
Abstract
Background:
It is crucial to timely recognize individuals presenting high-risk characteristics indicative of acute myocardial infarction.
Objectives:
Our study aimed to analyze the significance of evaluating ST-segment depression in patients with acute inferior myocardial infarction (MI). We assessed precordial ST-T changes as an indicator of ongoing ischemia, examined their correlation with the extent of coronary artery involvement, and potential association with both early and late cardiac outcomes.
Methods:
We enrolled 200 hospitalized patients with acute inferior MI who displayed ST depression in their precordial leads and underwent angiography. Individuals were divided into three groups based on the location of ST depression (V1–V3, V4–V6, and V1–V6). Demographic and echocardiographic data were extracted, and cardiac outcomes were assessed during hospitalization and follow-ups.
Results:
The findings revealed significant associations between ST depression in leads V1–V6 and V4–V6 with left ventricular systolic dysfunction, mitral regurgitation severity, and the extent of coronary artery stenosis in comparison with ST depression in V1–V3 (p < 0.05). Furthermore, a notable connection was found between the involved vessels and the degree of ST depression in precordial leads (p < 0.05). Moreover, individuals with prominent ST depression in V1–V6 and V1–V3 exhibited poorer outcomes (p < 0.05).
Conclusion:
Greater ST-segment depression in V1–V6 and V4–V6 in comparison with V1–V3 may signal multivessel disease, severe ischemia. Adverse outcomes like heart failure showed in V1–V6 especially V1–V3 versus V4–V6. This ST depression in acute inferior MI patients could indicate simultaneous ischemia or necrosis in other left ventricle regions, worsening cardiac function and prognosis. Thus, timely interventions are crucial.

Introduction
Acute inferior wall myocardial infarction (MI), a condition that occurs due to ischemia in the cardiac inferior region, constitutes approximately 40%–50% of all MIs. It is typically characterized by an elevation in the ST segment within the inferior electrocardiographic leads, accompanied by a concurrent depression in the ST segment within the precordial leads.1,2 The 12-lead electrocardiography (ECG) has proven to be an effective diagnostic tool for identifying and evaluating significant cardiac abnormalities in individuals presenting with angina. Timely diagnosis and precise evaluation of myocardial tissue damage are crucial for successful and effective reperfusion therapy in these cases. 3 ST-segment depression observed in the electrocardiograms of individuals suffering from MI, alongside ST-segment elevation in alternate leads, can suggest a reciprocal (mirror) alteration indicative of acute ischemia this change often results from the involvement of a non-infarcted vascular region located on the opposite side of the heart, a phenomenon commonly known as ischemia at a distance. Other causes of this change are taught to be infarct size, peri-infarction ischemia, an extension of infarction, concomitant left anterior descending coronary artery (LAD) or left circumflex artery (LCX) involvement, and collateral vessel stenosis. 4 The electrocardiographic pattern of mirrored ST-segment depression is a widely recognized indicator of ST-elevation MI. These changes are typically seen in opposing leads to those showing ST elevation, for instance, the anterior leads (V1–V4) compared to the inferior leads (II, III, and augmented (a)Voltage(V) of left Foot(F) (aVF)). 5 The leads opposite to the inferior leads are augmented (a)Voltage (V) of Left arm(L) (aVL) and I.
The prognosis and clinical outcomes related to acute MI in the inferior wall mainly depend on the involved coronary artery. 6 An estimated 80%–90% of patients demonstrate an affected right coronary artery (RCA). Notably, LCX involvement can result in electrocardiographic patterns resembling ST elevation in the inferior leads (II, III, and AVF). In addition to ST elevation in the inferior leads, a majority of patients represent reciprocal changes, such as ST depression in the aVL lead. 7 The significance and prognostic value of these reciprocal changes have been reported in prior research. Badiuzzaman et al.’s 4 study showed that acute inferior infarction with ST-segment depression in the anterior leads is associated with the involvement of the LAD, diminished ejection fraction (EF), and poor prognosis.4,8 Although the prognostic implications of evaluating ST depression in anterior leads are not fully understood, patients representing these characteristics are seen to experience a more extended MI. 9 Current studies seek to ascertain whether these depressions reflect additional cardiac vessel involvement, signifying ischemia in other myocardial territories, or are benign electrophysiological variations. Considering the importance of ST depression evaluation in acute inferior MI cases, our study aims to analyze and examine the extent of coronary artery involvement, as well as early and late cardiac outcomes in these patients. Early identification of at-risk patients through ECG—a noninvasive and widely accessible diagnostic tool—prior to invasive angiography may facilitate timely and appropriate intervention, potentially reducing short- and long-term morbidity and mortality.
Method
This research was a cross-sectional study conducted at the emergency department of the Dr. Heshmat Educational and Remedial Hospital, Rasht, Iran, targeting 200 individuals diagnosed with acute inferior MI displaying ST-segment depression in precordial leads on their ECGs between January 2016 and December 2017. We enrolled individuals who underwent angiography during their hospitalization while excluding those with a history of previous MI or revascularization, concomitant posterior or right ventricular MI, intraventricular conduction defect, valvular diseases, and specific cardiomyopathies (hypertrophic, restrictive, dilated), cases of mortality occurring before or during angiography, complications associated with angiography or angioplasty procedure, including infarction around angioplasty or angiography, and incidents of coronary dissection or perforation during angiography. Patients were categorized into three groups according to the presence of ST depression in leads V1–V3, V4–V6, and V1–V6.
The sample size was determined according to the number of involved coronary vessels and the methodology outlined by Badiuzzaman et al.

Given the calculations above, enrolling a minimum of 21 patients in each group was necessary to examine the involvement of 3 vessels and 10 individuals to evaluate each demographic variable.
Upon patient admission to the emergency department, qualified nursing staff conducted initial 12-lead ECGs at rest. The acute inferior MI diagnosis was determined by a board-certified cardiologist based on electrocardiographic findings and elevated cardiac enzymes. An expert interventional cardiologist then performed advanced coronary angiography through either the femoral or radial artery, with imaging recorded by Siemens angiographic equipment in multiple projections of both right and left coronary arteries. Subsequently, angiographic images were evaluated by two cardiologists blinded to the patient’s clinical information, who resolved any disagreements through review, discussion, or consultation with a third cardiologist.
The SYNTAX score (SS) was utilized to evaluate the severity of coronary artery involvement, grading stenosis severity, and predict outcomes for individuals eligible for revascularization, specifically percutaneous coronary intervention (PCI). This scoring system assesses 11 angiographic variables to classify patients with complex coronary artery disease for treatment with PCI, medical therapy, or coronary artery bypass grafting. It categorizes severity as low risk (SS ⩽ 22), intermediate risk (23 ⩽ SS ⩽ 32), and high risk (SS ⩾ 33).
Demographic variables were recorded, including age, gender, history of systemic hypertension, smoking, and diabetes, and diastolic and systolic blood pressure was measured. Laboratory results were also analyzed, including complete blood count, creatine kinase-myoglobin binding, cardiac troponin 1, triglyceride (TG), high-density lipoprotein (HDL), low-density lipoprotein (LDL) cholesterol, creatinine, blood urea nitrogen, and bleeding time. Fasting blood sugar, blood lipids, and creatinine (Cr) were evaluated within 24 h of hospitalization in the emergency or coronary care unit. All patients underwent ECG and echocardiography on discharge, and any vascular incidents were documented. All patients received appropriate diagnostic and therapeutic interventions as necessary. A follow-up session was scheduled according to the pre-determined program during the patient’s discharge, and a cardiologist visited all patients 1 week and 1 month post-discharge.
The study analyzed the correlation between ST depression and the severity of coronary artery involvement in three groups (V1–V3, V4–V6, and V1–V6), assessing cardiac outcomes including congestive heart failure, cardiogenic shock, second- and third-degree heart blocks, tachycardias, fibrillation, re-infarction, revascularization procedures, and cerebrovascular accidents. Cardiac re-infarction was defined as the presence of clinical symptoms such as chest pain, coupled with elevated cardiac enzymes and new ST elevation following the primary PCI, necessitating angiography and revascularization. Cerebrovascular accidents were diagnosed based on symptoms, neurologist’s diagnosis, and CT scan evidence. Cases of congestive heart failure and cardiogenic shock were identified based on recorded clinical symptoms. Other complications, such as heart block, ventricular tachycardia, and fibrillation, were diagnosed based on ECG findings.
The statistical evaluation was performed using IBM SPSS Statistics software version 24 (IBM Corp., Armonk, NY, USA). Descriptive statistics, including frequency, percentage, mean, and standard deviation (SD), were utilized to characterize the acquired data. The normality of the data distribution was analyzed using the Shapiro–Wilk test and the Kolmogorov–Smirnov test. In addition, Levene’s test was applied to assess the homogeneity of variance across groups. Comparative analyses were conducted by applying T-tests, chi-square tests, Mann–Whitney U tests, and Kruskal–Wallis tests. Statistical significance was demonstrated by a p value of less than 0.05 (p < 0.05).
Results
In the present study involving 200 participants who met the inclusion criteria, the average age was calculated to be 61.5 ± 12.5 years. The age range spanned from 15 to 88 years. Based on the SYNTAX score, data analysis indicated that 132 individuals exhibited low-risk coronary artery stenosis (accounting for 66.0%), 62 presented with intermediate-risk stenosis (31.0%), and a minority of 6 patients (3.0%) demonstrated high-risk stenosis. Due to the limited number of cases in the high-risk group, it has been merged with the intermediate group. Table 1 outlines the distribution of severity of coronary artery stenosis in acute inferior MI concerning patient demographics in which no significant correlations were observed between the stenosis severity and demographic, clinical, laboratory, and echocardiographic variables (p > 0.05). Exceptions were noted with diastolic blood pressure, hemoglobin levels, and mitral regurgitation (MR) severity, which displayed significant correlations (p < 0.05). Patients with severe MR exhibited a high risk of coronary artery disease based on SYNTAX score compared to those with moderate and mild regurgitation.
The relationship between demographic, clinical, laboratory, and echocardiography variables with the severity of coronary artery stenosis.

Numerical variable: mean ± SD or median (IQR); categorical variable: N (%).
Independent t-test.
Pearson chi-square.
Mann–Whitney test.
BS, blood sugar; CAS, coronary artery stenosis; Chol, cholesterol; Cr, creatinine; DBP, diastolic blood pressure; G1, low risk; G2, intermediate and high risk; Hb, hemoglobin; HDL, high-density lipoprotein; LDL, low-density lipoprotein; MR, mitral regurgitation; Neut, neutrophil; SBP, systolic blood pressure; TG, triglyceride; WBC, white blood cell.
No statistically significant correlations were observed between the precordial lead groups and hypertension, and smoking (p value > 0.05). Nevertheless, a notable relationship was seen between all three groups and the echocardiographic results. EF created a significant separation in data as normal EF corresponded with a trend toward lower ST-segment depressions, which significantly increased with worsening systolic dysfunction, particularly with severe systolic dysfunction showing markedly elevated ST-segment depression in all leads (p values: V1–V6 = 0.018, V1–V3 = 0.035, V4–V6 = 0.047). Patients with mild MR showed lower ST-segment depressions than those with moderate or severe MR. Table 2 also delineated a progression in ST depression across various degrees of coronary artery stenosis severity in all three groups (p < 0.05).
The mean ST depression in precordial leads in patients with acute inferior infarction according to demographic, clinical, and laboratory results.

Numerical variable: median (IQR).
Mann–Whitney test.
Kruskal–Wallis H.
CAS, coronary artery stenosis; MR, mitral regurgitation.
As indicated in Table 3, a statistically meaningful correlation was found between the type of affected vessel and the ST depression exhibited in precordial leads. Data highlighted how individual coronary artery involvement impacts ST-segment depression. The co-involvement of the LAD with either the LCX or RCA was associated with increased ST-segment depression, indicating a progression toward the involvement of all three coronary vessels.
The mean ST depression in precordial leads in patients with acute inferior infarction according to the involved vessel.
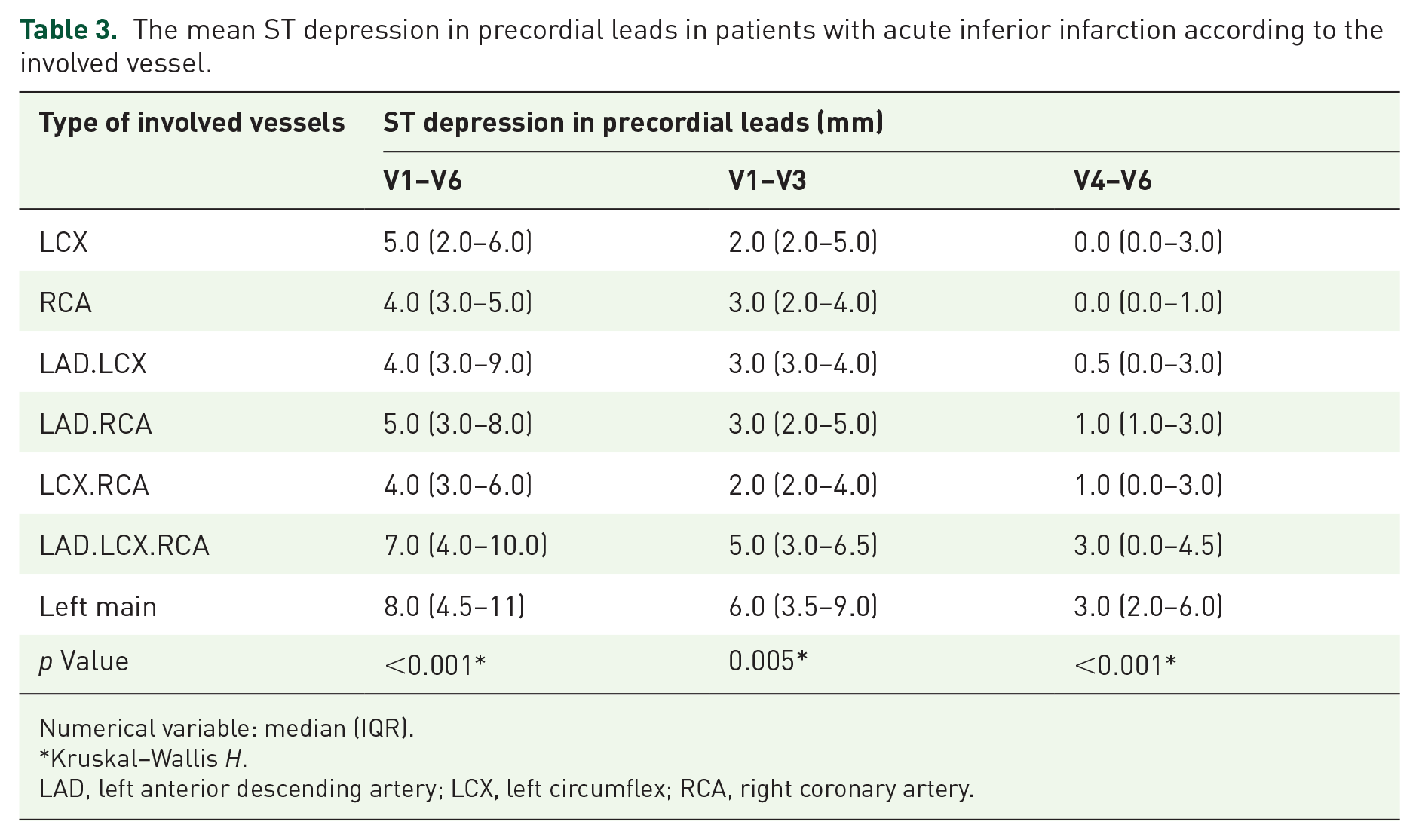
Numerical variable: median (IQR).
Kruskal–Wallis H.
LAD, left anterior descending artery; LCX, left circumflex; RCA, right coronary artery.
Table 4 demonstrates the relation of ST-segment depression in precordial leads and future cardiac outcomes such as re-infarction, hospitalization, cerebrovascular accident, arrhythmia, and heart failure. Notably, patients with cardiac outcomes exhibited statistically significant greater ST-segment depression in V1–V6 and V1–V3 leads (p = 0.012 and p = 0.003, respectively).
The mean ST depression in precordial leads in patients with acute inferior infarction according to cardiac outcomes.
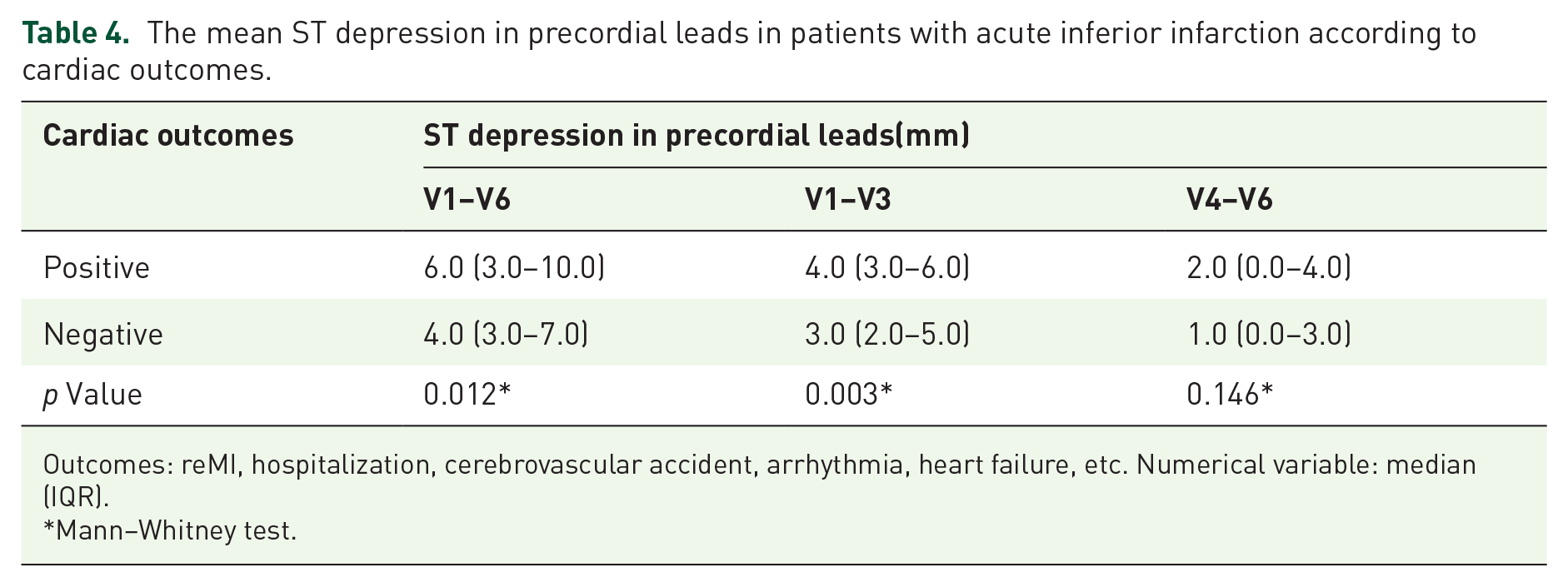
Outcomes: reMI, hospitalization, cerebrovascular accident, arrhythmia, heart failure, etc. Numerical variable: median (IQR).
Mann–Whitney test.
Discussion
The most promising finding in our study was the link between the extent of ST depression and the number of involved vessels in three specific groups (V1–V3, V4–V6, and V1–V6). Our results indicated a significant direct relationship between mean ST depression in all three groups and the number of involved vessels. Furthermore, we unveiled a relationship between the extent of ST-segment depression and the severity of involvement in each vessel. Specifically, we found that the combination of LAD, LCX, and RCA with RCA and LCX had statistically significant differences in V1–V6 and V1–V3, with the mean of ST depression in LAD, LCX, and RCA being consistently higher. In the V4–V6 group, the only observed difference was between LAD, LCX, and RCA and RCA, with the mean of ST depression in these three coronary arteries involvement also higher, highlighting a more prominent association between ST depression and LAD involvement. In a study conducted by Nour, the results demonstrated a notable association between ST depression in precordial leads and the presence of multivessel disease. 10 Similarly, Parale et al. found that ST depression equal to or greater than the ST elevation in leads I, aVL, and V4–V6 was linked to multivessel disease. 11 However, in these two studies, Ruiz-Mateos and Edmunds et al. 12 indicated that in individuals with inferior MI, ST-segment analysis was not predictive of multivessel disease but showed the percentage of myocardium at risk was significantly greater (23% vs 15%) in patients with ST depression. El Atroush et al.’s investigation revealed a statistically meaningful association between ST depression and LAD vessel lesions. 13 Savonitto et al. discovered a noteworthy association between the extent of ST-segment depression in V4–V6 and V1–V3 leads with both the level of left main artery involvement and the presence of multivessel disease. 14
Also, our study showed a noteworthy association between MR and the severity of coronary artery stenosis given the SYNTAX score; the severity of stenosis was elevated with increased levels of mitral insufficiency. He et al. conducted a study assessing the prognostic value of the clinical SYNTAX score in acute coronary syndrome patients undergoing PCI. The study revealed no notable association between uric acid, cholesterol, LDL, HDL, and TG levels and the severity of SYNTAX. However, factors such as age, gender, and a history of stroke, particularly cerebrovascular accidents, showed a significant correlation with SYNTAX severity. In addition, a history of cerebrovascular accidents was more prevalent in patients with severe SYNTAX compared to those with moderate or mild SYNTAX. Diabetes, however, did not show a meaningful relationship with the SYNTAX score. 15 This was in line with the findings of Namdar et al., which indicated a considerable association between SYNTAX score and ST-segment depression. They also found that 62.9% of patients without ST-segment depression and 69.8% with ST-segment depression had multivessel involvement. 16
In the present study, we found no discernible association between ST depression and a history of heart disease, smoking, or high blood pressure. Patients with diabetes demonstrated a statistically lower mean ST-segment depression. Similarly, the findings of Nour were in line with ours, indicating that factors such as gender, diabetic status, hypertension, familial history, dyslipidemia, smoking habit, and history of cerebrovascular accidents did not display a significant association with ST-segment depression presence or absence. 10 Furthermore, in 2012, El Atroush et al. observed no statistically significant associations between age, sex, diabetes, hypertension, smoking, dyslipidemia, or a history of heart disease in the patients or their families and the existence or absence of ST depression. 13 Çelik et al. similarly found no statistically significant correlation between the presence or absence of precordial changes and factors such as age, sex, hypertension, diabetes, dyslipidemia, and smoking. 17 Their findings align with those reported by Zoghi et al. 18
We also analyzed the incidence of heart failure and cardiac outcomes among patients exhibiting various degrees of ST-segment depression. Our findings established a correlation between the extent of ST-segment depression in each group and the occurrence of heart failure, mitral valve insufficiency, and other cardiovascular events. The findings suggest that prominent ST depression in precordial leads correlates strongly with both left ventricular systolic dysfunction and the severity of MR, which are indicative of more extensive ischemia and poorer outcomes. We acknowledge the relevance of the aforementioned distinction between occlusive and nonocclusive ischemia as it pertains to ST-segment depression. Furthermore, our results indicate that patients with ST depression in specific lead combinations (such as V1–V6 and V1–V3) experience more severe cardiac consequences, aligning with literature suggesting that maximal ST depression in V1–V4 is particularly suggestive of acute coronary occlusion. 19 A study by El Atroush et al. compared two groups based on the presence of at least 1 mm of ST-segment depression in specific leads, revealing that a larger proportion of patients in the first group experienced cardiovascular events compared to the second group, indicating a significant association with the degree of ST depression. 13 Also, Shah showed that inferior AMI patients with reciprocal ST depression in V1–V4 had larger infarcts, more extensive Wall Motion Abnormality (WMA’s), lower EF’s, and worse hemodynamics than inferior Acute Myocardial Infarction (AMI) patients without precordial reciprocal ST depression. 20 However, a study by Çelik et al. focusing on acute inferior infarction did not find a substantial link between ST depression and echocardiographic parameters, specifically Left Ventricle (LV) function. 17 Similarly, Nour demonstrated that the existence or absence of ST depression changes in precordial leads was not significantly related to the rate of severe systolic heart failure. 10
The findings indicate that the relationship between ST depression changes and coronary artery involvement could assist clinicians in accelerating angiography for inferior MI affecting smaller territories, potentially reducing revascularization delays.
Limitations
A key limitation of our study is the absence of a control group. We could include a control group of patients with acute inferior MI without precordial ST depression to provide a comprehensive comparison and bolster the conclusions regarding the prognostic value of ST-segment changes, which reduces the generalizability of our results. In addition, the study did not address long-term follow-up or the correlation between ST-segment depression and elevation, suggesting a need for more extensive, long-term studies focusing on the relationship between SYNTAX score and ST-segment depression and elevation.
Conclusion
Acute inferior MI seems to have a better prognosis than anterior MI. Patients with acute inferior MI are usually at lower risk of in-hospital and long-term mortality. However, some subgroups of this type of MI conducted in our study appear to be high risk, have poor prognosis, and need urgent revascularization. The findings suggest that greater ST depression in precordial leads V1–V6 and V1–V3 may indicate multivessel disease and severity of ischemia, as well as adverse cardiac outcomes like heart failure and left ventricular dysfunction. The presence of coronary artery stenosis in patients with acute inferior MI displaying ST-segment depression in the precordial leads may indicate the presence of simultaneous ischemic or necrotic incidents in other regions of the left ventricle myocardium. These incidents could contribute to the deterioration of cardiac function, potentially leading to severe heart failure and a poor prognosis. Consequently, implementing timely and prompt interventions is recommended in these cases.