
Abstract
Background and objectives:
California is one of a few states with mandatory reporting of mortality after coronary artery bypass graft (CABG) surgery. The Affordable Care Act restructured Medicaid, preferentially penalizing patients experiencing poverty because payments to hospitals for isolated surgical events overshadow payments to primary care clinicians. We propose outcomes are superior when hospital networks organize surgical episodes within the context of primary care inside that same network.
Design and methods:
We listed factors impacting outcomes after CABG. CABG surgery outcome depends upon the integration of issues beginning years preoperatively and extending for decades. Therefore, we studied one health maintenance organization (HMO) from 2009 to 2020 compared to surrounding individual hospitals. We divided 58 hospitals in Northern California in 2009 according to income and population. To focus on changes introduced because of COVID-19, we compared a public database for the subset in 2009 for any relationship between poverty in a zip code and low volumes of CABG in that area to overall mortality in 2020. First, we defined low-income zip codes as those with a higher rate of poverty than the state average or with a lower per capita average income, per Census Bureau. Second, low volume was defined as a population under 165,000 because a hospital adjacent to a larger community can easily transfer care, sharing surgeons and processes. Third, we defined low volume as fewer than 180 CABG per year.
Results:
Our qualitative evidence synthesis reveals that informal communication and hospital HMO policies improve CABG outcomes. In our small pilot data, Chi-square analysis showed higher crude mortality rates in 1507 CABG in 17 low-income low-volume hospitals versus 8163 CABG in the other 41 Northern California hospitals (2.72% vs 1.69%, p = 0.0064). Low-income low-volume hospitals had a relative mortality risk of 1.61 (95% CI: 1.14–2.27). These hospitals had a mean mortality rate of 3.79%, readmission 11.12%, and stroke 1.84%. A patient undergoing CABG in a low-income low-volume hospital has a 61% higher chance of dying. The number needed to treat analysis shows that one life can potentially be saved for every 97 patients referred to another institution.
Conclusion:
We describe features of an HMO that contribute to up to fourfold lower mortality rates.
Keywords
Introduction
High surgical volume
Mortality rates 30 days after coronary artery bypass graft (CABG) surgery are inversely correlated to hospital volume.1–3 When the public gained access to individual hospital and surgeon-specific outcome data in California in 2001, referral patterns changed to improve such de facto advertisements, evidenced by vast improvements in mortality in the first few years of the reporting program. The California Health and Human Services Agency collects the data as a public service to improve transparency. OpenGov is a separate entity that manages the website, and the data are not intended to guarantee any particular outcomes. Also, methods of collection could vary, introducing bias at multiple levels.
We were surprised to find one outlier in 2009, Kaiser Permanente, with a fourfold lower CABG mortality than the state’s average. At Kaiser Permanente Medical Center in San Francisco, the mortality rate was 0.53%, the readmission rate was 8.84%, and stroke incidence was 1.22%. These benchmarks compare favorably to the overall California CABG mortality rate of 1.9%, readmission rate of 13.24%, and stroke incidence of 1.4% reported in 2009.
Kaiser Permanente is a large non-profit health maintenance organization (HMO) in the Western United States. In California, Kaiser provides care to about one-fourth of the insured population. 4 We examined only this HMO because it is the predominant one in the state. The medical group of physicians is for-profit, with a competitive selection process and management in a small setting at each building. Kaiser Hospitals in California are organized into either the Northern or Southern corporations. Insured members may only be admitted to Kaiser Hospital and Clinic buildings, while non-Kaiser members are not allowed, which is unique among insurance providers. The volume of cardiac surgery is regionalized in a way seldom seen in America. For example, at the Kaiser San Francisco building, over 2000 CABG, an unusually high annual volume, were performed in the late 1990s when the volumes were under 200 in most of the other 120 programs in California. Due to physical plant constraints, about half of these CABG operations moved about an hour south; therefore, San Francisco volumes do not now look as impressive as in 2009. The appeal of a regionalized high-volume center is improved coordination before high-risk procedures and increased access to appropriate follow-up.
By contrast, outcomes are predicted to be worse in smaller centers. Additional costs for staffing standby surgeons, anesthesiologists, perfusionists, and equipment with short shelf-life can surpass a million dollars even for a hospital only performing approximately two dozen CABG annually.5,6 In the last couple of years, California law expanded percutaneous coronary intervention (PCI) beyond the 120 hospitals providing rescue CABG to include 21 additional hospitals, 8 of which are Kaiser. Of note, when the Affordable Care Act (ACA) favored reimbursements for PCI, mortality for PCI by 2007 began to surpass that of CABG. An increased use of PCI corresponds to those same patients not having a CABG. Potentially, PCI mortality increased because the public had no access to mortality data until California law required reporting around 2016. In 2020, out of 48,904 PCI performed, 1245 died within 30 days, a rate mirroring CABG. Long-term mortality is largely undescribed in the post-pandemic environment, where patients experiencing poverty have even less access to primary care. After usually 1 year of dual antiplatelet prescriptions, non-compliance may result in in-stent thrombosis, while severe bleeding may occur with too high a dose. Similarly, non-compliance with congestive heart failure or diabetic medications after CABG would be expected to result in increased long-term mortality at small centers without a network of primary care physicians following these individuals.
The COVID-19 pandemic of 2020 brought a lower life expectancy. One contributing factor may be the decreased use of preventive medicine. For example, access to cardiac catheterization labs was 30% lower, as measured in coronary catheterizations per month nationally. This example of delayed care was associated with a decline in the volume of CABG in California to 10,949 and a rise in risk-adjusted mortality to 2.64%, compared to 13,049 at 2.2% in 2017 and 13,260 at 1.9% in 2009.
Low-income zip codes with low surgical volume
An unintended consequence of the ongoing restructuring of Medicare payments is the punishment of safety-net hospitals.7,8 Mortality and morbidity rates for adults undergoing CABG at high-volume regionalized hospitals are lower compared to rates for those undergoing the same surgery in rural hospitals located in communities in poverty.1,2,9 Because low-income zip codes in recent years are concentrated in rural America, Kaiser can alleviate the problem by transporting rural patients to their regionalized building that contains high volumes. About 60% of Medicare beneficiaries in the United States live in counties with low socioeconomic status (SES).3,10 Non-Hispanic Whites fall into the highest SES category half the time, while Blacks fall into the lowest 80% of the time, corresponding to Medicare rates of 70% for Whites and 55% for Blacks and Medicaid rates of 4% for Whites versus 12% for Blacks. 11
Massachusetts compared PCI and CABG before and after healthcare reform. PCI was offered more often than CABG to Blacks and Hispanics than Whites and Asians, especially before reform. 12 Similarly, patients in communities with a high level of college graduates, men, and patients with private insurance were more likely to be offered CABG than PCI, both before and after reform. After reform, in-hospital mortality was worse in communities with less educated populations. 13 In New York between 1993 and 1996, among over 58,000 patients undergoing CABG, uninsured patients were more likely to receive care at a high-mortality center. 14 These investigators found a significant association between types of insurance coverage and higher readmission rates: Medicare 15% versus Medicaid 19% versus private insurance 9.7%. Furthermore, patients from zip codes with a median household income under $43,000 had a nearly 15% risk of readmission, compared with 12% for patients from a higher income household.
Therefore, we hypothesized that low-volume hospitals in low-income Northern California communities fare worse. To test this hypothesis, we collected pilot data from CABG mortality rates in 2009, 2017, and lastly in 2020 in an attempt to explain if results could be sustained over time at San Francisco Kaiser. Kaiser is unique because primary care is capitated in a closed system funded by members only for the 20% of costs remaining after 80% of payments by Medicare. Mortality at 30 days postoperatively in Kaiser San Francisco began at 0.5% but rose to 3% of 384 patients in 2017, falling again to 1.95% of 363 patients in 2020. Meanwhile, mortality rates were better preserved at Kaiser Los Angeles in 2017 at 2% of 688 and in 2020 at 0.61% of 600 CABG.
Comprehensive healthcare network
Not much data has been released after the COVID-19 pandemic, but delayed care would be expected to result in worse outcomes for several more years. We propose that the etiology of the original advantage is comprehensive coordinated care. Inherent in the HMO structure is both formal, that is, top-down, and informal, that is, relationships between different specialists within a hospital system. 15 If high informal communication is present, the American hospitals performing a quarter of a million CABG might save $640 million annually. 15 Informal communications lead to fewer readmissions and 13% less need for payment. 15
Reasons for failure
We hypothesize the HMO advantage was lost because of factors such as obesity, COVID-19, opiate addiction, depression, and homelessness, at a macroeconomic level. At the microeconomic level, a series of hospital consolidations into larger corporations forced rules of management that disengaged participating clinicians and patients. Approximately one-third of elective surgeries and primary care clinic visits were canceled during portions of the pandemic, along with falling reimbursements causing small hospital systems to close their doors. Factors implicated in hospital closures include low volumes and poor outcomes in highly reimbursed procedures, such as CABG.16,17 This environment created fragmented care, even within an HMO.
Methods
We conducted a PubMed search using the keywords CABG, outcomes, HMO, and poverty. To focus on changes introduced because of COVID-19, we compared a public database for the subset in 2009 for any relationship between poverty in a zip code and low volumes of CABG in that area to overall mortality in 2020. We analyzed administrative data available to the public on the Internet from the California CABG Outcomes Reporting Program (CCORP from the Office of Statewide Health Planning and Development). It is one of at least six states mandated to report outcomes data. We selected the 58 hospitals north of Los Angeles (and two related hospitals in San Diego County) performing CABG in 2009. 1 We included the low-income low-volume group hospitals that met three criteria. First, we defined low-income communities as those zip codes with a higher rate of poverty than the state average or with lower per capita average income per Census Bureau data. Second, low volume was defined as a population under 165,000 because a hospital adjacent to a larger community can easily transfer care. Surgeons are often on staff at nearby hospitals and share processes during perioperative care. Third, we defined low volume as fewer than 180 CABG per year. Rural geographically isolated hospitals necessarily have a small catchment area, so those fell into the fewer than 180 CABG per year group. We compared outcomes from these 17 low-income low-volume hospitals to the other 41 Northern California hospitals performing CABG operations. We performed a Chi-square analysis to compare the crude mortality rate. Pearson moment correlation coefficients were calculated to compare risk-adjusted readmission rates and stroke rates. CABG surgery was selected as our study cohort because it requires coordination of complex healthcare throughout many years to achieve less morbidity and mortality.
Results
Our qualitative evidence synthesis of published literature reveals that informal communication and hospital HMO policies improve CABG outcomes. In our small pilot dataset, we found in 2009, 17 hospitals in low-income low-volume centers performed 1507 CABG. The crude mortality rate for CABG operations, on average, was 2.72%, that is, 41 deaths within 30 days of surgery. The crude mortality rate for the other 41 centers was 1.69%, that is, 138 deaths out of 8163 operations, an absolute reduction of 1.03% (Table 1). These differences were highly statistically significant when we performed Chi-square analysis (2.72% vs 1.69%, p = 0.0064, Figure 1). Low-income low-volume hospitals had a relative mortality risk of 1.61, with a 95% confidence interval of 1.14–2.27. These 17 hospitals had a readmission rate of 11.12% and a stroke rate of 1.84%. The other 41 hospitals had a readmission rate of 13.1% and a stroke rate of 1.67%. The 17 low-income low-volume hospitals performed on average 89 CABG annually, compared to 194 at the other hospitals. Those hospitals in zip codes with lower individual average income (more so than in those living below the poverty limit) tended to experience more crude (more so than risk-adjusted) readmissions and strokes. A patient undergoing CABG in a low-income low-volume hospital had a 61% higher chance of dying. The number needed to treat analysis shows that one life can potentially be saved for every 97 patients referred to another institution for CABG.
Data collected from 2009 from the 58 hospitals in this study.

CABG, coronary artery bypass graft; CCORP, California CABG Outcomes Reporting Program.

Boxplot of high-volume high-income quartiles and means, compared with all the other Northern California CABG centers.
Discussion
Three components that determine surgical mortality and cost are coordination of preoperative optimization and prehabilitation of comorbidities, team skill, and continuity of care. CCORP defines operative mortality as a death in the hospital or transfer facility within 90 days of CABG or as a death after discharge from the hospital within 30 days of CABG. CCORP defines risk-adjusted mortality using a statistical technique that allows fair comparisons, although some hospitals have patients with more comorbidities. We chose to examine crude mortality because a hospital network can transfer patients with complex conditions to a regionalized center, and crude mortality data will expose which hospitals perform better. We believe SES relates to complex comorbidities and should have been included in CCORP risk-adjusted mortality rates. A healthier patient population can be induced through comprehensive care.2,18
Optimization
In the United States, the approval to perform an invasive procedure is not dependent upon the outcomes in a given patient population, except for the minimal requirements listed by Medicaid and Medicare. These do not include expectations of prolonged life or improved quality of life. As a result, a disproportionate fraction of resources are allocated to satisfy a patient’s uninformed demand rather than what a multidisciplinary group of primary and preventative care physicians would argue is beneficial. For example, beneficiaries with lower SES were less likely to use hospice care but tended to use ER, ICU, and inpatient care. 2
The SYNTAX trial of 2014 measured the cost-effectiveness of CABG at $8132 per quality-adjusted life years (QALY) gained, far below $50,000 per QALY gained considered by most groups to be cost-effective. Even though CABG is associated with approximately $8600 higher initial procedure and hospitalization costs per patient, compared to stents, costs are offset by repeat revascularization and cardiac medications. 19 In Medicaid populations, morbidity can be attributed to restenosis during non-compliance with clopidogrel, smoking, head trauma, and gastrointestinal bleeding.
Patient demographic and clinical risk factors, rather than measured hospital characteristics, accounted for most of the observed hospital variation in CABG readmissions. A fourfold decreased mortality may be mostly from preoperative risk stratification, resulting in not performing the highest risk CABG, thus saving costs as Kaiser does. For example, if a patient is obese, the benefits of prehabilitation reduce the risk of postoperative cognitive decline. Six weeks of exercise, nutrition, smoking cessation, reduction of hemoglobin A1C, etc., can improve outcomes. Low metabolic capacity and obesity were proven to be risk factors for postoperative cognitive decline in rats bred to have extreme metabolic syndrome after 35 generations. 20 Although studies performed in animals cannot be extrapolated to humans, the findings are impressive and warrant further study. Unfortunately, patients with exercise-induced angina are not candidates for a prehabilitation program such as running a treadmill. Just 6 weeks of treadmill exercise for the rats preoperatively prevented all the cognitive decline. The rats were uniformly obese, hypertensive, hyperlipidemic, and diabetic. Surgical trauma via neurohormonal and inflammatory pathways allowed permanent cognitive decline, further proved by staining of the regions involved in the memory of these rats’ brains postmortem. 20
One proposed method to decrease patient morbidity and mortality is the integration of a single electronic medical record spanning all hospitals nationally. 3 In addition, disease-specific multidisciplinary recurring conferences preoperatively, with attached frequent primary care visits, will optimize comorbidities and encourage prehabilitation. Monthly meetings often occur via video with the patient’s primary care physician, the surgeons, anesthesiologists, and cardiologists. Also present via video conference is a dedicated nurse practitioner, who will longitudinally call the patient to pretreat existing infections, by insisting on seeing annual dental X-rays, cleaning certificates, and urine cultures. The nurse practitioner will also ensure control of hypertension as measured by brain natriuretic peptide and diabetes measured by hemoglobin A1c, among other key comorbidities (Table 2). That same primary care clinician would follow all complex layers of postoperative care, continuing into rehabilitation pathways such as physical therapy. Clinicians can call patients at home or visit them in their home.10,21
Common factors contributing to enhanced recovery after surgery at HMO.
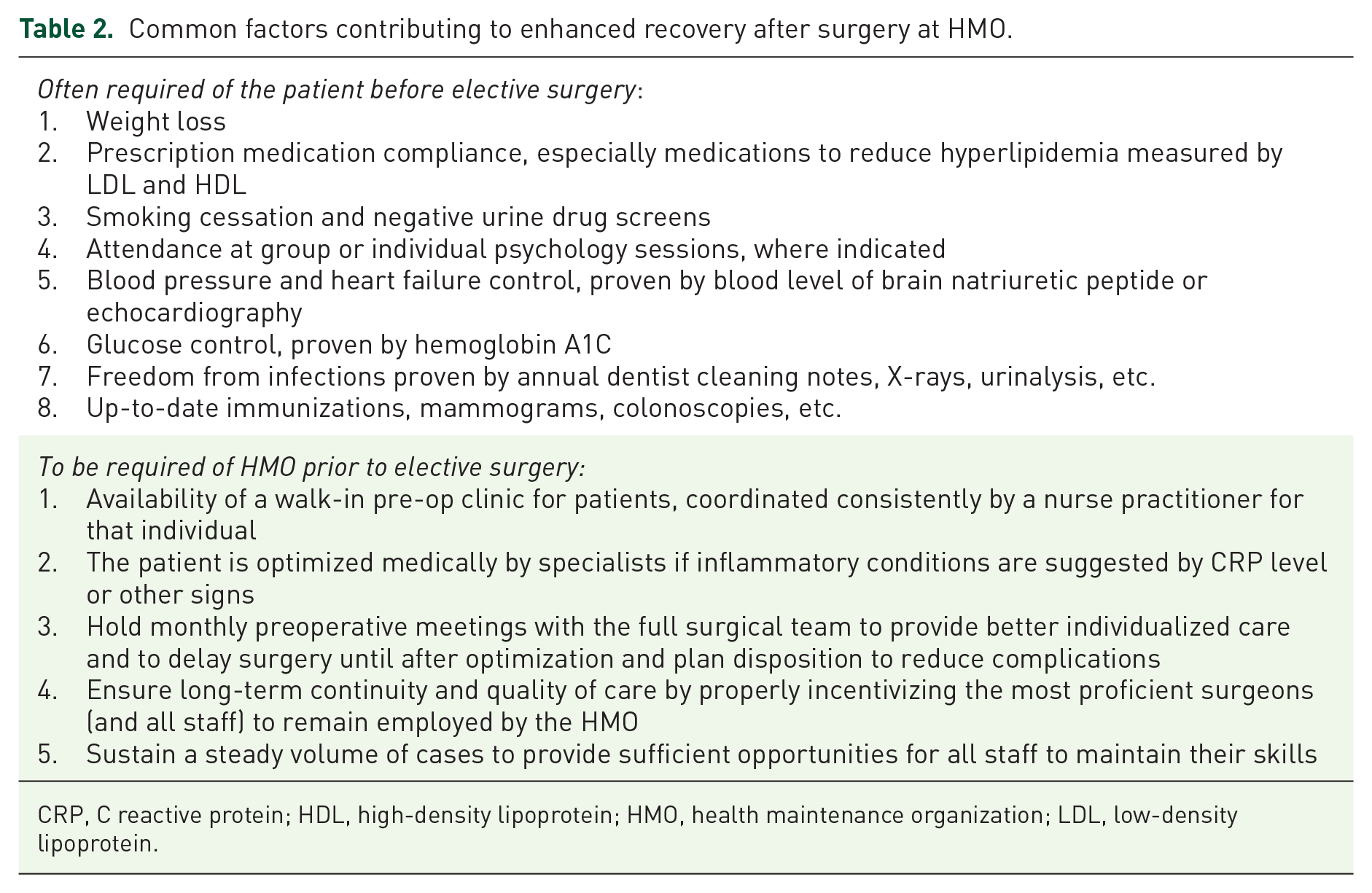
CRP, C reactive protein; HDL, high-density lipoprotein; HMO, health maintenance organization; LDL, low-density lipoprotein.
Team skill and volume
Lack of surgical team skills contributes to up to nine-fold higher risk of mortality. 21 Not only the surgeon but also the ICU nurses, anesthesiologists, nurse practitioners, cardiologists, and primary care physicians matter in terms of outcomes. In Canada, where care is already regionalized, high-volume versus low-volume centers arrived at a plateau in 2002, showing no difference in mortality. A study investigating whether Canada should further regionalize health services found mortality at high-volume centers is decreased with improved surgical training and technical advances. The decrease in mortality in relation to caseload is not a linear relationship but reaches a plateau at about 200 cases/year. 5 It is also important to consider that Canada has a national healthcare system, providing continuity of care. In the wake of the COVID-19 pandemic and healthcare provider burnout, aspects of teamwork can be disjointed.
Continuity of care
A large HMO allows continuity of preoperative communication between patients and more specialists, triage of patients who will benefit from surgery in terms of quality of life, and thorough postoperative care.12,18 Without an HMO clinician calling their homes and offering positive reinforcement of procedures only after compliance with their overall individualized plan, patients may continue to smoke or not take medications and thus worsen outcomes. For example, waiting until a patient sees a dentist before allowing a hip replacement is positive reinforcement to see a dentist.
Heart failure and postoperative infections were the most frequent reasons for readmission (15% and 12%), with household income and age notable predictors. 6 Age, gender, race, creatinine, peripheral artery disease, diabetes, atrial fibrillation, heart failure, and insurance status were significant predictors of readmission. None of the hospital characteristics, including teaching status, type of ownership, geographic region, bed size, or CABG volume, were significant predictors of readmission. 22
Some types of insurance coverage were significantly associated with higher readmission rates: Medicare 15.0% versus Medicaid 18.9% versus private insurance 9.7%.6,10,11 Their model showed that age, female sex, non-White race, preoperative creatinine level, peripheral artery disease, diabetes mellitus, atrial fibrillation, and heart failure were each significant predictors of readmission. Medicaid patients had a twofold higher risk of mid-term mortality after CABG (95% CI: 1.2–3.7). At one institution, long-term survival after CABG in over 5000 patients was evaluated compared to Medicaid Status. 23 Medicaid had a hazard value of 2.1 for mid-term mortality but not in-hospital mortality. In over 174,000 patients, non-White patients had a 33% higher risk-adjusted mortality than White patients. Hospital quality accounted for 35% of this disparity, and 18% was accounted for by poor SES.4,14
Long-term primary care can prevent heart failure and infections. Efforts can be checklists, education, outreach, walk-in clinics, telemedicine, and “boots on the ground” nurse practitioners in a patient’s home while calling the collaborating primary care physician for advice. We propose the practices in place at hospitals with favorable outcomes may be extrapolated to other hospital systems. For example, Stanford created collaboration and demonstrated a sustained improvement in maternal mortality. 24 Their funding was from federal Title 5 and state programs, and they disseminated education to over 99 hospitals providing maternity care. Their toolkits included materials and checklists of algorithms for postpartum hemorrhage, reducing Cesarean sections, and, to the point of our research study, detecting and optimizing primary care for mothers with chronic cardiac disease. Cardiac disease is now the number one cause of maternal mortality at 1 year after delivery, often arising in the setting of substance use disorder, obesity, poverty, or lack of primary care. They established a network of primary care clinics for mothers in California. Where these initiatives work, it would be wise to copy the systems organized by local collaboratives at universities, funded at a federal level, rather than continuing federal piecemeal Medicaid payments for each invasive procedure. 25
Costs
We explain barriers to reducing costs, such as regionalization to high-volume centers, hiring a set of uniformly high-quality specialists in a competitive medical group, preoperative meetings, and more continuous communication between patients and specialists. Patients choose a desirable HMO and pay premiums for this long-term follow-up. Patients who cannot afford an HMO appear at later stages of disease at safety-net hospitals. System issues at those hospitals, such as lack of funds or organizational leadership, contribute to adverse outcomes like infections. When a safety-net hospital coordinates efforts to reduce infections through awareness campaigns, including informal communication and positive rewards, surgical site infections may be cut in half. For example, at Parkland Hospital in Dallas, a 770-bed safety-net hospital, surgical site infections dropped from 3.4% to 1.3%; the primary mechanism was proven simply by measuring liters of hand sanitizer purchased doubled. 26
A plausible explanation for the dissociation of outcomes and costs at any given hospital could include uncoordinated approaches to healthcare in America versus Canada or Europe. Various hospital systems and individuals move between these systems in America, guided predominately by complex insurance structures favoring profitable procedures. Payments to hospitals accounted for the largest share of variation in payments. 17 Among specific types of payments, those associated with 30-day readmissions and post-acute care varied most substantially across hospitals. A reasonable explanation is that patients in lower SES provide a hospital with lower payments than required for their long length of stay. 25
A higher quality of care for CABG patients is likely to result from referral to coordinated regional centers, where physicians are guaranteed a fixed annual salary with a smaller bonus for quality and volume (Table 2). It is possible for hospitals to pressure teams to perform more procedures that profit the hospital, especially if physicians are employed directly by a hospital. 11 An HMO-style network may be less likely to encourage CABG operations for the Medicare-derived profit of the operation itself.
Conclusion
We aimed to investigate what features integrated by any HMO improve the mortality of patients undergoing CABG. To test whether an HMO structure is conducive to better outcomes, we also investigated a subset of data to discover how SES relates to outcomes. Patients who were members of Kaiser, even if in low-income and low-volume areas, were automatically transferred to a large city Kaiser. CABG was selected as the test case because it requires coordination of care through a long preoperative and postoperative phase to achieve less morbidity. This small but original pilot study was conducted before the ACA or COVID-19-associated disruptions to hospital systems, especially in rural areas. We propose that the practices seen in hospitals with the most favorable outcomes may be extrapolated to improve other hospital systems. We identified the best outcome at the lowest cost occurs when primary care physicians optimize patients preoperatively with both formal and informal communication among specialists. 15 Also key are high-quality surgery teams in a high-volume hospital, followed by years of continuity of comprehensive care. 27
During the consolidation of small groups into larger ones, burnout of staff, and delayed care from the obesity, opiate, and then COVID-19 epidemics, we describe factors contributing to fragmented care for individuals formerly stable at an HMO, strained even in that setting. Future research should guide the toolkits that improve the coordination of cost-effective healthcare within large hospital networks. 28 Besides such expensive fragmented care, poor SES should not dictate poor access to quality surgeons and hospitals.29,30 A weakness of our review stems from the bias that any dataset can have. Parker et al. found that this California administrative data set showed a similar mortality prediction as a clinical model, although some outliers were not similar. 31