
Abstract
Stress-related psychopathology is on the rise, and there is a pressing need for improved prevention strategies. Positive appraisal style, the tendency to appraise potentially threatening situations in a positive way, has been proposed to act as a key resilience mechanism and therefore offers a potential target for preventive approaches. In this article, we review n = 99 studies investigating associations of positive cognitive reappraisal, an important sub-facet of positive appraisal style, with outcome-based resilience and relevant other outcomes, which are considered resilience-related. According to the studies reviewed, positive cognitive reappraisal moderates the relation between stressors and negative outcomes and is positively related to several resilience-related outcomes. It also mediates between other resilience factors and resilience, suggesting it is a proximal resilience factor.
Life is stressful. While living our lives, we are forced to adapt to all kinds of changes in the environment and within ourselves, which provokes short-term responses and long-term modifications of our physiological, cognitive, and behavioral systems. The acute stress response per se is not necessarily detrimental but first and foremost a crucial adaptive reaction to changing demands and inherent to life, enabling survival and the development of knowledge and skill. As Hans Selye, father of the term ‘stress’, pointed out: ‘[…] complete freedom of stress is death!’ (Selye, 1976).
However, when stressors become chronic or exceed our abilities to cope with them, they provoke a state of imbalance called allostatic overload (McEwen & Wingfield, 2003), which can lead to the development of psychopathology. Stress-related disorders such as depression or anxiety are a major cause of disability in our modern societies. Between 1990 and 2017, major depression continuously resided within the four leading reasons for years lived with disability globally, with its contribution rising over time (Spencer et al., 2018). Stress-related disorders do not only pose an immense individual burden on affected persons and their social environment; due to healthcare expenses and losses of productivity and income they also create vast economic costs that are estimated even higher than those for somatic disorders (Trautmann et al., 2016).
Resilience
Even though the link between stress and psychopathology has been known for decades, the prevalence of mood and anxiety disorders has not decreased between 1990 and 2015, which is likely due to the suboptimal implementation of clinical practice guidelines and a lack of attention to preventive strategies (Jorm et al., 2017). At the same time, the notion that most people do not develop psychological disorders after adversity or trauma (Berntsen et al., 2012; Bonanno et al., 2006; Feder et al., 2009; Galatzer-Levy et al., 2014; Galatzer-Levy & Bonanno, 2012, 2014) led to a perspective shift, away from stress research and towards resilience research. Resilience is conceptualized as the maintenance or quick recovery of a healthy mental state during and after adversity (Bonanno et al., 2011; Kalisch et al., 2017). Resilience research, the investigation of factors and mechanisms that contribute to effective stress adaptation, is a constructive and health-oriented approach that complements disease-oriented studies of psychopathology by promoting adaptive skills and strategies that circumvent potentially harmful effects of stress.
Whereas resilience has often been described as a trait or ability (Schultze-Lutter et al., 2016; Tugade & Fredrickson, 2004) and is assessed with self-report questionnaires (Connor & Davidson, 2003; Smith et al., 2008), a recent, more broadly accepted conceptualization argues that resilience should be assessed as an outcome (Kalisch et al., 2017; Mancini & Bonanno, 2009; Seery et al., 2010). The main idea of mental resilience as an outcome is that an affected person does not develop significant long-term mental health problems despite being exposed to adversity (which can for example be chronic exposure to stressors, single negative life events, or challenging life transitions). A related definition from the American Psychological Association rather emphasizes the processes that lead to such good long-term mental health outcomes. It describes resilience as ‘[…] the process of adapting well in the face of adversity, trauma, tragedy, threats or significant sources of stress […]’ (American Psychological Association, 2010). This definition emphasizes an active and dynamic component to successfully dealing with stressors. Both the outcome- and process-based definitions are closely related and common in the scientific field of resilience research and, in contrast to the trait-based definition, take into account the actual experience of adversity (ranging from daily hassles to traumatic events) as a necessary part of determining somebody's resilience (Kalisch et al., 2017; Mancini & Bonanno, 2009; Russo et al., 2012). At the same time, both definitions allow for the existence of trait-like entities that can make a resilient response to stressors more likely. These predisposing entities are called resilience factors and comprise all those bio-psycho-social variables that statistically predict resilience. Resilience factors increase the likelihood of a resilient outcome by activating resilience mechanisms, processes of successful adaptation that actively operate whilst dealing with a given stressor (Kalisch et al., 2017; Russo et al., 2012).
In the current review, we focus on resilience as an outcome, or outcome-based resilience. To operationalize outcome-based resilience, resilience studies should be longitudinal, with a baseline measure of mental health, a quantification of exposure to stressors, and at least one follow-up mental health measure, preferably several. Importantly, all changes in the outcome variable should be normalized by stressor load between baseline and follow-up. This excludes the possibility that differences in mental health outcomes can trivially be explained by inter-individual differences in stressor exposure. Resilience is then operationalized as a positive or non-negative outcome despite a certain exposure to stressors and one can ask which factors predict such outcomes (resilience factors) or which processes of change observed longitudinally in some other measure statistically explain the outcome (resilience processes; for in depth discussion, see Kalisch et al., 2015, 2021).
Research that investigates mental health and well-being without normalizing for stressor load or without exploring the possible moderating role of a proposed resilience factor on the stressor-outcome relationship should thus not be considered resilience research as such. It can, however, offer first insights that resilience researchers could incorporate in more rigorous study designs, which is why studies that do not specifically consider stressor exposure can be valuable to review. This may be the case, for instance, in studies only assessing mental health outcomes. We term these outcomes resilience-related as opposed to resilience outcomes proper.
Emotion Regulation and PASTOR
Being stressed (the stress reaction) is an emotional response that includes not only the subjective experience, but also changes in perception, attention and thinking, physiological activation on different levels – e.g., the autonomic nervous system (ANS), the hypothalamus-pituitary-adrenal (HPA) axis, and the brain (Dedovic et al., 2009; Lazarus & Folkman, 1984; McEwen & Stellar, 1993; van Oort et al., 2017) - and associated behavioral tendencies or overt behavior (Mauss & Robinson, 2009). Already quite early it has therefore been suggested that emotion regulation is important for coping with adversity. In fact, disturbed emotion regulation is associated with a variety of mental disorders (Sheppes et al., 2015). More specifically, how we appraise a potentially stressful event – for instance as threatening or as challenging – plays an important role and determines our emotional responses to the event (Arnold, 1969; Lazarus & Folkman, 1984; Scherer, 1984).
The Positive Appraisal Style Theory of Resilience (PASTOR) suggests positive appraisal style (PAS) to be the key resilience mechanism through which all resilience factors converge and exert their effects on resilience (Kalisch et al., 2015). PASTOR assumes that people have a global appraisal style, which means that people have a more or less pronounced habitual tendency to appraise stressors in a certain way, and that a tendency, or bias, to appraise stressors positively can be protective against a variety of symptoms when exposed to a variety of stressors. Positive appraisal is positive in the sense of not negative: It first and foremost eschews negative biases, such as pessimism, catastrophizing, and learned helplessness. Thus, whereas it comprises threat estimations that range from accurate, or realistic, to slightly positive, it does not entail blind optimism and extremely positive appraisals that are delusional. Such a mildly positive appraisal allows for a fine-tuned, optimal stress response. Adequate stress reactions are provoked whenever needed, while avoiding stress responses that are too strong or too extended. Thereby, an excessive consumption of resources and allostatic overload is prevented.
The authors of PASTOR claim that in mildly adverse situations, positive appraisal can be easily attained by processes that involve more or less automatic positive situation classification, based on comparison with earlier, successfully managed situations or positive cultural stereotypes (process class 1). When, however, an aversive situation is strong enough to automatically trigger negative appraisals, a reappraisal (i.e., re-evaluation) of the situation is in any case required to appraise the situation positively (process class 2). Such reappraisal processes can stretch from implicit, unconscious, non-volitional, effortless, and nonverbal to explicit, conscious, volitional, effortful, and verbal. Positive reappraisal processes can result in ‘safety learning’ about reduced probabilities of actual threat (e.g., extinction of previously learned stimulus-response relationships, discrimination of non-threat-predictive from threat-predictive stimuli, or recovery after stressor offset) or can lead someone to weigh the positive and negative aspects of a given situation towards a more positive interpretation or to positively reconstrue the meaning of a situation (e.g., in ‘positive cognitive reappraisal’ (PCR), as an example of a conscious, volitional and effortful reappraisal process). Importantly, reappraisal not only entails strategies specifically aimed at upregulating positive emotion, but all processes that result in an overall more positive (i.e., less negative) evaluation of the situation. Successful reappraisal may require the inhibition of competing negative interpretations and the already happening stress response (process class 3; Kalisch et al., 2015).
PASTOR claims that PAS is both 1) a resilience factor and should thus moderate the association between stressors and negative outcomes, and 2) the key resilience mechanism, ultimately mediating the relationship between other resilience factors and resilience. This means that other resilience factors (such as received or perceived social support, socio-economic status, a certain genotype, brain structure or function, or other emotion regulation skills) promote resilience by promoting positive appraisal of potentially stressful situations, and PAS is a more proximal cause for resilience compared to other, more distal factors. This PASTOR claim can be illustrated with the example of social integration, that is, a combination of received social support (which has the potential to change stressor exposure by providing actual help), and perceived social support (which has the potential to change stressor appraisal by enhancing perceived coping resources). Higher stressor exposure generally is associated with a higher mental burden load (Agid et al., 2000; Shields & Slavich, 2017), and PAS as a resilience factor moderates this relationship. Social integration, a resilience factor in its own right, is negatively associated with mental burden load (Ozbay et al., 2007), but this association should be fully mediated by both the effects on reduced stressor exposure (received support) as well as increased PAS (perceived support), rendering the direct path non-significant (see Figure 1A). This makes PAS a more proximal resilience factor than social integration. For resilience factors that likely do not influence stressor exposure (e.g., a certain genetic background that influences threat processing), this effect is entirely mediated via PAS according to the theory (see Figure 1B).
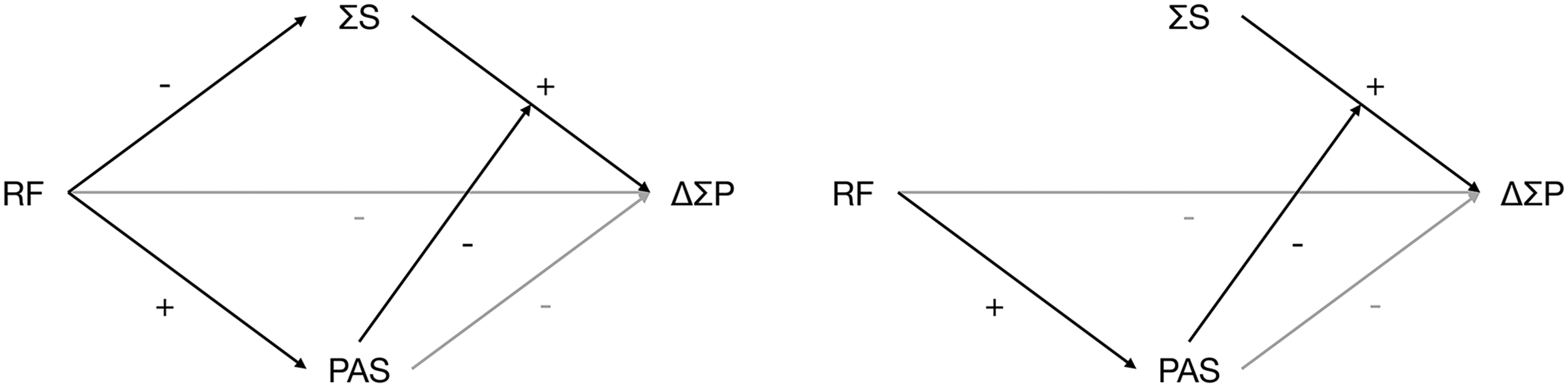
Expected patterns of moderating and mediating influence of positive appraisal style (PAS) in line with PASTOR. We expect the same relationship for positive cognitive reappraisal, it being a sub-process of PAS. Note: RF = resilience factor, ΣS = absolute stressor exposure, PAS = positive appraisal style, ΔΣP = change in mental burden load.
The example highlights that PASTOR does not necessarily contradict resilience theories that emphasize non-appraisal-related resilience factors. Next to theories invoking the role of social support, this also applies to theories that emphasize the importance of regulatory flexibility (Aldao et al., 2015; Bonanno & Burton, 2013; Kashdan & Rottenberg, 2010). In fact, PASTOR allows for the existence of other resilience factors than PAS. However, it does posit that their effects on resilience are in the end mediated by PAS. For example, applying both appraisal-based and non-appraisal-based emotion regulation strategies (such as distraction) as seems suitable for different stressful situations may well be shown to promote resilience, but according to PASTOR would do so only if such flexible regulation abilities lead to a more generalized benign stressor appraisal, in particular on the appraisal dimension of coping potential or power (Lazarus & Folkman, 1984; Scherer et al., 2001).
Positive Cognitive Reappraisal
A much-studied topic is PASTOR's second process class: reappraisal. Within this process class, positive cognitive reappraisal (PCR) specifically has been proposed to play a crucial role in moderating the relationship between stressors and resilience (Troy & Mauss, 2011). The study specifically of PCR can be categorized into different modes of assessment (observed, induced) and different time scales (trait, situational). ‘Observed’ refers to quantifications of PCR extent, whereas ‘induced’ refers to training studies and other elicitations of a not necessarily specifically quantified PCR state. ‘Trait’ refers to a reported stable tendency, whereas ‘situational’ refers to actual PCR use.
Observed trait PCR according to this classification is what others termed the tendency to choose an emotion regulation strategy (Silvers & Guassi Moreira, 2019) or subjective reports of long-term emotion regulation frequency (McRae, 2013). It is usually assessed by self-report questionnaires retrospectively measuring the tendency to use (the frequency of) typical PCR processes, such as the Emotion Regulation Questionnaire (ERQ; Gross & John, 2003) or the Cognitive Emotion Regulation Questionnaire (CERQ; Garnefski et al., 2001). The ERQ is a 10-item-instrument that assesses habitual PCR, operationalized as a change in thinking about a current situation with the goal to improve one's emotional state, next to habitual expressive suppression (the tendency of keeping emotions to oneself). An example item of the ERQ's reappraisal subscale is ‘When I want to feel less negative emotion, I change the way I’m thinking about the situation’. The CERQ consists of nine subscales assessing whether different emotion regulation strategies are typically used when being confronted with negative events. The two prototypical positive reappraisal subscale items retained in the short version of the CERQ (Garnefski & Kraaij, 2006b) are ‘I think I can learn something from the situation’ and ‘I think that I can become a stronger person as a result of what has happened’. Hence, PCR in the CERQ is more narrowly understood as reappraising a situation as conducive to growth. These questionnaires are self-report instruments and as such are not immune to biases that emerge due to retrospective reporting or self-narratives. In terms of PASTOR, they may not always clearly discriminate neuro-cognitive processes belonging to the process class of reappraisal from processes contributing to the first process class in PAS, namely positive situation classification (a statement such as in ‘I think that the situation also has its positive sides’ might also reflect relatively effortless and stereotypical positive appraisal).
Another type of observed PCR is observed situational PCR. Here, studies either assess the frequency of spontaneously used PCR in daily life via diary or ecological momentary assessment (EMA) studies (equally referred to as subjective reports of long-term emotion regulation frequency by McRae (2013), with the difference that it is now assessed in daily life instead of using trait questionnaires). As an alternative to assessing PCR use, studies quantify spontaneous PCR ability or inventiveness via task performance. PCR ability tasks investigate emotional experience or physiological responses towards aversive stimuli, operationalizing PCR ability (effectiveness, success) as the difference in outcome between an instructed reappraisal and a control condition. This type of observed situational PCR has been also called the capacity to implement an emotion regulation strategy (Silvers & Guassi Moreira, 2019) or (short-term) emotion regulation success (Ford & Troy, 2019; McRae, 2013)). Importantly, although the experimental tasks instruct participants to use reappraisal, this type of observed situational PCR is not to be confused with induced PCR (introduced below). Whereas induced PCR investigates the effects of a reappraisal induction on subsequent outcomes, observed situational PCR is a quantification of reappraisal success. PCR inventiveness tasks assess the number of distinct reappraisals generated in response to presented vignettes (Weber et al., 2014). Similar to trait questionnaires, these EMA- and task-based measures of PCR may not allow sharp discrimination with respect to positive situation classification. While situational observations may inform about PCR in specific life situations or phases, or towards specific types of adversity, they are sometimes also used to infer trait-like PCR tendencies, such as in studies where task performance is used as an alternative, non-self-report-based predictor of resilience outcomes. Whereas studies using PCR ability tasks are less fraught with the typical biases of self-report (trait and EMA questionnaire) measures, all observational operationalizations of PCR merely offer associational research approaches.
Studies on induced PCR investigate the effects of experimental reappraisal inductions on resilience or resilience-related outcomes. PCR can either be induced by training studies in which the use of reappraisal is trained over a period of at least several days (induced trait PCR), or by instructions to reappraise while being in a laboratory setting, where the dependent variable is not reappraisal ability but the effect of such an induction on tertiary variables like state anxiety (induced situational PCR). These approaches do not rely on self-report and, most importantly, have the potential to give additional information on a possible causal relationship between PCR and resilience.
Aim of This Review
This review aims to give an extensive overview of published studies that provide insights into the association between PCR and resilience, as well as resilience-related outcomes. The following key questions are guiding this overview: Firstly, does the literature support the idea of PCR being a resilience factor, that is, moderating the relationship between stressor exposure and an associated lower health or well-being (key question 1)? For example, a person who is currently going through a stressful life period could be less likely to experience subclinical internalizing symptoms if they habitually cognitively reappraise a lot. Although PASTOR allows other sub-processes than PCR to contribute to its overarching reappraisal process class, it is here assumed that PCR is such an important member of this process class that the absence of evidence for it to be a resilience factor would be a challenge to the theory. Further, finding evidence for an association between PCR and resilience would allow us to postulate that training individuals in this specific process might be a promising strategy to promote resilience. Secondly, is there evidence for PCR mediating the relationship between other resilience factors and resilience, suggesting it might be a more proximal resilience factor than those other factors (key question 2)? Note that since PCR is only a sub-process of PAS, we do not assume it to be the single central resilience mechanism, but still expect it to be more proximal to resilience than other factors. An example for such a mediation could be that other emotion regulation strategies, such as distraction or variable use of different emotion regulation strategies, eventually lead a person to cognitively re-evaluate stressful situations as less negative in general, which, in turn, reduces the situation's impact on the person's mental well-being. Note that, because PASTOR does not postulate PCR to be the only constituent of PAS, absence of mediation by PCR would not challenge the theory; however, presence of mediation would further underscore the importance of PCR in resilience and further suggest that promoting it might be especially beneficial for resilience.
To answer these two key questions, we will have a closer look at studies investigating relationships between observed trait PCR, observed situational PCR (i.e., interindividual differences in the ability to use PCR in different situations like reappraising videos or pictures, or the frequency of spontaneous PCR use in daily life, which indirectly should also reflect trait-like PCR), or induced trait PCR (trainings of several days/weeks that have the potential to influence PCR habits) on the one hand, and both resilience and resilience-related outcomes on the other hand. Studies investigating induced situational PCR (i.e., where participants are instructed to use reappraisal in a laboratory setting, and effects on tertiary variables are assessed) will not be included since we do not expect them to have an influence on PCR tendencies, due to their short timeframe.
We assume that a relationship between PCR and resilience would be unlikely if it did not appear in cross-sectional studies employing resilience-related outcomes, given that cross-sectional studies have the tendency to overestimate effect sizes (Allison, 2021). We therefore first test for consistent associations between PCR and resilience-related outcomes in cross-sectional data as a necessary but not sufficient condition for inferring true effects. For outcomes with sufficient evidence, we will provide meta-analytic syntheses. We will then progress to the longitudinal studies that have a higher evidentiary value regarding resilience, and put an emphasis on those that also provide stressor measures.
Methods
The following search was conducted in PubMed, Web of Science, and PsycINFO on July 1st, 2020: reappraisal AND (resilience OR (symptoms AND (depressive OR anxiety OR somatic OR internalizing OR psychiatric)) OR (stress AND (response OR recovery OR perceived)) OR (well-being AND (mental OR physical))).
We included studies on mentally healthy adults with or without experiences of increased stressor load, including patients with a somatic diagnosis. The latter, as well as samples consisting of specific professionals such as firefighters, nurses, or rescue workers were considered to be samples with a regular increased stressor load. Importantly, we also included studies that assessed symptom measures of anxiety and depression in healthy populations without diagnoses. Whereas outcomes noticeably have less variability in these populations due to the fact that scores are predominantly sub-clinical, an elevated, but sub-clinical score does reflect an increased mental burden that can even entail the risk of eventually transitioning into an actual disease state. Investigating this sub-clinical but burdened state is therefore of particular interest for resilience research.
Studies had to report at least a correlation between at least one measure of PCR on the one hand, and at least one outcome measure of resilience or of a resilience-related outcome on the other hand. Resilience-related outcomes included in this study were general mental health, depressive symptoms, anxiety symptoms, or psychological factors related to subjective stress or well-being (i.e., positive affect, life satisfaction, quality of life, questionnaire resilience, self-efficacy, self-esteem, and, negatively, loneliness, perceived stress, and negative affect), measured in the absence of information on stressor exposure. Studies focusing on other positive outcome measures, such as academic performance, were not included in this review due to the missing relation with mental health or well-being.
Moderation analyses were included if they investigated whether PCR moderates the relationship between the exposure to stressors and a resilience-related outcome (that is, whether PCR was associated with resilience). Whereas we did include studies that examined the influence of tertiary independent variables whose influence on resilience or the resilience-related outcome measure was mediated by PCR, papers that merely investigated PCR as the dependent variable (e.g., comparing levels of reappraisal in different groups) were excluded, given the lack of quantitative association with an outcome related to mental health or well-being.
Studies applying an experimental PCR induction were included if they investigated the effects of this training on resilience or a resilience-related outcome in real life.
Selection of studies was limited to papers published in peer-reviewed journals in English language. If the same sample was examined in two publications, results from the second study were only included if they investigated a different dependent variable than the first one. Papers that were missed by the search terms but were found in reference lists or pointed out by reviewers were included if they met the inclusion criteria.
Figure 2 shows the PRISMA flow diagram of literature selection. A characterization of included studies can be found in Figure 3. An overview of all 99 selected publications is available in supplementary tables S1 and S2.
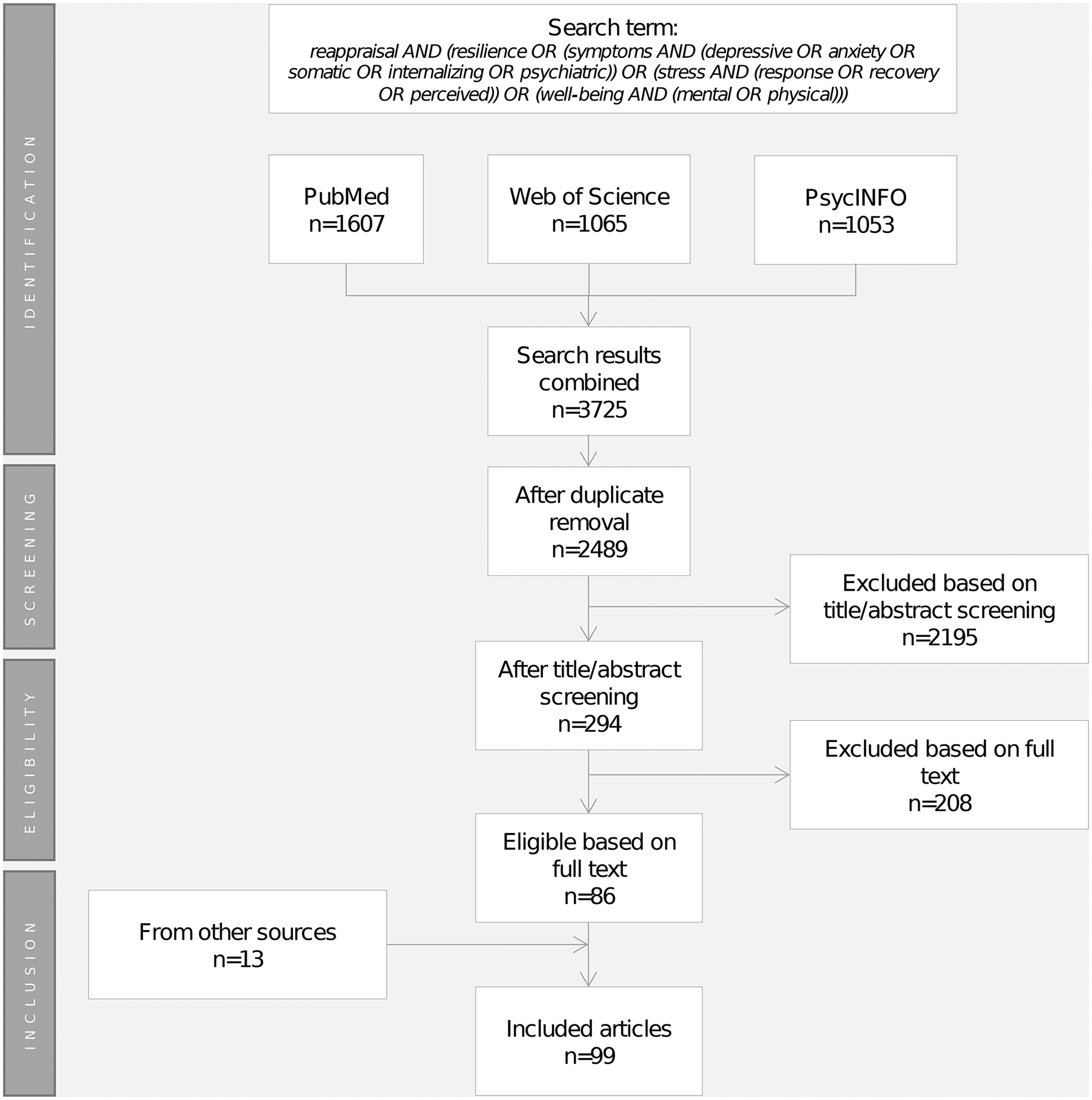
PRISMA diagram of the literature selection process.
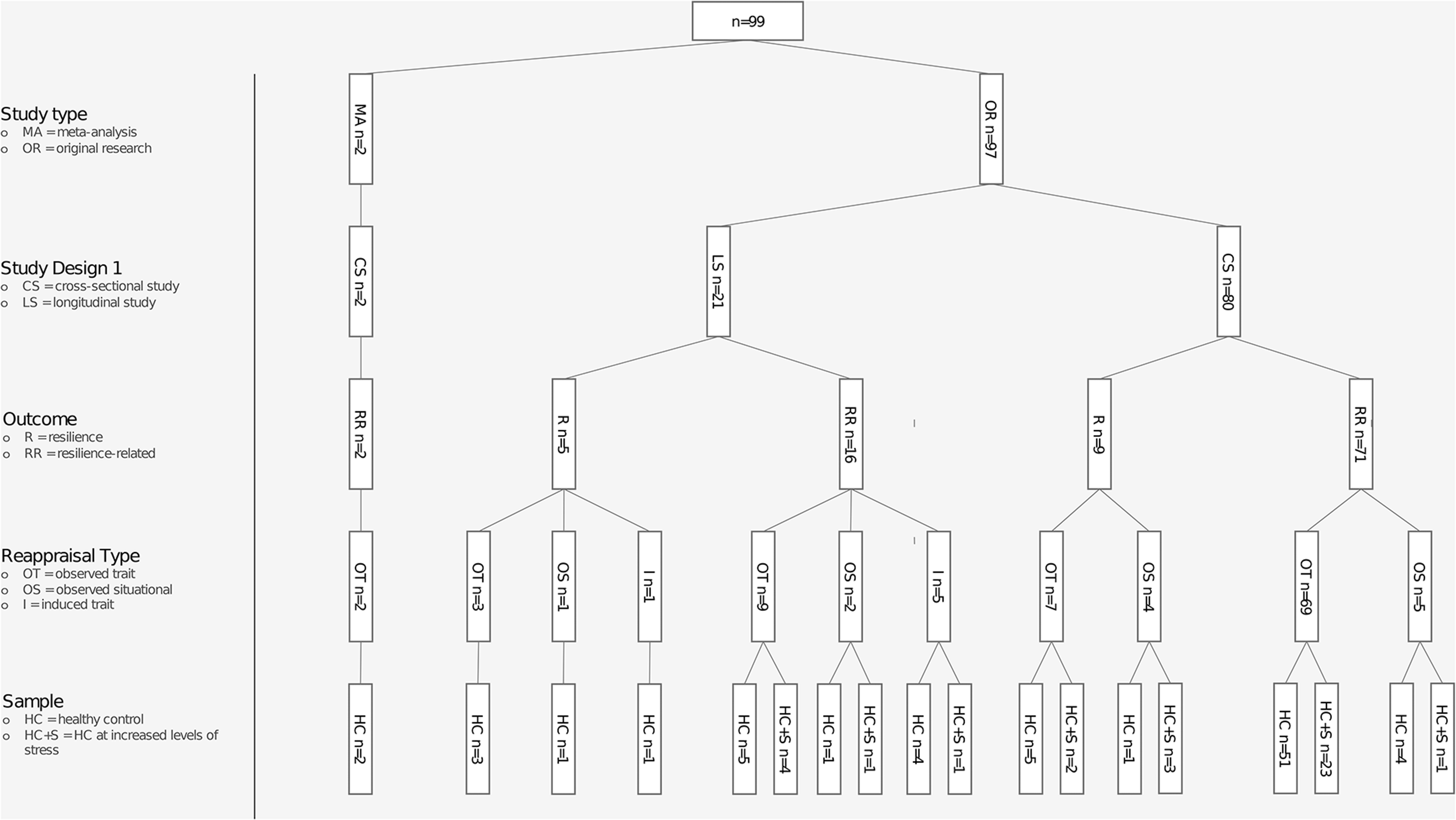
Categorization of studies included in this review. Note: For clarity, only nodes with n > 0 studies are shown. Some studies represented in one higher-level node fit the categories of more than one lower-level node and are thus mentioned at several instances.
Post-hoc meta-analyses were conducted wherever technically possible (k > 1 studies investigating the same effect size measure for the same outcome). Only cross-sectional studies reporting Pearson correlations met these criteria; meta-analyses were thus not conducted for longitudinal studies and moderation/mediation analyses.
Results
A considerable amount of literature exists on the relation - in real life - between PCR and resilience-related outcomes, that is, measures of mental health or well-being in the absence of information about stressor exposure. These studies are mostly cross-sectional studies (n = 80), investigating the association between observed trait PCR and experience of emotions, perceived stress levels, or psychiatric symptom severity, and mostly used regression models or correlation analyses. A smaller number of studies (n = 8) looked at mediation effects of observed trait PCR on the relation between other resilience factors and resilience-related outcomes. Finally, some longitudinal studies (n = 21) measured PCR and subsequently assessed the outcome variables at a later point in time, of which n = 6 studies also included interventions aimed at increasing PCR. These studies mostly did not consider stressor load, therefore not allowing to investigate whether PCR has a moderating role on the relationship between stressor exposure and the outcome variable. Four of the longitudinal studies (Ford et al., 2017; Ng & Diener, 2013; Russell & Anderson, 2019; Zahniser & Conley, 2018), however, also quantified stressor exposure in one or the other way and therefore can give particularly valuable insights on the relationship between PCR and actual resilience.
Cross-Sectional Studies (Observed PCR)
Given the small number of studies complying with a-priori stated quality criteria for resilience research, we included cross-sectional studies on the relationship between PCR and resilience-related outcomes. A relationship between PCR and resilience-related outcomes in cross-sectional studies is necessary (but not sufficient) for an existing relationship between PCR and actual resilience, which in turn would be necessary to support the PASTOR claim of PCR being a resilience factor (key question 1). At the same time, these cross-sectional studies cover an abundance of different specific resilience-related outcomes, ranging from different mood and well-being measures to psychiatric symptoms. They can thus provide additional insights into which outcomes are especially promising to investigate in proper resilience research when applying more rigorous study designs. The larger body of literature for cross-sectional studies moreover allowed us to conduct meta-analytical syntheses of effects.
Observed PCR and Mood/Well-Being
In association studies on trait PCR and different psychological or health variables, we can observe a clear picture regarding mood and well-being measures: In psychologically healthy adults, trait PCR is reported to be positively associated with questionnaire-assessed trait resilience (Hong et al., 2018; Karreman & Vingerhoets, 2012), positive affect (Andreotti et al., 2013; Balzarotti et al., 2016; Gross & John, 2003; Gunaydin et al., 2016; Hu et al., 2014; Johnson et al., 2016; Masumoto et al., 2016; Mauss et al., 2007; Nowlan et al., 2016; Richardson, 2017; Schanowitz & Nicassio, 2006; Schutte et al., 2009), optimism (Gross & John, 2003), well-being (Altena et al., 2018; Balzarotti et al., 2016; Costa et al., 2017; Freire et al., 2016; Gross & John, 2003; Karreman & Vingerhoets, 2012; LeBlanc et al., 2019; Mayordomo et al., 2016; McRae, Jacobs, et al., 2012; Ranney et al., 2017), self-esteem (Gross & John, 2003; Soto et al., 2012), self-acceptance (Schanowitz & Nicassio, 2006), life satisfaction (Aliche & Onyishi, 2019; Gross & John, 2003; Haverstock et al., 2020; Hu et al., 2014; LeBlanc et al., 2019; Schutte et al., 2009; Soto et al., 2012), self-efficacy (Hanley et al., 2015), autonomy (Schanowitz & Nicassio, 2006), emotional closeness and likability (Gross & John, 2003), positive relations with others (Schanowitz & Nicassio, 2006), as well as managing one's own emotions (Schutte et al., 2009). Likewise, mostly negative associations have been found with negative affect (Andreotti et al., 2013; Gross & John, 2003; Gunaydin et al., 2016; Hu et al., 2014; J. Johnson et al., 2016; Masumoto et al., 2016; Mauss et al., 2007; Pappaianni et al., 2020; Yeung & Wong, 2020), anger (Martin & Dahlen, 2005; Mauss et al., 2007), aggression (Juang et al., 2016), worry (LeBlanc et al., 2019), loneliness (Kearns & Creaven, 2017), perceived stress (Aliche & Onyishi, 2019; Ellis et al., 2019; Garland et al., 2011; Krafft et al., 2019; Martin & Dahlen, 2005; Memedovic et al., 2010; Miklosi et al., 2014; Perchtold et al., 2018; Powell, 2018; Sagui & Levens, 2016; Yeung & Wong, 2020), daily arousal (Meyer et al., 2012), as well as with affective responses to stressful events (J. Johnson et al., 2016). Only one study found no relations with questionnaire-assessed trait resilience (Mayordomo et al., 2016). Moreover, a handful of studies found no associations with positive affect (Pappaianni et al., 2020; Yeung & Wong, 2020), negative affect (Nowlan et al., 2016; Richardson, 2017), or the affective reactivity after experiencing a stressor (Richardson, 2017), or only found nonsignificant trends for affective reactivity after experiencing daily stress (Russell & Anderson, 2019), all however in the presence of associations with other resilience-related outcomes. Interestingly, using PCR in uncontrollable situations was found to be particularly associated with higher well-being, whereas using PCR in controllable situations even seems to be related to lower well-being (Haines et al., 2016; Troy et al., 2013). Likewise, while overall adaptive, frequent use of PCR was inversely related to satisfaction with life in individuals with a high oppressed minority identity (Perez & Soto, 2011). However, literature on this specific topic is sparse.
Relationships of PCR with well-being outcomes seem to be stronger in people who experienced adversity or report an increased exposure to stressors (Altena et al., 2018; Babore et al., 2019). Similarly, the relationship between childhood adversity and perceived stress in adulthood was weakest at high levels of PCR (Kalia & Knauft, 2020), indicating a buffering role on the relationship between stressor exposure and negative outcomes. Generally, in stressor-exposed samples, the same positive relationships with positive affect (Gillanders et al., 2008; Haverstock et al., 2020; Katana et al., 2019; Litzelman et al., 2017), well-being (Hopp et al., 2011; Katana et al., 2019), perceived quality of life (Li et al., 2015), sense of control (Haverstock et al., 2020), and questionnaire-assessed trait resilience (Baghjari et al., 2017), as well as negative relationships with negative affect (Gillanders et al., 2008; Haverstock et al., 2020; Karademas et al., 2018; Katana et al., 2019) and perceived stress (Haverstock et al., 2020; Katana et al., 2019) can be found.
Meta-analyses combining all positive mood and well-being outcomes (positive affect, questionnaire-assessed resilience, satisfaction with life, general well-being, personal growth, autonomy, self-acceptance, environmental mastery, positive relations with others, purpose in life, self-esteem) in one analysis revealed a medium association of r = .32 for the general population (k = 42; p < .0001; 95% CI [.29;.35]; I2 = 84%) and a trend association of r = .32 for individuals with increased stressor exposure (k = 5; p = .093; 95% CI [-.08;.73]; I2 = 97%; see Figure 4). Meta-analyses combining all negative mood and well-being outcomes (negative affect, perceived stress, distress) in one analysis revealed a small-to-medium association of r = -.22 for the general population (k = 14; p < .0001; 95% CI [-.30;-.15]; I2 = 68%) and for individuals with increased stressor exposure (k = 6; p = .0061; 95% CI [-.34;-.10]; I2 = 21%; see Figure 5). Details on the meta-analyses as well as analyses of individual (i.e., non-combined) well-being outcomes can be found in Supplement 2.
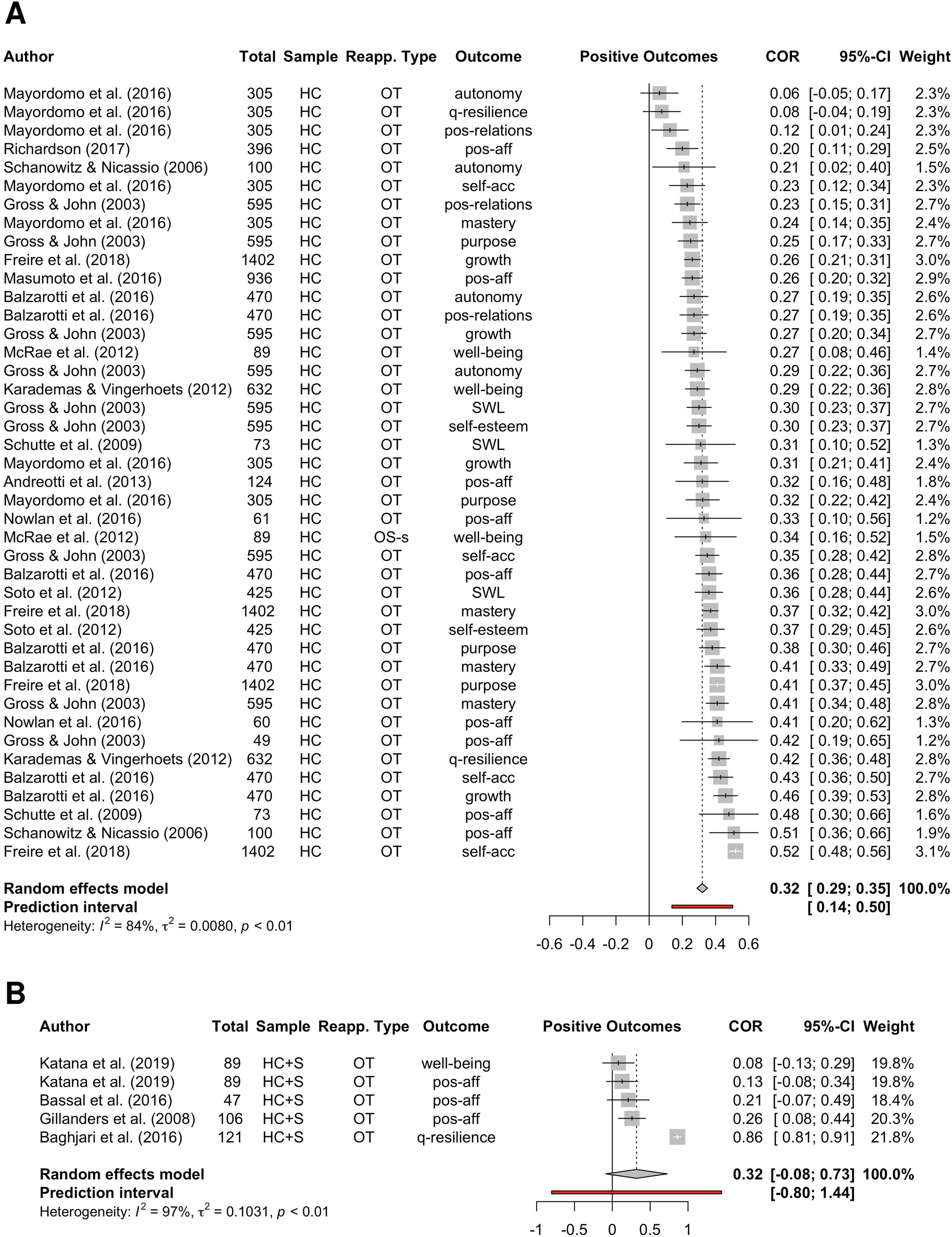
Results of meta-analyses including all studies on positive well-being outcomes in general healthy samples (HC; Panel A) and healthy samples with increased levels of stress (HC + S; Panel B). Note: OT = observed trait reappraisal, OS-s = observed situational reappraisal (reappraisal success), q-resilience = questionnaire resilience, pos-relations = positive relations, pos-aff = positive affect, self-acc = self-acceptance, SWL = satisfaction with life.
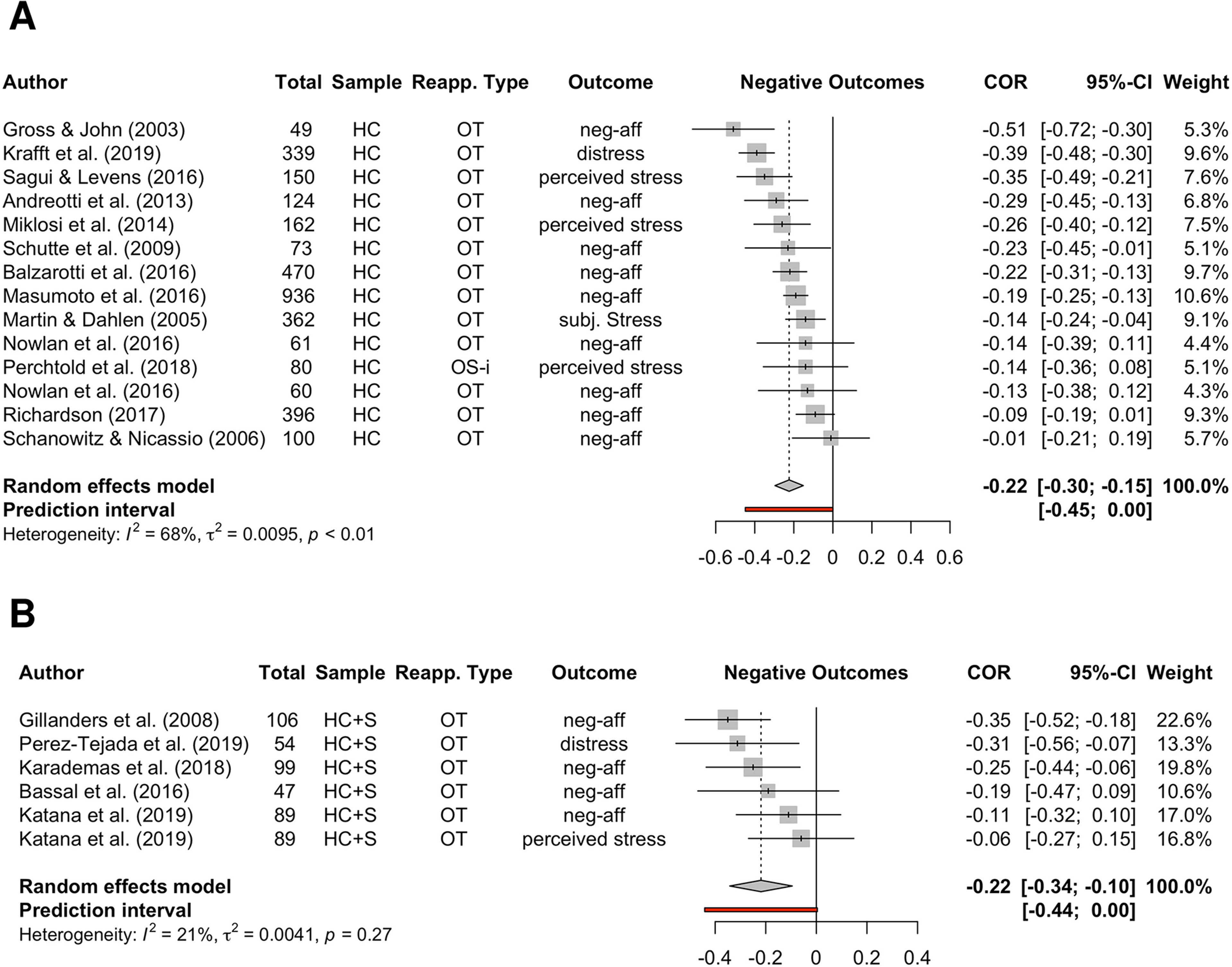
Results of meta-analyses including all studies on negative well-being outcomes in general healthy samples (HC; Panel A) and healthy samples with increased levels of stress (HC + S; Panel B). Note: OT = observed trait reappraisal, OS-i = observed situational reappraisal (reappraisal inventiveness), neg-aff = negative affect, subj. stress = subjective stress.
Observed PCR and Psychiatric Symptoms
Previous meta-analytic evidence mostly suggests that PCR is altogether negatively correlated with psychopathology to a small-to-medium extent (r = -.20; k = 48 studies; n = 21,150 participants; Hu et al., 2014), with one older meta-analysis reporting a small negative association with psychological health (r = -.1; k = 34 studies; n = 3,908 participants; Penley et al., 2002).
In healthy adults who experienced increased stressor load or traumatic experiences, research is mixed, with four studies suggesting lower depressive symptomatology at higher observed trait PCR (Garnefski & Kraaij, 2006a; Gillanders et al., 2008; Kraaij, Garnefski, et al., 2008; Mocan et al., 2018), and six studies not finding this relationship (Amstadter & Vernon, 2008; Cavanagh et al., 2014; Gärtner et al., 2019; Hopp et al., 2011; Kraaij, van der Veek, et al., 2008; Moore et al., 2008). Although overall related to lower depressive symptoms in an oppressed minority sample, frequent use of PCR was positively related to depressive symptoms in individuals who highly identified as belonging to an oppressed minority (Perez & Soto, 2011). Interestingly, in a study assessing both questionnaire PCR ( = observed trait PCR) and actual PCR success during an experimental task ( = observed situational PCR) in trauma-exposed participants, only PCR success was related to lower depressive symptoms (Cavanagh et al., 2014). Several studies by Troy and colleagues also measured PCR ability via task performance (i.e., the interindividual differences in successfully using PCR when instructed to do so) instead of a questionnaire measure of trait PCR. In all of these studies, a relation between observed situational PCR and lower depressive symptoms was found, especially at high levels of stress (Troy et al., 2010), in participants with low socioeconomic status (Troy et al., 2017), and when the experienced stressors are uncontrollable (Troy et al., 2013).
Our meta-analysis including only those samples with increased stressor load found a trend association of r = -.18 (k = 5; p = .0861; 95% CI [-.41;.04]), potentially due to the small number of studies and the high heterogeneity between studies (I2 = 91%; τ2 = .03; prediction interval [-.79; .43]). See Figure 6 for the results of both meta-analyses on depressive symptoms.
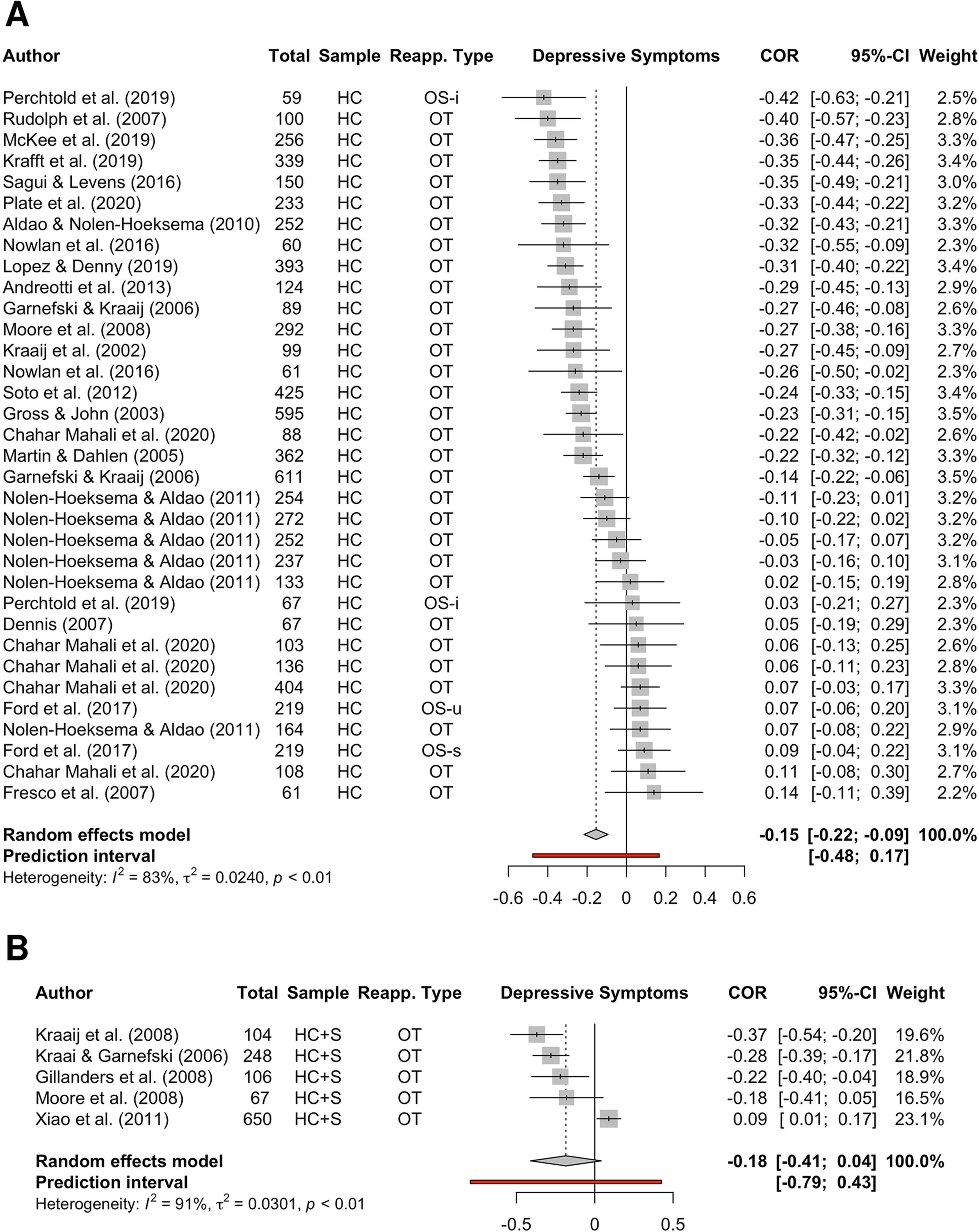
Results of meta-analyses including all studies on depressive symptoms in general healthy samples (HC; Panel A) and healthy samples with increased levels of stress (HC + S; Panel B). Note: OS-i = observed situational reappraisal (reappraisal inventiveness), OT = observed trait reappraisal, OS-u = observed situational reappraisal (reappraisal use), OS-s = observed situational reappraisal (reappraisal success).
In trauma-exposed participants, the scarce number of studies (n = 2) report mixed results with no associations in one (Amstadter & Vernon, 2008), and lower anxiety in another study (Johnson & Tottenham, 2015), though both studies rely on small sample sizes (n = 34 and n = 26, respectively). Studies investigating anxiety in physically ill and therefore by our definition stress-exposed participants found PCR to be related to lower anxiety symptoms (Gillanders et al., 2008) and lower pre-operative state anxiety (Aliche et al., 2020), or not to be associated with anxiety (Kraaij, van der Veek, et al., 2008). Our meta-analysis on anxiety in samples exposed to increased stressor load was based on three studies only and revealed an association of r = -.28 (k = 3; p = .0186; 95% CI [-.45;-.11]; I2 = 0%). Figure 7 reports the results of the meta-analyses conducted on anxiety outcomes for both sample groups.
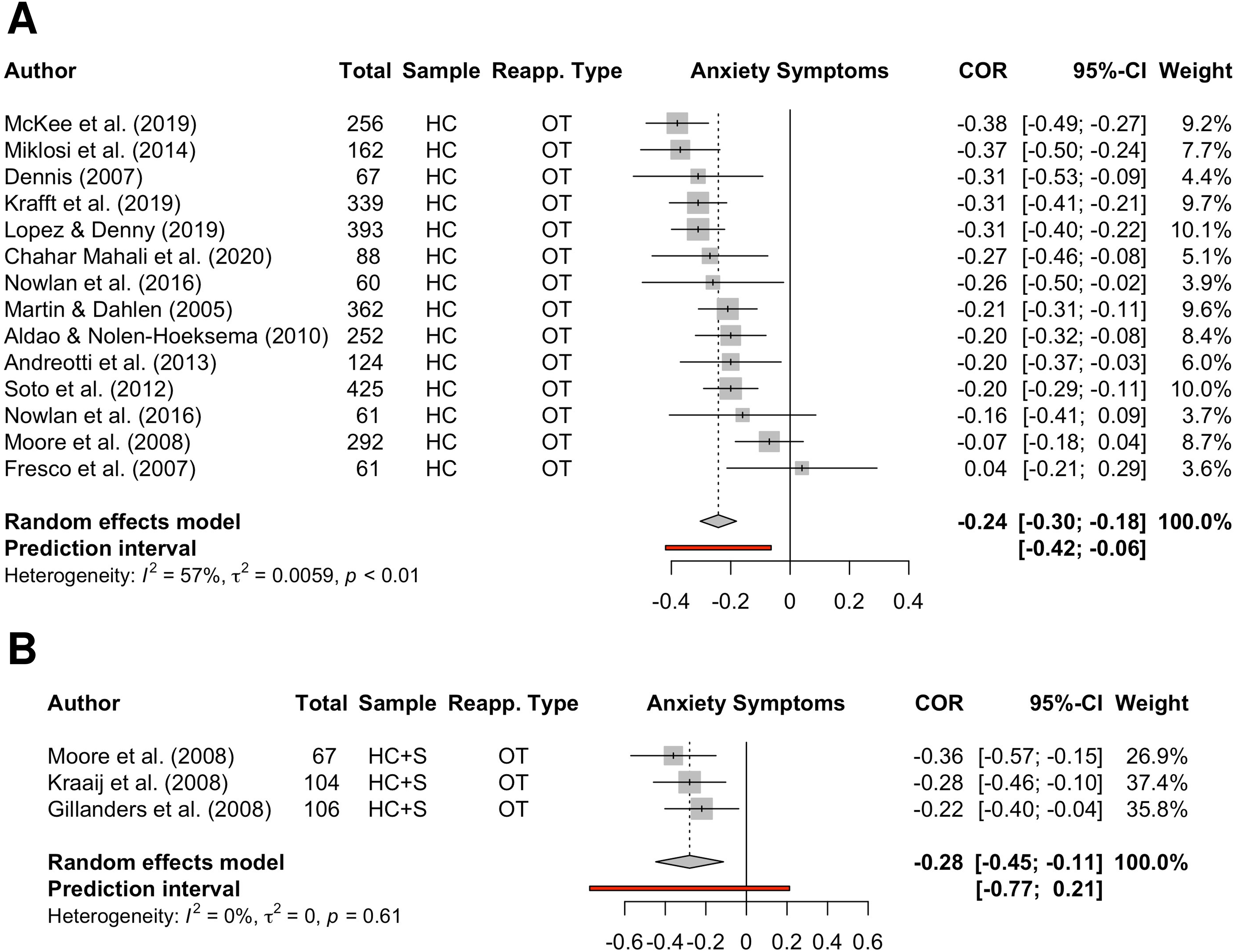
Results of meta-analyses including all studies on anxiety symptoms in general healthy samples (HC; Panel A) and healthy samples with increased levels of stress (HC + S; Panel B). Note: OT = observed trait reappraisal.
It is important to reiterate that all beforementioned studies were conducted in psychologically healthy adults. Therefore, clinical scores were all subthreshold and probably less variable than if the sample included, for instance, participants with continuous symptomatology scores ranging from minimal to severe.
Overall, PCR thus seems to be moderately related to a lower depressive and anxiety symptomatology in healthy adults and in healthy adults with experiences of adversity or higher stressor load.
Longitudinal Studies (Observed and Induced PCR)
Observed PCR in Longitudinal Studies
Overall, 9 studies investigated the relationship between baseline observed PCR and follow-up resilience (-related outcomes) using a longitudinal design. Although some of these found baseline trait PCR to predict future positive affect (Nowlan et al., 2016), and mental well-being (LeBlanc et al., 2019) or, inversely, depression (LeBlanc et al., 2019) and worry (LeBlanc et al., 2019), the majority of investigations found no prospective predictions of trait PCR for depression (Aldao & Nolen-Hoeksema, 2012; Krafft et al., 2019; Long & Hayes, 2014; Xiao et al., 2011), anxiety (Krafft et al., 2019), distress (Brewer et al., 2016; Krafft et al., 2019), or perceived quality of life (Long & Hayes, 2014).
However, when taking into account stressor exposure or experience of adversity, which is the gold standard for resilience research (see introduction), the picture is different: In a longitudinal investigation on more than 7000 randomly sampled participants across the USA, PCR did predict future decreases in anxiety levels, but only in participants with a low socio-economic status (SES), which often coincides with a higher exposure to adversity (Hittner et al., 2019). Specific stressors were, however, not quantified in this research, in which the level of adversity was inversely inferred from SES.
Some studies moreover used naturally occurring stressors to investigate changes in outcomes after a stressful period. Brewer and colleagues (2016) investigated college students’ PCR levels at the start of the first academic year, a period in life that is marked by many changes and can be considered to be a stressor for a relevant fraction of students. Baseline PCR predicted higher psychological well-being and lower levels of depression and anxiety at the end of the academic year, although only with small effect sizes (Cohen's f2 = .01). In a similar design examining a large sample (n = 1130) of first-year college students, Zahniser and Conley (2018) found that a higher increase in perceived stress from before the start of the first semester to the end of the first semester predicted higher levels of internalizing symptoms at the end of the first academic year. Perceived stress is not only a well-being outcome, but also a stressor on its own, which has the potential to induce mental health problems. Trait PCR moderated this relationship, such that in better reappraisers the increase in perceived stress on internalizing symptoms was only half as strong.
In addition, trait PCR was related to fewer depressive symptoms one month later in a large sample of n = 504 women who just received a diagnosis of breast cancer (Wang et al., 2014). Importantly, this study also suggests that although PCR by itself is predictive of a better mental health outcome, a combination of multiple emotion regulation strategies measured by the CERQ, involving PCR as well as refocusing and acceptance, is more predictive of a better outcome. A limitation of this study is that the baseline assessment was done after stressor onset (i.e., cancer diagnosis), making it impossible to disentangle pre-existing factors from reactions to the stressor that are related to a more resilient outcome.
Overall, the prospective results are mixed and do not offer a clear picture of a possible predictive nature. At increased levels of stressor exposure, however, this relationship is more apparent, indicating evidence for an attenuation of stressor effects on internalizing symptomatology. It has to be mentioned that these longitudinal studies mostly did not assess stressor load on an individual basis, but instead assumed similarity of stressful situations within the study sample (e.g., first year of college, cancer diagnosis) and the impact it overall has on participants. However, these results indicate that prospectively, PCR is especially predictive of resilience rather than of mental health or well-being in the absence of adversity. Together, the results thus give evidence for PCR being a resilience factor in accordance with PASTOR (key question 1).
Induced PCR in Longitudinal Studies
On top of the above-mentioned studies that investigated the possible predictive nature of observed PCR on mental health outcomes, there are studies that actively trained the use of PCR for several weeks (n = 2), or indirectly increased PCR levels by means of other trainings (n = 4), and subsequently investigated immediate or delayed effects on mental health.
Ng and Diener (2013) instructed participants to use reappraisal in their daily lives over the course of one week. They found that this instruction significantly reduced the experience of negative emotions in response to negative events during that week compared to a control instruction. A 10-day PCR training led to increases in trait PCR, which mediated increases in well-being and decreases in ill-being, as well as less negative emotional reactivity when reflecting on a stressful interpersonal situation that happened during the time of the training (Ranney et al., 2017).
There are more interventions that indirectly increased PCR levels via other trainings, which, in turn, mediated changes in outcomes: Directly after a three-week intervention of mutual social support via an online platform, people who engaged more in helping others to regulate their emotions had greater decreases of depression scores, which was mediated by an increase in PCR in these participants (Doré et al., 2017). Similarly, participating in an eight-week long mindfulness-based stress and pain management program led to reduced levels of perceived stress at the end of these eight weeks. Again, this relationship was mediated by increases in PCR (Garland et al., 2011). More delayed effects could also be observed: A five-week mantra meditation training led to immediate increases in PCR, which, in turn, mediated the relationship between the training and decreased anger 22 weeks post training (Bormann & Carrico, 2009). Finally, LeBlanc et al. (2019) found increases in PCR and satisfaction with life, as well as decreases in worry, anxiety, and stress after a 4-week general emotion regulation workshop. They did not, however, specifically investigate whether increases in PCR mediate changes in the other outcomes.
To conclude, the instructed use of PCR, and indirect increases in PCR following other interventions, were overall mostly related with favorable outcomes, indicating the potential of resilience interventions for increasing mental well-being. Trainings as short as one week have already proven some immediate effect, with slightly longer trainings showing even more prolonged results. Of importance for the question of whether PCR is related to resilience, we do see increases in PCR a) moderating the effects of stressors on emotional experience (Ng & Diener, 2013; Ranney et al., 2017), supporting the hypothesis of PCR being a resilience factor according to PASTOR (key question 1), and b) mediating the effect of different interventions on the assessed outcomes (Bormann & Carrico, 2009; Doré et al., 2017; Garland et al., 2011), indicating initial evidence for PCR being a more proximal resilience factor than other factors (key question 2).
Spotlight on Moderation and Mediation
The studies presented above indicate that whereas evidence for a direct relationship between PCR and resilience or resilience-related outcomes is mixed, successfully used PCR is especially helpful at high levels of stressor exposure, acting as a buffer against the detrimental effects of adversity. Moreover, moderating effects of PCR have been found on the relationship between daily stressors and negative mood (J. Johnson et al., 2016) and between adverse working conditions and psychological distress (Too & Butterworth, 2018). One study investigating a possible moderating role of PCR on the relationship between daily stressors and negative affect found no significant association, but a trend (Russell & Anderson, 2019). The literature thus indicates evidence for a role of PCR as a resilience factor as proposed by PASTOR (key question 1).
In addition, PCR acts as a mediator in the relation between different assumed resilience factors, such as mindfulness (Aliche & Onyishi, 2019; Desrosiers et al., 2013; McKee et al., 2019; Parmentier et al., 2019), secure attachment style (Karreman & Vingerhoets, 2012), perceived social support (Pejičić et al., 2018), as well as giving social support (Doré et al., 2017), and resilience-related outcomes. In contrast, PCR does not seem to mediate the relationship between stable risk factors such as neuroticism (Yoon et al., 2013) and resilience-related outcomes. Taken together, the results provide evidence that several resilience factors may impact resilience via PCR as a proximal resilience factor, in line with PASTOR (key question 2).
Discussion
The aim of the current review was to investigate scientific evidence substantiating the role of positive cognitive reappraisal (PCR) in resilience, as proposed by PASTOR theory. Next to giving an extensive overview on the literature of the field, our main goal was to answer whether PCR acts as a resilience factor, by moderating the relationship between stressor exposure and increased levels of psychological distress or mental health problems, and whether it is a proximal resilience factor that mediates the relationship between other resilience factors and resilience. To this end, we examined literature shedding light on the relationship between PCR and resilience as well as resilience-related outcomes in cross-sectional and longitudinal studies.
The existing literature suggests that PCR has a moderating role on the relationship between stressor exposure or other risk factors on the one hand, and psychopathology or other undesired outcomes on the other hand, indicating PCR is a resilience factor. Research moreover supports the idea of PCR mediating the beneficial effects of other resilience factors on resilience. Resilience factors whose relationship with resilience are mediated by PCR include mindfulness, secure attachment style as well as giving and perceiving social support. Future studies should systematically investigate a possible mediating role of PCR between a variety of resilience factors and resilience.
The emotion regulation strategy of PCR appears to be related to positive outcomes for many healthy participants and to play a protective role if applied successfully in the appropriate context (see Ford & Troy (2019) for an overview of factors behind unsuccessful and unfunctional reappraisal use). When facing stressful events, PCR can help to cope and maintain well-being and functioning. Specifically, several interventional studies showed increases in well-being to be mediated by increases in PCR. There is thus a potential for prevention, where at-risk states can be targeted before people have developed a psychiatric disorder. Implementing PCR trainings for participants at elevated levels of distress who do not fulfill the criteria of a mental disorder might be effective in preventing a transition into clinically relevant disease states (cf. Kalisch et al., 2019). In this context, it is also worth noting that studies comparing the use frequency of PCR relative to not regulating (e.g., Suri et al., 2015) or to other emotion regulation strategies such as social sharing, distraction, or expression (e.g., Bellingtier et al., 2022) usually find that PCR is used relatively infrequently. This indicates that efficient training strategies to raise the frequency or success of PCR can potentially achieve particularly large effects on resilience.
In individuals with high stressor load, the inverse relationship between PCR and depressive symptoms was most evident when investigating PCR ability, but less so when investigating questionnaire trait PCR (Cavanagh et al., 2014; Gärtner et al., 2019; Moore et al., 2008; Troy et al., 2010, 2013). These results indicate the possibility that questionnaire trait PCR is not a good measure of actual PCR use or ability in individuals with high stressor load or traumatic experiences. One explanation could be that questionnaire measures primarily assess conscious reappraisal mechanisms, whereas actual cognitive reappraisal ability as measured by a task can reflect a mixture of both conscious and unconscious mechanisms. Disentangling conscious and unconscious reappraisal mechanisms in individuals with high stressor load might thus be a promising avenue for future research.
According to PASTOR, reappraisal (conscious or unconscious) is only one of three overarching classes of neuro-cognitive processes whose effectiveness and efficiency shape a positive appraisal style, and positive cognitive (conscious) reappraisal is only one component of this class. Although focusing on the other two process classes – positive situation classification and interference inhibition – as well as on other reappraisal sub-processes – e.g., safety learning – is beyond the scope of this review, they should not be neglected when evaluating our results.
For example, the finding that the use of PCR at low levels of stress was related to higher rather than lower state anxiety (Moore et al., 2008) and that its use in controllable situations was related to lower rather than higher well-being (Haines et al., 2016) may surprise at first glance. A possible explanation for this pattern might be that, according to PASTOR, reappraisal should only be necessary for adaptive appraisal outcomes in situations that are aversive enough to initially trigger a stress response. Controllable or low-stress situations, however, may rather be ‘mildly aversive’ and thus do not necessitate a reappraisal in the first place, as these are effortlessly classified as non-threatening by individuals with a positive appraisal style. If an individual uses reappraisal nonetheless, they might thus be inaccurately classifying the only mildly aversive situation as negative enough to need a reappraisal, and thus be inefficient in the initial positive situation classification (PASTOR process class 1).
In one study, the combination of different presumably adaptive emotion regulation strategies, including PCR, refocusing (self-distraction), and acceptance, as assessed with the CERQ, explained more variance in the outcome measures than PCR alone, with acceptance and PCR showing the highest associations with the outcome (Wang et al., 2014). This can be partly explained by a terminological choice made by the authors of the CERQ, which strongly focuses on reappraisal as formulating expectancies of growth (see introduction), while excluding processes such as acceptance, or also putting into perspective (Garnefski & Kraaij, 2006b). By contrast, other widely used taxonomies, such as employed in the ERQ (see introduction), conceptualize PCR considerably more broadly as consisting of any cognitive change that improves situation appraisal. Within this umbrella category, they differentiate between reappraisal sub-types (as a function of the object of reappraisal; Webb et al., 2012) or tactics (as a function of semantic categories employed; McRae, Ciesielski, et al., 2012). These taxonomies explicitly include acceptance, but also putting into perspective or distancing in the cognitive reappraisal strategy family (see also Kalisch et al., 2005; Ochsner et al., 2004). Arguably, one can take a more positive view on a situation by abandoning a negative and judgmental primary appraisal in favor of a more accepting or distanced stance or by reminding oneself that things could be, or have been, much worse. PASTOR defines positive reappraisal similarly broadly as processes whereby negative appraisal become less negative or are complemented by alternative, positive appraisals (Kalisch et al., 2015) and therefore would assume other CERQ subscales, such as acceptance, to also inform about this process class. A methodological improvement in future investigations of a role for reappraisal in resilience would therefore be to be more inclusive in the choice of reappraisal measures. Nevertheless, the independent effect of a strategy (distraction) clearly not related to reappraisal in the Wang et al. study requires further corroboration and would - if confirmed and not explainable by mediation through PASTOR process classes - challenge the theory.
Overall, whereas there is a reasonably large body of literature investigating associations between PCR and measures related to psychological experience or mental health, studies fulfilling the recently postulated study design criteria for resilience research (Kalisch et al., 2015, 2017) are rare. Stressors are seldomly assessed systematically, but if they are, then mostly via self-reported impact/severity ratings. It can therefore not be ruled out that individual differences in PCR influence the severity ratings. This highlights the importance of a more objective assessment of stressors based on their occurrence instead of their impact or severity (as discussed in Chmitorz et al., 2020; Kalisch et al., 2021). Overall, there is a need especially for longitudinal studies that objectively and quantitatively assess stressor exposure between time points to get a more fine-grained understanding of the resilience process. Moreover, studies not only investigating reactivity to stressors, but also dynamics of recovery are needed to gain knowledge of how PCR is related to the exact processes underlying the stress response and the early recovery phase (Walter et al., 2015). Such research would best make use of standardized laboratory stress inductions. However, even though laboratory stressors have the benefit of enabling a comparable stressor exposure across participants, these may feel artificial, and a disconnect between laboratory-based (ability, success) and questionnaire-based (use, tendency) measures of PCR has been noted (McRae & Gross, 2020). Thus, although laboratory stressors allow us to gain insight into the temporal dynamics of the stress response and interindividual differences, evidence for their applicability to real-life resilience is to date scarce, which should be kept in mind when interpreting the results of stress induction studies.
Besides the above-mentioned methodological problems attached to the included studies, a further limitation of this review is that peer-reviewed articles in the English language were considered only. We were unable to adequately distill information from some articles that were, for instance, published in Chinese, which contributed to the fact that the majority of the included samples investigated PCR in European or North American populations. Since emotion regulation has culturally diverse aspects (Ford & Mauss, 2015), we can therefore only draw substantial conclusions for Western populations.
Altogether, with stress-related disorders being on the rise, it is important to find strategies that help preventing them. Besides having an association with a range of positive outcomes, this review found PCR to moderate the relationship between stressors and negative outcomes, thereby providing evidence for its proposed role as a resilience factor. PCR also mediated the effects of several other resilience factors on resilience, further supporting its important role. PCR thus does present as a viable candidate for prevention programs aimed at increasing well-being and decreasing symptomatology, particularly in at-risk individuals.
Supplemental Material
sj-docx-1-emr-10.1177_17540739221114642 - Supplemental material for Positive Cognitive Reappraisal in Stress Resilience, Mental Health, and Well-Being: A Comprehensive Systematic Review
Supplemental material, sj-docx-1-emr-10.1177_17540739221114642 for Positive Cognitive Reappraisal in Stress Resilience, Mental Health, and Well-Being: A Comprehensive Systematic Review by Antje Riepenhausen, Carolin Wackerhagen, Zala C. Reppmann, Hans-Christian Deter, Raffael Kalisch, Ilya M. Veer and Henrik Walter in Emotion Review
Footnotes
Acknowledgements
The authors thank Lasse Brandt for advice regarding meta-analyses. This project has received funding from the European Union's Horizon 2020 research and innovation programme under grant agreement No 777084 (DynaMORE project) and from the State of Rhineland-Palatinate (Stiftung Rheinland-Pfalz für Innovation, DRZ program).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. RK receives advisory honoraria from Joy Ventures, Herzlia, Israel.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Stiftung Rheinland-Pfalz für Innovation, Horizon 2020 Framework Programme, (grant number DRZ program, 777084).
Supplemental Material
Supplemental material for this article is available online.
Box 1.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.