease (NAFLD) in observational studies.
Methods:
We searched the literature of all languages from PubMed, EMBASE, and the Cochrane library from 1 January 1980 through 10 January 2015. Total caffeine consumption was defined as the daily intake of caffeine (mg/day) from all caffeine-containing products. Combined and subgroup analyses stratified by study designs, study locations, and type of caffeine intake were performed.
Results:
Four cross-sectional and two case control studies with a total of 20,064 subjects were included in the meta-analysis. Among these, three studies with 18,990 subjects were included in the analysis for prevalence of NAFLD while the other three studies with 1074 subjects were for hepatic fibrosis. Total caffeine consumption (mg/day) was not significantly associated with either the prevalence [pooled mean difference (MD) 2.36; 95% confidence interval (CI) −35.92 to 40.64] or hepatic fibrosis (higher versus lower stages; pooled MD −39.95; 95% CI −132.72 to 52.82) of NAFLD. Subgroup analyses stratified by study designs and locations were also not significant. However, after stratifying by type of caffeine intake, regular coffee caffeine intake (mg/day) was significantly associated with reduced hepatic fibrosis of NAFLD (pooled MD −91.35; 95% CI −139.42 to −43.27; n = 2 studies).
Conclusion:
Although total caffeine intake is not associated with the prevalence or hepatic fibrosis of NAFLD, regular coffee caffeine consumption may significantly reduce hepatic fibrosis in patients with NAFLD.
Introduction
Caffeine consumption has significantly increased over the last several decades. Coffee continues to be the major source of caffeine, followed by soft drinks and tea for the average consumer in the United States [Frary et al. 2005]. Current estimates suggest 85% of the US population consume at least one caffeinated beverage daily, mainly sought out for its properties to improve mental alertness, concentration, and fatigue [Mitchell et al. 2014; Heckman et al. 2010]. Coffee consumption has been associated with a decrease in all-cause mortality, and multiple studies have highlighted the beneficial effects for several medical conditions including diabetes mellitus type II, Parkinson’s disease, hepatitis C virus, hepatocellular carcinoma (HCC), and nonalcoholic fatty liver disease (NAFLD) [Mitchell et al. 2014; Bambha et al. 2014; Freedman et al. 2012; Ruhl and Everhart, 2005; Molloy et al. 2012; Anty et al. 2012; Birerdinc et al. 2012; Catalano et al. 2010; Gutierrez-Grobe et al. 2012; Paynter et al. 2006; Bravi et al. 2007; Wilson et al. 2011; Liu et al. 2012].
As the most common cause of chronic liver disease, NAFLD most notably denotes an accumulation of fat within the liver; however this includes a wide spectrum of pathologic cellular injury including inflammation, hepatic fibrosis, cirrhosis, and HCC [Chen et al. 2014]. NAFLD is thought to be a hepatic manifestation of metabolic disorders such as hypertension, dyslipidemia, obesity, and impaired glucose tolerance, which likely contribute to its rapidly escalating prevalence [Chen et al. 2014; Shen et al. 2014].
Caffeine consumption is reported to be associated with reduced hepatic fibrosis in patients with chronic liver disease [Modi et al. 2010]. Multiple studies have since found similar findings but have been unable to clearly differentiate if the effect is from the coffee or caffeine and how these changes influence hepatic fibrosis of NAFLD, which is thought to be a manifestation of metabolic syndrome [Marchesini et al. 2001]. Therefore, to provide a synthesis of all evidence, we performed a systematic review and meta-analysis to evaluate the association between caffeine consumption and prevalence or hepatic fibrosis of NAFLD.
Methods
Literature search and inclusion criteria
We searched the literatures of all languages from PubMed, EMBASE, and the Cochrane library from 1 January 1980 through 10 January 2015, using the search terms (‘NAFLD’ or ‘nonalcoholic fatty liver disease’ or ‘NASH’ or ‘nonalcoholic steatohepatitis’ or ‘fatty liver’ AND ‘caffeine’ or ‘coffee’). Publications that met the following criteria: (I) observational studies with a comparison (retrospective or prospective cohort or case-control studies); (II) all study participants were over the age of 18; (III) the reported amount of caffeine consumption can be transformed to milligrams per day; (IV) NAFLD patients were diagnosed by elevated liver enzymes, abdominal ultrasound and/or liver biopsy, were included in the systematic review and meta-analysis. Bibliographies of the studies that met these criteria were also searched for potential applicable studies.
Data extraction and quality assessment
Two reviewers independently extracted the following data: first author, publication year, study population’s country of origin, study design, sample size, and findings. The Newcastle–Ottawa Scale (NOS) was utilized to assess the methodological quality of included studies independently by each reviewer. Methodological quality assessment using the NOS is based on selection of study groups, comparability of study groups, and the ascertainment of the exposure/outcome of interest. Any discrepancies regarding the inclusion/exclusion of studies or data extraction were determined by consensus of the reviewers.
Statistical analysis
To assess the association, summary data from individual studies were pooled using a random effect model. All continuous data are summarized as mean difference (MD) along with 95% confidence intervals (CIs). The inconsistency index (I2) was used to measure heterogeneity, with values of I2 > 50% indicating substantial heterogeneity [Higgins et al. 2003]. We planned for but did not assess for publication bias as we found less than 10 studies. All analyses were performed using Review Manager 5.2 with a p value <0.05 considered statistically significant. MOOSE guidelines were followed during the completion and reporting of this meta-analysis [Stroup et al. 2000].
Results
Characteristics of the studies
We initially identified a total of 118 studies that met our search criteria. After title and abstract review, 111 studies were excluded, which resulted in seven studies that underwent full-text review. Finally, six (four cross-sectional and two case control) studies were included in the meta-analysis (Figure 1) [Bambha et al. 2014; Molloy et al. 2012; Anty et al. 2012; Birerdinc et al. 2012; Catalano et al. 2010; Gutierrez-Grobe et al. 2012].
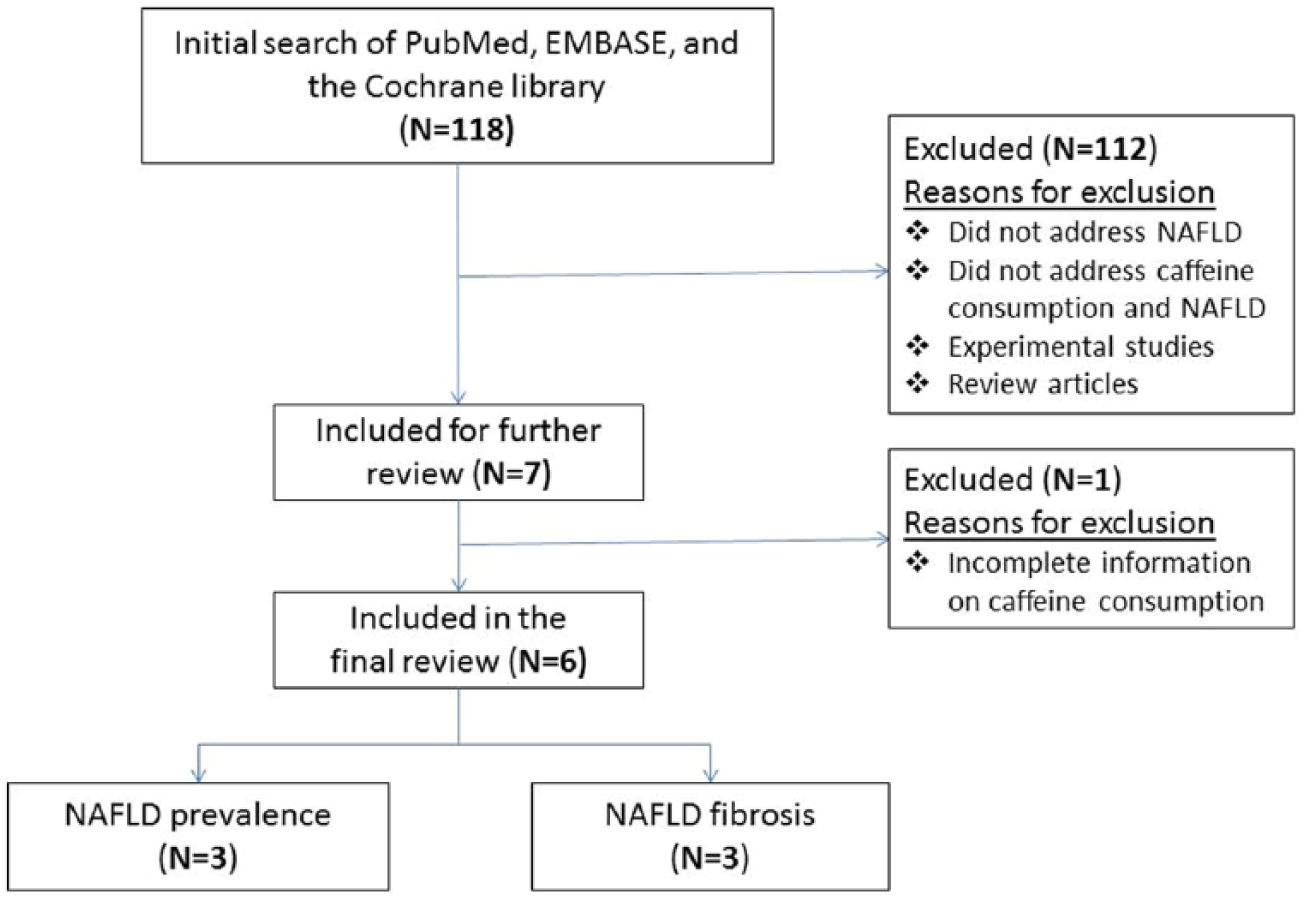
Study flow diagram.
Characteristics of the studies included in this meta-analysis are described in Table 1 and demographic characteristics of the cohorts analyzed are described in Table 2. Four cross-sectional and two case-control studies generated a total study population of 20,064 subjects. Among these, three studies with 18,990 subjects were included in the analysis for prevalence of NAFLD while the other three studies with 1074 subjects were used for the analysis of hepatic fibrosis. Measurement of caffeine intake by each study is included in Table 3. All of the included studies were thought to be of medium to high quality based on their NOS score.
Characteristics of studies included in meta-analysis.
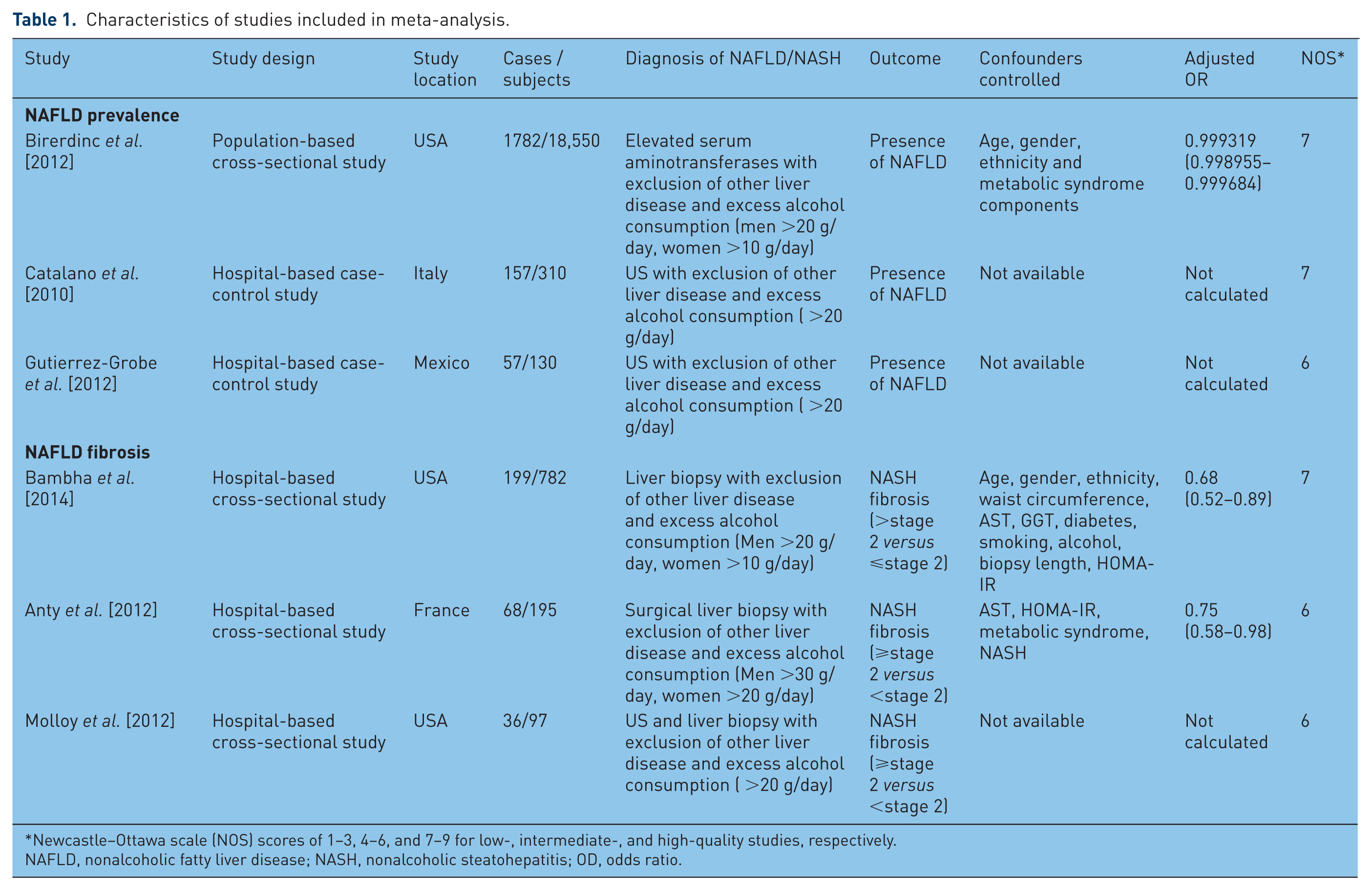
Newcastle–Ottawa scale (NOS) scores of 1–3, 4–6, and 7–9 for low-, intermediate-, and high-quality studies, respectively.
NAFLD, nonalcoholic fatty liver disease; NASH, nonalcoholic steatohepatitis; OD, odds ratio.
Demographic characteristics of the cohorts analyzed for each study included in meta-analysis.

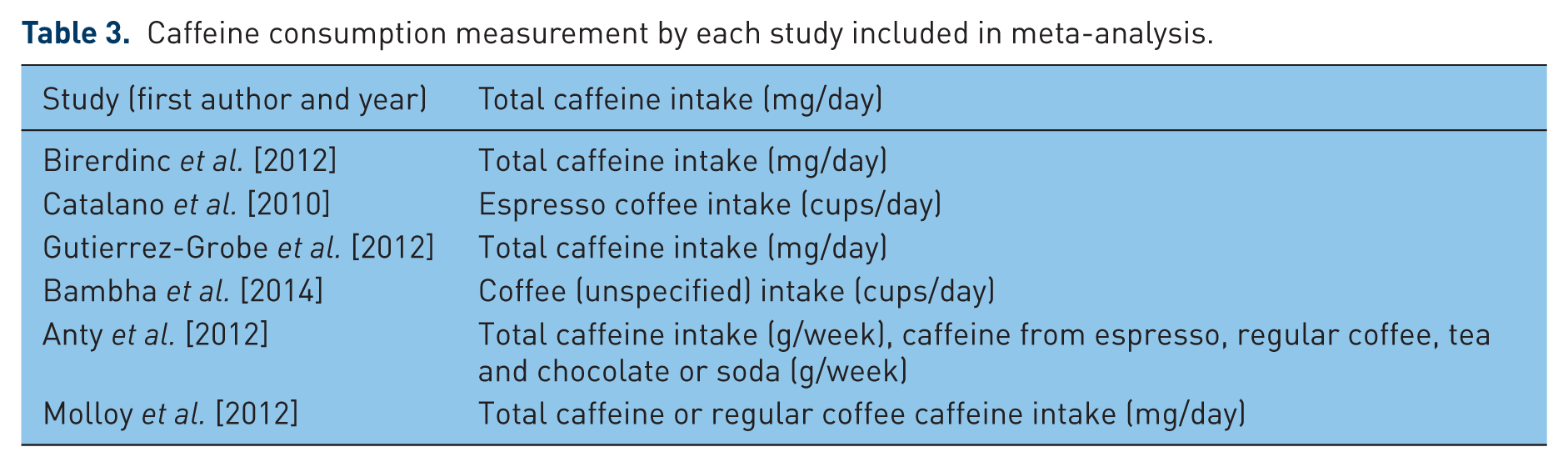
Caffeine consumption measurement by each study included in meta-analysis.
Outcome results
Total caffeine consumption (mg/day) was not significantly associated with either the prevalence [pooled mean difference (MD) 2.36; 95% confidence interval (CI) –35.92 to 40.64] (Figure 2) or hepatic fibrosis (pooled MD −39.95; 95% CI −132.72 to 52.82) of NAFLD (Figure 3). Further subgroup analyses stratified by study designs and locations were also not significant.

Forest plot: association between caffeine consumption and prevalence of nonalcoholic fatty liver disease (NAFLD).

Forest plot: association between caffeine consumption and hepatic fibrosis (advanced versus early stage) of nonalcoholic fatty liver disease (NAFLD).
Subgroups were then stratified again by type of caffeine intake (Table 4). Regular coffee as the source of caffeine intake was significantly associated with reduced hepatic fibrosis of NAFLD (pooled MD −91.35; 95% CI −139.42 to −43.27; n = 2 studies) (Figure 4). However, regular coffee caffeine intake was not associated with prevalence of NAFLD (pooled MD 23.06; 95% CI −8.67 to 54.80; n = 2 studies).
Subgroup analyses stratified by study designs, study locations, types of caffeine consumption.

NAFLD, nonalcoholic fatty liver disease; MD, mean difference.

Forest plot: association between regular coffee consumption and hepatic fibrosis (advanced versus early stage) of NAFLD.
Discussion
Previous studies have suggested that caffeine consumption plays a protective role in NAFLD [Bambha et al. 2014; Molloy et al. 2012; Anty et al. 2012; Birerdinc et al. 2012; Catalano et al. 2010; Gutierrez-Grobe et al. 2012; Modi et al. 2010]. To the best of the authors’ knowledge this is the first meta-analysis to investigate this relationship among caffeine consumption and the prevalence or degree of hepatic fibrosis of NAFLD.
The exact role caffeine plays in the prevalence and progression of NAFLD remains unknown. Caffeine has been implicated to have many antifibrotic effects through a series of biochemical processes including stimulation of hepatic stellate cell apoptosis, induction of intracellular F-actin and cAMP expression, inhibition of focal adhesion kinase and actin synthesis, along with inhibition of alpha-smooth muscle actin and procollagen expression [Shim et al. 2013]. The difficulty has been trying to tease out the role specific sources such as regular coffee, energy drinks, espresso, tea, etc. may influence these antifibrotic effects.
While this study did not find any significant association between total caffeine consumption and the prevalence or hepatic fibrosis of NAFLD, regular coffee caffeine intake was significantly associated with reduced hepatic fibrosis of NAFLD. Regular coffee consumption was defined as the ingestion of caffeine only from regular coffee, not including other caffeinated beverages such as espresso, tea, soda, etc. The beneficial effect of regular coffee on the liver to reduce liver enzymes (GGT, ALT) has recently been suggested by multiple studies [Molloy et al. 2012; Birerdinc et al. 2012; Cadden et al. 2007]. As a complex mixture of over one hundred compounds, coffee is considered to be derived of three main compounds: caffeine, chlorogenic acids, and diterpenes (cafestol and kahweol) [Gressner, 2009]. While caffeine modifies signaling pathways leading to the decreased activity of connective tissue growth factor (CTGF), considered to be a major stimulator of hepatic fibrosis, many of the cytoprotective antioxidant effects of coffee are thought to be independent of the actual caffeine [Kalthoff et al. 2010]. The various forms of brewing coffee additionally complicate the ability to retain the antioxidant effect as the use of high pressured filtration versus ordinary filtration during preparation have been suggested to contain different levels of cafestol and kahweol [Anty et al. 2012]. While the exact mechanism of this effect or the amount of coffee required to provide significant benefit remains unclear, it is clear that the potential benefit of coffee needs to be further investigated.
This meta-analysis has several limitations. First, the included studies were quite heterogeneous methodologically. Second, several of our studies diagnosed NAFLD based on ultrasonography without the requirement for pathologic confirmation after liver biopsy. Third, as almost all of the studies measured caffeine intake through the use of a questionnaire at a single point in time, it is difficult to accurately represent caffeine intake over time. Recently, the ability to truly assess adequate intake of coffee accurately and evaluation of the nutritional and lifestyle behaviors of patients included in studies evaluating the role of coffee on NAFLD and hepatic fibrosis have been challenged [Anty et al. 2013]. Lastly, several confounders such as cigarette smoking, physical activity, diet, or socioeconomic factors were not included in this analysis.
The inclusion of over 20,000 patients was a significant strength of this meta-analysis. While cross-sectional and case-controlled studies have their inherent limitations, with the utilization of six studies we were able to generate a much greater statistical power compared with a single study [Mann, 2003]. Lastly, there was a diverse population studied without significant ethnic disparity.
In conclusion, our results suggest regular coffee caffeine consumption is significantly associated with reduced hepatic fibrosis in patients with NAFLD. Further research should be directed at understanding the potential beneficial components of regular coffee and determining the required amount that must be consumed and method of brewing to generate an advantageous effect. Given the potential benefits of regular coffee, patients with NAFLD should be encouraged to consume regular coffee daily.
Footnotes
Authors’ contributions
All authors have participated in conception and design, manuscript writing, and final approval of the manuscript.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The authors report no financial or personal conflicts of interest. This manuscript is not under consideration elsewhere.