
Abstract
Rates of transmission of hepatitis B virus (HBV) infection from organ donors with HBV markers to recipients along with reactivation of HBV during immunosuppression following transplantation have fallen significantly with the advent of hepatitis B immune globulin (HBIg) and effective antiviral therapy. Although the availability of potent antiviral agents and HBIg has highly impacted the survival rate of HBV-infected patients after transplantation, the high cost associated with this practice represents a major financial burden. The availability of potent antivirals with high genetic barrier to resistance and minimal side effects have made it possible to recommend an HBIg-free prophylactic regimen in selected patients with low viral burden prior to transplant. Significant developments over the last two decades in the understanding and treatment of HBV infection necessitate a re-appraisal of the guidelines for prophylaxis of HBV infection in solid organ transplant recipients.
Introduction
Liver transplantation for end-stage liver disease due to hepatitis B was associated with a substantially diminished graft survival until the mid-1990s because of the increased incidence of hepatitis B reactivation and graft loss in recipients. With the advent of antiviral agents such as nucleos(t)ide analogs and hepatitis B immune globulin (HBIg), however, the risk of reactivation of hepatitis B and graft reinfection has been substantially reduced. The overall current survival after liver transplantation for hepatitis B related cirrhosis exceeds 85% in the first year and 75% at year 5 [Kim et al. 2004; Steinmüller et al. 2002; Vargas et al. 2002], in contrast to a 2-year graft survival of 50% in the past [Starzl et al. 1989]. A combination regimen of lamivudine (LAM) and HBIg has been shown to reduce the hepatitis B virus (HBV) recurrence rate after transplant to <5% at 5 years [Markowitz et al. 1998]. Thus, with appropriate prophylactic therapy, liver transplantation in patients with chronic hepatitis B is now associated with excellent long-term outcomes. Although the availability of potent antiviral agents and HBIg has highly impacted the survival rate of HBV-infected patients after transplantation, the high cost associated with this practice represents a major financial burden in developed countries, as well as in HBV endemic countries with limited financial resources. This has led to the consideration of prophylaxis without HBIg for selected patients undergoing liver transplantation. Significant developments over the last two decades in the understanding and treatment of HBV infection necessitate a reappraisal of the guidelines for prophylaxis of HBV infection in solid organ transplant recipients.
HBV reinfection following liver transplantation in prior hepatitis B surface antigen positive recipients
Enhanced viral replication occurs due to the use of immunosuppressive medications in the post-transplant period [McMillan et al. 1995; Tur-Kaspa et al. 1988]. Extrahepatic reservoirs of HBV, predominantly the peripheral mononuclear cells and spleen [Omata, 1990], are the most likely sources of HBV reinfection after transplantation. The reappearance of hepatitis B surface antigen (HBsAg) and HBV DNA in the serum of an HBV-infected patient after liver transplantation is called reinfection (and not reactivation) because the HBV-infected liver is removed at transplantation and the new graft is reinfected by HBV virions present in the circulation or released from extrahepatic sites. Most cases of HBV reinfection occur in those who are hepatitis B extracellular antigen (HBeAg) positive with elevated HBV DNA levels in the serum at the time of transplantation. Reinfection occurs almost universally after orthotopic liver transplantation (OLT) in patients who are HBsAg positive but is uncommon in those recipients with anti hepatitis B core antigen (anti-HBc) without HBsAg [Markowitz et al. 1998]. The presence of HBV DNA in serum, as detected by sensitive polymerase chain reaction (PCR) assays, precedes the elevation of serum aminotransferases or reappearance of HBsAg. As untreated reinfection can lead to fibrosing cholestatic hepatitis, progressive liver disease or cirrhosis, it is important to monitor patients who are not receiving prophylactic therapy in the post OLT period, so that antiviral therapy can be initiated as soon as serum HBV DNA is detectable. Alternatively, some patients with detectable HBV DNA in the liver or peripheral mononuclear cells remain HBsAg negative with no clinical or histological evidence of recurrent HBV [Feray et al. 1990; Roche et al. 2003]. Owing to the enhanced sensitivity of the current HBV DNA assays, detection of low-level transient viremia without clinical evidence of reinfection has been noted. Patients with detectable HBsAg and persistent HBV DNA levels are at risk for clinical disease and graft loss [Fox and Terrault, 2012].
Strategies to prevent HBV allograft reinfection include HBIg monotherapy, a combination of HBIg and antiviral therapy, and antiviral monotherapy. These are discussed below.
HBIg monotherapy and combination therapy with antiviral agents
HBIg is a polyclonal purified preparation of human anti-HBs (hepatitis B surface antibody) derived from pooled plasma. In addition to neutralizing circulating virions, anti-HBs decreases HBsAg secretion by interacting with HBsAg within the cells after endocytosis by hepatocytes [Schilling et al. 2003]. Prophylaxis with HBIg has been shown to decrease reinfection, and improve patient and graft survival [Konig et al. 1994; McGory et al. 1996; Müller et al. 1991; Samuel et al. 1991, 1993; Sawyer et al. 1998]. The maximum benefit from HBIg is conferred when the total viral burden is lowest (the anhepatic phase) and also during the time of intense immunosuppression in the early post-transplant period, i.e. during the first 6–12 months after transplant.
Inhibition of viral replication using antiviral agents (LAM and adefovir ± LAM) in the pre- and immediate post-transplant period has been shown to protect grafts from HBV reinfection after transplant [Perrillo et al. 2001; Schiff et al. 2007; Yoshida et al. 2007]. These studies have also revealed the limitations of antiviral monotherapy, however. The emergence of drug resistance with LAM monotherapy limits its efficacy. Newer, more potent antivirals with higher genetic barriers to resistance such as tenofovir and entecavir have been shown to be safe in decompensated liver disease and effective in achieving HBV DNA suppression before transplant [Liaw et al. 2011], and hence are the recommended antivirals in patients with decompensated HBV cirrhosis.
Multiple studies have reported on the efficacy of combination therapy with HBIg and an antiviral agent in preventing HBV reinfection [Angus et al. 2000; Gane et al. 2007; Markowitz et al. 1998; Terrault et al. 2005]. Combination therapy has been associated with a significantly lower rate of both HBV-related and all-cause mortality compared with HBIg monotherapy, according to the results of a meta-analysis of two prospective and four retrospective studies [Loomba et al. 2008a]. A serum HBV DNA level greater than 100,000 copies/ml at the time of OLT is associated with a 50% risk for recurrent disease even with prophylactic therapy, whereas a pretransplant viral load less than 200 copies/ml carried no risk for recurrent disease [Marzano et al. 2005]. There was no difference in the observed HBV recurrence rate between patients treated with HBIg monotherapy versus combined HBIg and LAM prophylaxis in this study, probably due to comparably low viremic loads in both groups at the time of surgery. Antiviral therapy before transplant has been shown to reduce the risk of reinfection by reducing the circulating viral load at the time of transplant and prolonging the half-life of HBIg [Dickson et al. 2006]. Although a combination regimen of LAM and HBIg has been the standard of care for prevention of HBV reinfection in most transplant centers, a number of small studies have confirmed the efficacy and safety of entecavir [Xi et al. 2009] and entecavir plus tenofovir [Jimenez-Perez et al. 2010] when used in conjunction with HBIg after OLT.
The usual dose of HBIG is 10,000 intravenous units (IUs) as a bolus dose intravenously during the anhepatic phase, followed by daily doses during the first week and monthly thereafter or dosed according to anti-HBs titers. It has been suggested that, in addition to continuation of antiviral therapy, high-risk patients should receive intravenous (IV) HBIg during the first post OLT year and intramuscular (IM) HBIg in the second year, whereas low-risk patients receive IV HBIg for 1 week only [Degertekin et al. 2010; Nath et al. 2006; Wong et al. 2007]. A trough anti-HBs titer of >500 IU/l (or at least 100 IU/l) has been shown to reduce reinfection rates [McGory et al. 1996; Terrault et al. 1996].
Use of a lower dose of IM HBIg (400–800 IU daily for 7 days and monthly thereafter) along with LAM at 100 mg daily has been shown to cost less than 10% of the high-dose IV HBIg-based combination therapy, with an actuarial risk of HBV recurrence of only 1% at 1 year and 4% at 5 years [Gane et al. 2007]; however, more than half the patients in this study had undetectable HBV DNA at the time of transplant. Another study using 800 IU IM HBIg (daily for 6 days, weekly for 3 weeks and monthly thereafter) along with LAM resulted in a higher rate of prophylaxis failure (28% versus 8% p = 0.015) in those with HBV DNA ≥105 copies/ml at transplantation compared with those with HBV DNA levels <105 copies/ml [Zheng et al. 2006]. Thus, the risk of recurrence with the low-dose HBIg approach appears to be primarily determined by the level of HBV DNA at the time of transplantation.
Anti-HBs titers can vary within the same patient even with the administration of a fixed dose of HBIg. Hence, the strategy of dosing HBIg to achieve a specific anti-HBs titer in the serum requires more intensive monitoring of titers. A target trough anti-HBs titer of 50–100 IU/l is ideal, when antiviral agents are given in combination with HBIg for prophylaxis [Fox and Terrault, 2012]. The rate of virologic recurrence using IM HBIg and LAM was <8.2% over a 3–93 month follow-up period, when the anti-HBs titers were maintained between 50 and 100 IU/l [Karademir et al. 2006; Karasu et al. 2004]. Another approach that has been shown to be effective is to titrate the dose of IM HBIg from 400 to 1200 IU/l, where HBIg is administered every 2–4 weeks to achieve an anti-HBs level of ≥100 IU/l [Jiang et al. 2010]. Thus, low-dose IM HBIg along with antiviral therapy may be a cost-effective strategy for prophylaxis. A randomized study that examined continuation of HBIg plus LAM versus switching over to LAM plus adefovir after 1 year of combination therapy with HBIg and LAM post-transplant showed significant cost reduction in the adefovir plus LAM group with only one patient in this group becoming transiently positive for HBsAg [Angus et al. 2008]. Most patients in this study were at low risk of recurrence, however, and a quarter of the patients had undetectable viral DNA at the time of transplant. More importantly, HBIg therapy was stopped only after the first post-transplant year, which is the most vulnerable period for reinfection. Another randomized controlled study evaluated the feasibility of discontinuation of HBIg 1 month after transplant in those who received a combination of LAM and HBIg therapy with an 18-month follow up [Buti et al. 2003] and a subsequent longer-term follow up of the same cohort [Buti et al. 2007]. The cases of HBV DNA and HBsAg positivity occurred in association with poor adherence to antiviral therapy upon discontinuation of HBIg, providing support for the feasibility of this practice in adherent patients who are on effective antiviral therapy. Strategies employing active immunization using HBV vaccination after transplantation as a replacement for HBIg infusions have yielded inconsistent results with either lack of initial response or failure to maintain protective anti-HBs levels [Angelico et al. 2002; Rosenau et al. 2007], and are hence not recommended.
In our opinion, antiviral therapy should be considered prior to OLT in all patients with positive serum HBV DNA and continued indefinitely after transplant, regardless of the magnitude of the viral load. The loss of HBs Ag after OLT is postulated to be attributable to the sudden decrease in viral load upon removal of the infected native liver and the effect of antiviral suppression. In spite of effective prophylaxis with HBIg and antivirals and the absence of detectable HBV DNA/HBsAg in serum, HBV can still be detected in the allograft and peripheral mononuclear cells, and may be the source of HBsAg [Coffin et al. 2011]. There have been reports of reinfection in patients who are maintained on HBIg prophylactic therapy [Carman et al. 1996; Ghany et al. 1998; Hawkins et al. 1996; Protzer-Knolle et al. 1998]. These cases may be due to inadequate dosing of HBIg or, more importantly, due to the emergence of HBIg-induced mutant virus that can escape neutralization. These findings underscore the importance of continuation of prophylactic antiviral therapy after OLT. It is also likely that the HBsAg positivity in recipients in this setting may not lead to an adverse outcome.
HBIg-free prophylaxis
Given the availability of more potent drugs such as entecavir with high genetic barrier to resistance and lack of nephrotoxicity, the role of HBIg therapy is diminishing. A recent study of 80 consecutive patients with chronic HBV undergoing liver transplantation on an HBIg-free regimen of entecavir monotherapy found a 91% loss of HBsAg and 98.8% achievement of serum HBV DNA clearance over a median follow-up time of 26 months post OLT [Fung et al. 2011]. In this study, low pretransplant HBV DNA level in itself was not significantly associated with HBsAg loss, but a combination of low HBV DNA level (<5 log10copies/ml) with low HBsAg level (<3 log10IU/ml was associated with a 100% HBsAg loss at 18 months. It should be noted that no resistance mutations were identified on entecavir monotherapy after a median follow up of 26 months. The results of this study suggest that antiviral therapy alone (with potent agents such as entecavir) without HBIg effectively prevents reinfection in at least low-risk recipients with undetectable viral load at the time of transplant. The recipients at low risk for HBV reinfection include those with negative HBeAg and low viral load (<20,000 IU/ml), fulminant HBV or coinfection with HDV (Vargas et al., 2002). Thus, patients achieving viral suppression pretransplant are the best candidates for an HBIg-free prophylaxis strategy.
However, potential liver transplant recipients with known antiviral drug resistance and those who have positive or negative HBeAg with high viral load (>20,000 IU/ml) are considered to be at high risk for HBV reinfection [Marzano et al. 2005; McGory et al. 1996; Omata, 1990]. Despite the lower reinfection rates in patients with HDV coinfection, this may represent a group in whom an HBIg-free strategy is not suitable because of the need to rapidly remove all circulating HBsAg in order to halt HDV reinfection of the graft in the immediate postoperative period. Thus patients with detectable HBV DNA, known antiviral resistance, higher risk for recurrence of hepatocellular carcinoma (HCC) and limited options if prophylactic antiviral therapy fails are not ideal candidates for an HBIg-free strategy and will need long-term HBIg in conjunction with antiviral agents [Fox and Terrault, 2012] (Table 1).
Candidates for antiviral monotherapy versus combination therapy for HBV prophylaxis.

HBeAg, hepatitis B extracellular antigen; HBIg, hepatitis B immune globulin; HBV, hepatitis B virus; HCC, hepatocellular carcinoma; HDV, hepatitis D virus; HIV, human immunodeficiency virus; IU, intravenous unit.
HBV infection following OLT in prior HBsAg negative recipients
HBV infection after OLT is discussed below in the following categories: liver transplantation from donors with isolated hepatitis B core immunoglobulin G (anti-HBc IgG), transplant recipients with isolated anti-HBc IgG, and transplantation from donors with no positive HBV markers.
Liver transplantation from isolated anti-HBc IgG positive donors
Prior studies have shown a substantial risk of acquiring HBV infection in recipients who receive livers from donors who are anti-HBc positive [Dickson et al. 1997; Prieto et al. 2001; Wachs et al. 1995]. Although recipients who have positive anti-HBs and/or anti-HBc at the time of OLT are considered less likely to acquire HBV infection from an anti-HBc positive donor [Prieto et al. 2001], HBV infection has been noted to occur in recipients who have protective surface antibody from vaccination or prior infection [Dickson et al. 1997]. Thus, the risk of acquiring HBV infection cannot be prevented solely by directing anti-HBc positive livers to those recipients with anti-HBs and administration of prophylactic antiviral therapy is essential in such settings.
HBIg monotherapy for the prevention of infection is considered inferior to antiviral therapy due to the inability of the HBIg to inhibit HBV replication [Roche et al. 2010]. A systematic review analyzing the incidence of de novo hepatitis B infection in liver transplant recipients from donors who were HBsAg negative and anti-HBc positive showed an incidence of 2.7% in patients receiving LAM only prophylaxis versus 3.6% in patients receiving HBIg plus LAM combination therapy [Saab et al. 2010]. The median follow-up time for the monotherapy group was 25.4 months, whereas the median follow-up time for the LAM + HBIG group was 31.1 months. The investigators concluded HBIg + LAM combination therapy was no more effective than LAM only treatment. Owing to the high rate of drug resistance with LAM, entecavir is now the preferred first line antiviral agent in the nucleoside naïve patient. Although many experts have recommended combination therapy, the lack of data to support this recommendation together with the high genetic barrier to resistance with entecavir likely obviate the need for combination therapy in this setting. There is a cost difference of US$79,395 during the first year with the use of LAM monotherapy at a dose of 100 mg per day compared with LAM + HBIg therapy at a dose of 10,000 IU of HBIg daily for 7 days and then monthly (excluding the costs of office visits and HBIG administration) [Saab et al. 2009, 2010]. A newer generation antiviral such as entecavir, at a dose of 0.5 mg/day given as monotherapy, is associated with a cost reduction of US$73,772 compared with LAM + HBIg combination therapy. Hence, indefinite antiviral monotherapy (without HBIg) is recommended for prophylaxis in this setting.
Isolated anti-HBc IgG positive recipients
Although reactivation of HBV replication (positive HBV DNA on liver biopsy) has been reported in recipients who are HBsAg negative but anti-HBc positive pretransplant, none of the recipients became HBsAg-positive or developed clinical hepatitis B after transplantation. Thus, prophylactic antiviral therapy is not warranted routinely after liver transplantation in HBsAg-negative, anti-HBc-positive recipients [Abdelmalek et al. 2003]. It is reasonable to monitor HBV DNA and alanine transaminase (ALT) periodically in the post OLT setting in those who are not receiving prophylactic therapy, particularly if they do not have or lose the protective surface antibodies over time. Such patients should be considered for antiviral therapy as soon as serum HBV DNA is detectable.
Liver transplantation from donors with no positive HBV markers
Although this scenario is associated with the lowest risk of HBV transmission, there have been reports of de novo HBV infection occurring in OLT recipients who received livers from donors with no positive serologic markers of HBV infection [Chazouilleres et al. 1994; Ghisetti et al. 2004]. This may be explained by the presence of occult HBV infection in these donors, as evidenced by the presence of HBV DNA in their serum or liver tissue. Prophylactic treatment of the recipient is not recommended. HBV transmission in this setting can be largely prevented by routinely vaccinating all potential OLT recipients.
Tables 2, 3, and 4 summarize risk stratification, suggested prophylactic regimens and monitoring algorithms for patients following liver transplantation. As shown in Table 2, the antiviral agent of choice for HBV prophylaxis in solid organ transplant recipients is entecavir due to its relative lack of nephrotoxicity, unless the patients were on LAM, tenofovir or emtricitabine/tenofovir pretransplant, in which case the same antiviral agent is continued post-transplantation.
Choice of antiviral agent and dosage.*
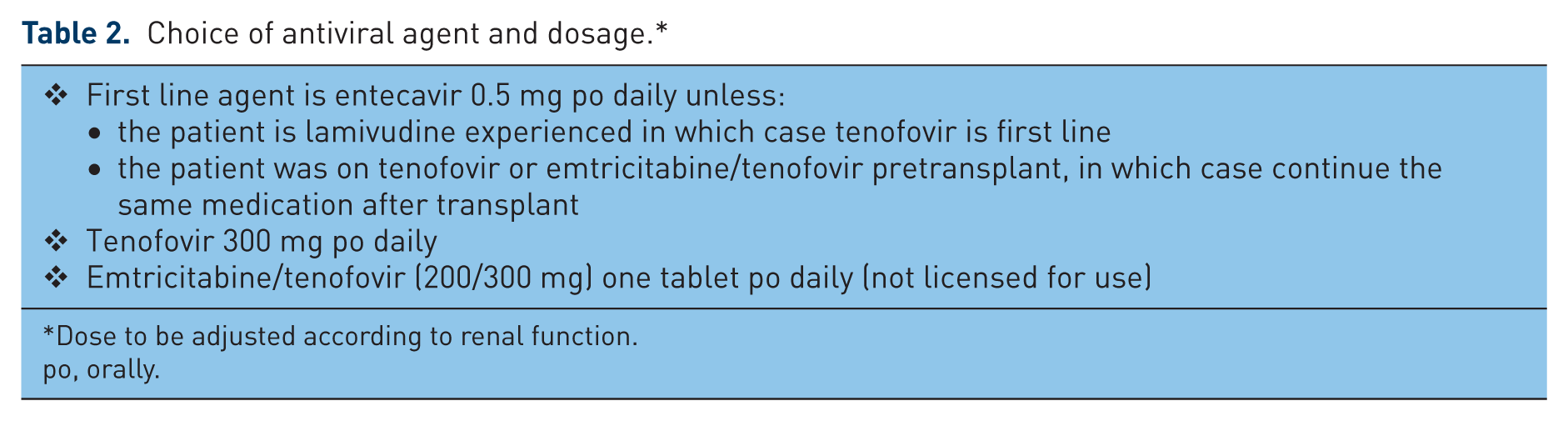
Dose to be adjusted according to renal function.
po, orally.
Suggested HBV prophylaxis in liver transplant recipients.

If HBV DNA level at OLT is not known or details of drug resistance are not known or if the patient is on two anti-HBV medications at the time of OLT, patient is considered high risk and treated accordingly.
If HBsAg is positive on day 3, then the dose of HBIg is continued to day 7.
IM HBIg only if INR <1.5 and platelets >50K; if not, give IV; the dose of IM HBIg is adjusted between 400 and 1200 IU IM (at 400 IU increments) to achieve a trough anti-HBs titer of ≥100 units/l.
Discontinuation of HBIg prophylaxis in adherent patients who are on effective antiviral agents with high genetic barrier to resistance therapy may be considered on an individual basis, once persistent viral suppression has been achieved. These patients should be monitored indefinitely for emergence of drug resistance with periodic HBV DNA testing while on treatment.
anti-HBc, anti-hepatitis B core antigen; anti-HBs, human anti-HBs; HBIg, hepatitis B immune globulin; HBsAg, hepatitis B surface antigen; HBV, hepatitis B virus; IM, intramuscular; IU, intravenous unit; IV, intravenous; OLT, orthotopic liver transplantation.
Monitoring of HBV patients post liver transplant and approximate cost of prophylactic therapy.

Based on data available from (Saab et al., 2009; Abdelmalek et al., 2003) and Epocrates® Online (https://online.epocrates.com); excludes expenses for medication administration, office/nurse visits and laboratory monitoring.
anti-HBs, human anti-HBs; HBIg, hepatitis B immune globulin; HBsAg, hepatitis B surface antigen; HBV, hepatitis B virus; IM, intramuscular; IV, intravenous.
Prophylaxis in other solid organ transplant recipients
Before the advent of effective antiviral agents for treatment of HBV infection, the presence of hepatitis B infection was considered a contraindication for organ transplantation. HBsAg positivity has been shown to be associated with an increased risk of renal allograft loss and death [Fabrizi et al. 2005]. The risk of re-activation of HBV is higher in the HBsAg positive recipient with detectable HBV DNA or HBeAg positivity compared with a HBV carrier with no detectable DNA or HBeAg [Fairley et al. 1991]. The risk of HBV infection is highest when an HBV negative recipient receives an organ from an HBsAg positive donor; it is lower if the HBV negative recipient receives the organ from an HBsAg negative but anti-HBc positive donor, and the lowest if the recipient has protective anti-HBs antibodies [Wachs et al. 1995].
The two primary approaches to prevent HBV reactivation after renal transplantation are prophylactic and preemptive strategies, in addition to routine vaccination of all prospective recipients who are not immune. The prophylactic strategy involves administration of antiviral agents prior to transplantation in patients who are at risk for reactivation. The preemptive strategy involves using sensitive PCR assays to detect HBV DNA in the post-transplant period (ideally every 3 months in the first year and 6-monthly thereafter), with prompt treatment in the event of persistent or progressive rise of HBV DNA. There have been no studies that have compared the two approaches in the renal transplant setting. Although preemptive LAM therapy based on serial HBV DNA levels and clinical monitoring has been shown to improve the survival of HBsAg-positive renal allograft recipients [Chan et al. 2002], many studies have shown the efficacy of prophylactic approach in both kidney transplant [Lewandowska et al. 2000; Park et al. 2001] as well as in nonkidney transplant setting where patients undergo chemotherapy for malignancy [Loomba et al. 2008b; Perrillo, 2001]. Observational studies have also suggested that treatment of HBV reactivation after detection of aminotransferase elevation is less effective in terms of preventing hepatic flares or hepatic decompensation than either a prophylactic or preemptive strategy [Fabrizi et al. 2005; Filik et al. 2006].
Hence, it appears reasonable to consider a prophylactic approach in situations where HBV DNA is detectable either in the donor or recipient and the preferred antiviral agent is entecavir (dosed according to renal function) due to its relative lack of nephrotoxicity. In all other cases, where HBV markers may be present either in the donor or recipient but with undetectable HBV DNA, a preemptive approach may be considered. The approach described here for prophylaxis of HBV infection in renal transplant recipients can be extrapolated to other solid organ transplant recipients but there are less data in these settings. The suggested regimen for prophylaxis of HBV infection in other solid organ transplant recipients is presented in Table 5.
Summary of prophylaxis for kidney/heart/lung/pancreas transplant recipients.

In cases where HBV DNA status is not known, assume HBV DNA (+) and provide prophylaxis accordingly. The use of donor HBV DNA testing is suggested given the potential risk of transmission with detectable HBV DNA (McMillan et al., 1995).
anti-HBc, anti-hepatitis B core antigen; HBsAg, hepatitis B surface antigen; HBV, hepatitis B virus; IgG, immunoglobulin G.
Conclusion
Rates of transmission of HBV infection from organ donors with HBV markers to recipients along with reactivation of HBV during immunosuppression following transplantation have fallen significantly with the advent of HBIg and effective antiviral therapy. The availability of potent antivirals with high genetic barrier to resistance and minimal side effects have made it possible to recommend an HBIg-free prophylactic regimen in selected patients with low viral burden prior to transplant. While this approach has not yet been proven sufficient for all organ recipients, it is likely that we can recommend a universal HBIg-free prophylactic strategy in the near future pending results of more definitive studies. This strategy could lead to a significant curtailment of health care cost without compromising long-term graft and recipient outcomes. Surveillance of HBV DNA is critical for early detection of new or recurrent infection because the appearance and rise of HBV DNA can precede development of necroinflammatory disease by weeks. Early implementation of antiviral therapy can effectively forestall graft or life threatening HBV infection.
Footnotes
Funding
R.C. has received research grants from Gilead and Roche/Genentech.
Conflict of interest statement
The authors declare no conflicts of interest in preparing this article.