
Abstract
Background:
Despite the use of safe and effective conventional drugs, drug therapy problems (DTPs) pose a threat to the successful management of hypertension. DTPs are of a great concern in health care because of their serious consequences such as poor quality of life, increased health care costs, morbidity and mortality. However, there is no published information regarding the prevalence of DTPs and associated factors among hypertensive patients in Uganda.
Objective:
The aim of the study was to determine the prevalence and factors associated with DTPs among hypertensive patients at the hypertension clinic of Mbarara Regional Referral Hospital (MRRH).
Method:
A cross-sectional study was conducted at the hypertension clinic, MRRH, Uganda among 228 hypertensive patients. Data were collected from medical records using a data abstraction tool and patients were interviewed using a structured questionnaire. Data analysis was done using Statistical Package for Social Sciences (SPSS) version 22.0. Descriptive analysis was used to determine the prevalence of DTPs. Logistic regression was used to determine the association between the independent and dependent variables. Variables were considered statistically significant at p-value <0.05.
Results:
A total of 178 DTPs were identified among 141 hypertensive patients. The prevalence of antihypertensive-related DTPs was 61.8% (95% confidence interval [CI]: 55.3–67.5) with an average of 1.26 ± 0.52 DTPs per patient. Out of 141 participants with DTPs, 109 (77.3%) had one DTP, 27 (19.1%) had 2 DTPs, and 5 (3.5%) had 3 DTPs. The most common types of antihypertensive-related DTPs were ‘dosage too low’ which accounted for 53 (29.8%), followed by ‘adverse drug reactions’ which accounted for 48 (27%). Uncontrolled blood pressure (BP; adjusted odds ratio [AOR]: 4.17; 95% CI: 2.33–7.45, p < 0.001) and routine laboratory test results (AOR: 1.87; 95% CI: 1.04–3.36, p = 0.036) were significantly associated with antihypertensive-related DTPs among hypertensive patients.
Conclusion:
Almost two-thirds of study participants had antihypertensive-related DTPs. The most common DTPs were ‘dosage too low’ and ‘adverse drug reactions’ which both accounted for almost a third of the total DTPs each. Uncontrolled BP and routine laboratory test results were significantly associated with antihypertensive-related DTPs among the study participants. Our study emphasizes the need for improved patient care by clinical pharmacists to identify and prevent DTPs among hypertensive patients.
Introduction
Hypertension is defined as persistently elevated arterial blood pressure (BP) of ⩾ 140/90 mmHg. 1 It is a serious medical condition that significantly increases the risks of heart, brain, kidney and other illnesses. 2 It is estimated that 1.13 billion people worldwide suffer from hypertension (HTN), and two-thirds live in low- and middle-income countries. 3 Globally, hypertension remains among the leading cause of mortality accounting for approximately 9.4 million deaths annually and is a growing public health problem in sub-Saharan Africa. 4
Drug therapy problem (DTP) can be defined as any undesirable event experienced by a patient that involves drug treatment, which actually or potentially interferes with achieving the desired goals of therapy and requires expert judgment to resolve. 5 DTPs include ‘unnecessary drug therapy’, ‘needs additional drug therapy’, ‘ineffective drug’, ‘dosage too low’, ‘adverse drug reaction’, ‘dosage too high and finally ‘non -adherence’. 5
Despite the use of safe and effective conventional drugs, DTPs pose a threat to the successful management of hypertension. 6 Patients with hypertension are prone to dose and indication-related drug problems that are attributed to co-morbidities and use of multiple drugs.7–10 Globally, DTPs have become far more prevalent over the past years, accounting for 1.3%–41.3% of hospital admissions. 11 It is also reported that worldwide, more than half of all medicines are prescribed and dispensed inappropriately and half of the patients fail to take them correctly. 12 The prevalence of DTPs in the United States is 89.5%. 13 In Africa, studies reported that 52.8% to 82% of ambulatory hypertensive patients experienced at least one DTP.14–19
DTPs are associated with morbidity, mortality, increased health costs as well as poor quality of life of patients. 20 According to a systematic review in the United States (United States of America) and European countries, the cost of treating DTPs especially adverse drug reactions (ADRs) among out patients is about €174 to €8,515. 21 In Nigeria, the economic cost implication of treating DTPs was € 1050.64, equivalent to about 1.9% of the total cost of all medications used by all medical inpatients during admission. 22 According to a study conducted in Spain, drug-related mortality was at 18.4%, 23 whereas a systematic review in Africa indicated that the mortality rate among patients hospitalized due to DTPs was as high as 5.7% with an average rate of 2.7%. 11 Patients with hypertension have a higher risk for DTPs due to multiple co-morbid conditions and use of multiple drugs that predispose them mostly to drug–drug interactions and ADRs. 24 Other factors associated with DTPs among patients with hypertension include polypharmacy, presence of co-morbidities, older age (above 65 years), uncontrolled blood pressure, females and low family income.25,26 The most common antihypertensive-related DTPs among ambulatory hypertensive patients are unnecessary drug therapy, need for additional drug therapy, dosage too high and ineffective drug therapy. 16
In Uganda, the prevalence of hypertension is 31.5% in adults. 27 According to the World Health Organization (WHO) report in 2018, non-communicable diseases (NCDs) are estimated to account for 33% of all deaths in Uganda, and the mortality rate due to cardiovascular diseases is 10% of which hypertension is the most common. 28 Despite the increasing mortality rate, hypertension awareness, treatment and control are unacceptably low across the globe, especially in low- and middle-income countries. 29
Although there are several studies done in other countries on the prevalence of DTPs among ambulatory hypertensive patients, no similar study has been done in Uganda. Therefore, this research was aimed at determining the prevalence, types and factors associated with antihypertensive-related DTPs among patients at the hypertension clinic of Mbarara Regional Referral Hospital (MRRH).
Methods and materials
Study design and setting
A cross-sectional study was conducted at the hypertension clinic of Mbarara Regional Referral Hospital for a period of 3 months from 2 November 2021 to 30 January 2022. MRRH is a government aided hospital located in Mbarara district in the South western region of Uganda. The hospital majorly serves over 4 million people from South-Western districts of Uganda. It has 600 beds and provides general out-patient, in-patients and emergency services. Currently, the hypertension clinic serves about 450 hypertensive patients and this clinic is run by 1 physician, 3 medical residents, 1 medical officer, 1 nursing officer and 1 records officer. The hypertension clinic day is every Tuesday of the week and the services offered include; triage (BP measurement, height measurement, weight measurement), health education and treatment. Hypertensive patients are prescribed drugs for 2 months, that is, every 2 months; these patients come back to the clinic for review.
Study population
All ambulatory hypertensive patients on follow up at MRRH, who visited the hypertension clinic during the study period.
Eligibility criteria
Inclusion criteria
All hypertensive patients 18 years and above who visited the hypertension clinic during the study period and had used antihypertensive drugs as well as consented to participate were included in the study.
Exclusion criteria
Patients with incomplete medical records and those that were unable to complete the interview were excluded.
Sample size
The sample size for the study was determined using single population proportion formula (Cochran, 1963)

where n = sample required, Z = critical value for 95% confidence interval (1.96), e = margin of error (5%) = 0.05, P = prevalence rate = 50% since there was no similar study done in Uganda and in East Africa, n = (1.96 x 1.96 x 0.50 x 0.50) / (0.05 x 0.05) = 384 participants.
The hypertension clinic serves a total of 450 hypertensive patients which is less than 10,000 people. Applied the finite population correction formula

where n is the sample size and N the population size, n = 384/1 + ((384 – 1)/450), n = 207 participants.
Additional 10% of the sample size for contingency, which led to a total of 228 participants.
Sampling technique
Systematic random sampling technique was used in this study.
Data collection methods and procedures
The data collection team consisted of the principal investigator (clinical pharmacist) and two trained research assistants (pharmacist and a medical resident). After the systematic random sampling, the selected patient’s details were checked against a list of patients who had previously taken part in the study to ensure that each eligible patient participates once. The patient would then voluntarily consent to participate in the study by writing. Thereafter, patients were interviewed using a structured questionnaire to obtain data on socio-demographics (marital status, religion, monthly income and education level), history of drug allergies, medical history, medication history which included herbal and over-the-counter drugs, medication adherence to prescribed drugs and ADR.
For medication adherence, questions adopted from Hill-Bone medication adherence scale were asked. 30 Non-adherence was considered if the drug therapy was indicated, effective and safe. Males and females were considered non-adherent if they scored <29.1 and <32.3, respectively. 30 Once non-adherence was identified, the Cipolle et al. 5 classification was used to determine the cause.
ADR were suspected when there was a relationship between time of drug administration and the onset of the ADR while excluding other causes. All suspected adverse events were assessed using the Naranjo Scale. Participants with definite (⩾9), probable5–8 and possible1–4 ADR causality scores in the Naranjo ADR causality algorithm were considered to be having ADR related to drug therapy. 31
Data from review of medical records were collected and recorded using a pretested data abstraction tool. Medical records were reviewed to obtain data on vital signs, current medication, results of current laboratory tests, ADR (clinical and laboratory evaluations) and the current medical conditions which were important for identification of DTPs.
Each documented drug therapy was evaluated for appropriateness, effectiveness and safety using the Lexicomp drug interaction checker and the Uganda clinical guideline. 32 According to Lexicomp drug–drug interaction checker, only drug–drug interactions in class C (monitor therapy), D (consider therapy modification) and X (avoid drug combination) are considered clinically significant. Identified DTPs and their causes were broadly classified according to the Cipolle et al. 5 classification system. Enrollment of patients was halted after the estimated sample size of 228 participants was reached.
Operational definitions
Controlled blood pressure
Is BP that is < 140/90 mmHg. 32
Drug therapy problem
Can be defined as any undesirable event experienced by a patient that involves drug treatment, which actually or potentially interferes with achieving the desired goals of therapy and requires professional judgment to resolve. 5
Unnecessary drug therapy
Can be defined as patient not having a clinical indication for drug therapy at a time, multiple drug products are being used for a condition that requires only single drug, non-drug therapy more appropriate, addiction or recreational drug use and treating avoidable adverse reaction. 5
Needs additional therapy
Additional drug is required to initiate therapy for untreated condition or to prevent a new medical condition from developing in the patient or synergistic therapy for a medical condition that requires additional pharmacotherapy. 5
Ineffective drug
The drug not being the most effective for the medical condition and a different drug is needed, the medical condition is refractory to the drug product and a different drug is needed or maybe the dosage form of the drug product is inappropriate, the drug product is contraindicated in this patient, and finally drug is not indicated for condition. 5
Dosage too low
Too low dosage to produce the desired response in the patient, the dosage interval is too infrequent to produce the desired response, incorrect administration, a drug interaction reduces the amount of active drug available resulting in lack of effectiveness in this patient, and then the duration of the drug therapy is too short to produce the desired response. 5
Adverse drug reaction (ADR)
The World Health Organization (WHO) defines an ADR as a response to a drug that is noxious and unintended and which occurs at doses normally used in man for prophylaxis, diagnosis or therapy of disease or for the modification of physiological function. 33
Dosage too high
Dose too high can be related to toxicity, the dosing frequency being too short for the patient or duration of drug therapy is too long for a patient or a drug interaction increases the amount of active drug available resulting in toxicity in a patient. 5
Quality control
Pre-testing of the data collection tool was done using 10 patients who met the inclusion criteria. This was to help in identifying challenges with the data collection tool and there-after the tool was modified accordingly.
The data collection tool was translated to Runyankole by a professional and then results were back translated to English to check for consistency. The principal investigator selected and recruited research assistants who were trained on the aim of the study, data collection techniques and how to use the data collection tool. The recruited research assistants were fluent in both English and Runyankole which facilitated patient interview. The principal investigator also closely supervised research assistants during the data collection period.
Data management
The data abstraction form for each patient was assigned an identification code. The filled forms were checked for accuracy, consistency and completeness by the principal investigator on a daily basis. Completed forms were kept under restricted access to protect patient confidentiality and protect data from alteration. Data were later stored in a computer with a password.
Data analysis
All filled data collection forms were checked for completeness in preparation for data entry into statistical package for social sciences (SPSS) version 22.0. Data cleaning was done to detect errors and validate the data. Data analysis was done using the same software. Patient, drug and disease-related factors were presented using descriptive statistics including mean, standard deviation, frequencies and percentages.
The prevalence of DTPs related to antihypertensives was determined by the number of patients with at least one DTP divided by the total number of the sample size. The results were expressed as a percentage.
The association between the independent variables and occurrence of DTPs was determined using univariate and multivariate logistic regression. Variables with p-value < 0.25 during the univariate analysis were further subjected to multivariate logistic regression analysis to control for confounders. Variables were considered statistically significant if p-value was less than 0.05 measured with odds ratio at 95% confidence interval.
Ethical considerations
Approval to conduct the study was obtained from Mbarara University of Science and Technology Research Ethics Committee (Reference number: MUST-2021-187). Written informed consent was obtained from the patients prior to participating in the study and use of their medical records. The purpose, objectives, benefits and risks as well as the impact of the study on the total time spent in the hospital were clearly explained to the patients. Completed forms were kept under restricted access and thus data were processed and presented anonymously to prevent anyone from tracing back the patient’s identity which preserved confidentiality.
Ministry of health COVID-19 guidelines were observed during the data collection process. These guidelines included social distancing, wearing face masks all the time and sanitizing before and after handling patient medical records.
Results
Socio-demographic characteristics of patients
About 230 hypertensive patients were recruited for the study, and 2 were excluded due to incomplete data giving us a total of 228 hypertensive patients that participated in this study. Out of these, majority were females accounting for 173 (75.9%) and 113 (49.6%) were in the age bracket 40–59 years. The mean age of the study participants was 58.13 ± 12.16 years ranging from 23 years to 86 years. In addition, 133 (58.3%) were married, 104 (45.6%) were Anglican by religion, 114 (50%) attended primary education, and 117 (51.3%) were unemployed. Twenty (8.8%) participants were currently using alcohol, 4 (1.8%) were still smoking and 62 (27.2%) were currently using herbal drugs (Table 1).
Socio-demographics characteristics of the study participants at the hypertension clinic, MRRH, from November 2021 to January 2022.

MRRH: Mbarara Regional Referral Hospital.
Drug and disease characteristics of study participants
Eighty-three (36.4%) of the patients were overweight and almost two-thirds (149, 65.4%) had uncontrolled BP. In this study, the mean duration of hypertension since diagnosis and initiation of antihypertensive was 5.08 ± 4.41 years and 4.79 ± 4.13 years, respectively. The majority (133, 58.5%) of the participants had at least one co-morbid condition. The most frequently diagnosed co-morbidities were diabetes mellitus 74 (32.5%), and neuropathy 39 (17.1%). The average number of prescribed drugs was 3.85 ± 1.61 whereas an average of 2.18 ± 0.89 antihypertensive drugs was used. Among the study participants, 192 (84.2%) were prescribed calcium channel blockers (CCB) such as immediate release Nifedipine and Amlodipine, 126 (55.3%) were prescribed diuretics such as Bendroflumethiazide, and 119 (52.2%) were prescribed angiotensin receptor blockers (ARB) such as Losartan and Telmisartan (Table 2).
Drug and disease characteristics of the study participants at MRRH from November 2021 to January 2022.
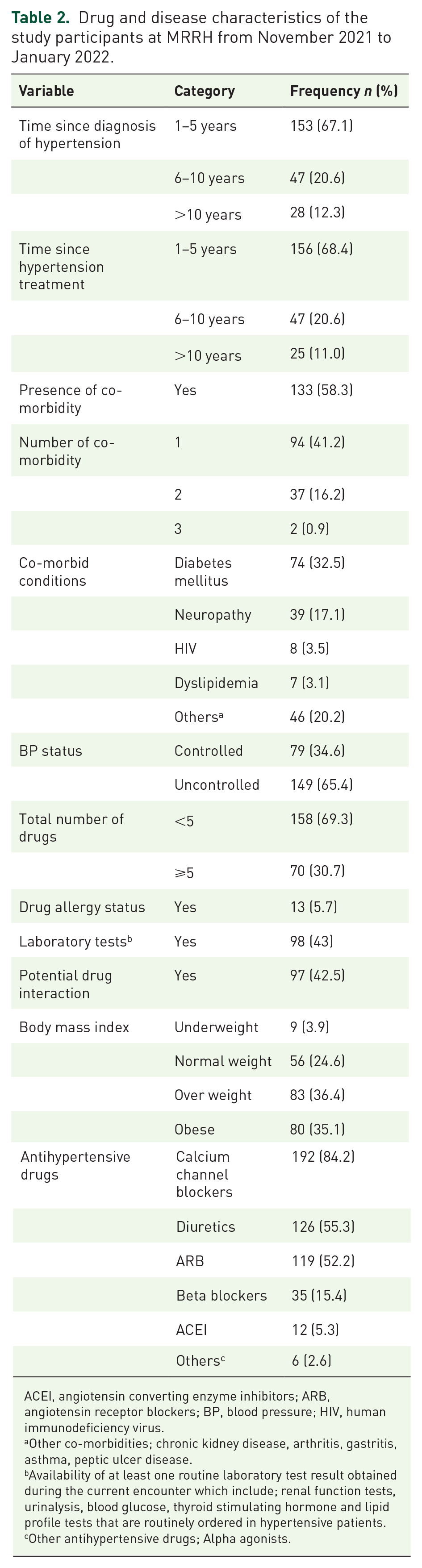
ACEI, angiotensin converting enzyme inhibitors; ARB, angiotensin receptor blockers; BP, blood pressure; HIV, human immunodeficiency virus.
Other co-morbidities; chronic kidney disease, arthritis, gastritis, asthma, peptic ulcer disease.
Availability of at least one routine laboratory test result obtained during the current encounter which include; renal function tests, urinalysis, blood glucose, thyroid stimulating hormone and lipid profile tests that are routinely ordered in hypertensive patients.
Other antihypertensive drugs; Alpha agonists.
Prevalence of antihypertensive-related DTPs
A total of 178 DTPs were identified among 141 hypertensive patients and the prevalence of antihypertensive-related DTPs was 61.8% (95% confidence interval [CI]: 55.3–67.5]. The average number of DTPs was 1.26 ± 0.52 DTPs per patient. Out of the 141 study participants with DTPs, 109 (77.3%) had one DTP, 27 (19.1%) had two DTPs and 5 (3.5%) had three DTPs.
Types and causes of antihypertensive-related DTPs
Dosage too low was the most common antihypertensive-related DTP accounting for 53 (29.8%), followed by ADRs, and non-adherence which accounted for 48 (27.0%) and 34 (19.1%) respectively. The least identified DTP was unnecessary drug therapy and it accounted for 2 (1.1%), (Figure 1).

Types of antihypertensive-related drug therapy problems identified among patients at MRRH from November 2021 to January 2022.
Of the dosage too low, ineffective dose was the major cause and it contributed 41 (23%) while ADRs were caused by undesirable effects which accounted for 35 (19.7%). Non-adherence was mainly caused by inability to afford drug therapy which accounted for 18 (10.1%), (Table 3). Immediate release Nifedipine contributed the most DTPs accounting for 63 (27.6%), followed by Amlodipine 22 (9.6%) and then Losartan 16 (7%).
Types of antihypertensive-related drug therapy problems and their causes among patients at the hypertension clinic, MRRH from November 2021 to January 2022.

DTP, drug therapy problems.
Factors associated with occurrence of antihypertensive-related drug therapy problems
Univariate logistic regression of the factors associated with occurrence of antihypertensive-related DTPs
At univariate logistic regression, treatment of hypertension for > 10 years (COR: 3.46; 95% CI: 1.13–10.57; p-value = 0.029), BP control (COR, 4.37; 95% CI: 2.44–7.80; p-value < 0.001) and availability of routine laboratory tests results (COR, 1.92; 95% CI: 1.10–3.34; p-value = 0.022) were significantly associated with antihypertensive-related DTP occurrence (Table 4).
Univariate and multivariate analysis of factors associated with antihypertensive-related DTPs among patients at MRRH from November 2021 to January 2022.

AOR: adjusted odds ratio; BP, blood pressure; CI, confidence interval; COR: crude odds ratio; DTP, drug therapy problems; HTN, hypertension.
Multivariate logistic regression of the factors associated with antihypertensive-related DTPs
All variables with p-value < 0.25 at univariate analysis were considered for multivariate logistic regression analysis. Multivariate analysis presented in Table 4 showed that study participants with uncontrolled BP were 4.17 times (adjusted odds ratio [AOR]: 4.17; 95% CI: 2.33–7.45; p-value < 0.001) more likely to experience DTPs compared to participants with controlled BP. Patients with routine laboratory test results were 1.87 times (AOR: 1.87; 95% CI: 1.04–3.36; p-value = 0.036) more associated with antihypertensive-related DTPs than those who didn’t have them.
Discussion
This study was conducted at the hypertension clinic with the aim of establishing the prevalence, types and factors associated with antihypertensive-related DTPs among hypertensive patients. During the study period, 178 DTPs were identified among 141 (61.8%) hypertensive patients with an average of 1.26 ± 0.52 DTPs per patient. The most common types of DTPs were ‘dosage too low’ which accounted for 53 (29.8%), followed by ‘adverse drug reactions’ which accounted for 48 (27%). The multivariate logistic regression analysis showed that uncontrolled BP and availability of routine laboratory test results were significantly associated with DTPs among hypertensive patients.
The current prevalence of antihypertensive-related DTPs of 61.8% is comparable to other studies in Northwest, Ethiopia (62.4%), Eastern Ethiopia (60.5%), Northern Ethiopia (55.6%) and Indonesia (57%).7,14,26,34 However, this finding is lower than 71.2% and 80.7% both in Eastern Ethiopia as well as 82% in Southwest Ethiopia.15,19,25 In addition, studies conducted in Malaysia showed that 88.8% and 90.5% participants had at least one DTP.35,36 The contrast in results could be attributed to difference in assessment of DTPs; our study excluded DTPs related to other drugs other than antihypertensives unlike the other studies that included DTPs related to all drugs. The variation in findings could also be due to difference in study setting, study population, study design and DTP classification; the study by Huri and Wee used retrospective study design and used in-patients, the two studies in Malaysia also used the pharmaceutical care network Europe foundation to classify DTPs whereas our study used the Cipolle classification.
Our study found out that the most common DTP was ‘dosage too low’ at 29.8%. This finding is higher than that reported in Indonesia, Malaysia and Nigeria; ranging from 5.2% to 7.7%.35,37,38 Furthermore, the dosage too low in our study is also higher than 18.5% and 16.8% in two studies conducted in Ethiopia.14,26 The discrepancy in findings could be due to variations in study population and medical practitioner’s expertise and experience. The study by Kefale et al. 26 had 100% patients having both hypertension and diabetes mellitus, whereas our study had only 32.5% having both conditions. The high proportion of ‘dosage too low’ in our setting could be attributed to prescribing an ineffective dose and too infrequent dosing. The failure to control BP adequately among two-thirds (149, 65.4%) of our study participants could be attributed to ‘dosage too low’. This implies the need to adhere to standard treatment guidelines in order to achieve the desired BP goal.
In this study, ‘adverse drug reactions’ accounted for 27%. This finding is comparable with 31.6% reported in a cross-sectional study conducted in Indonesia. 34 However, our results are higher than 19% reported in a retrospective cross-sectional study conducted in Eastern Ethiopia. 17 In addition, the finding also differs from 2.4% reported in a prospective cross-sectional study conducted in Southwestern Ethiopia. 19 The variation could be explained by the presence of a high prevalence of co-morbidities and drug-drug interactions in our setting. In addition, ADRs in our setting were caused by drugs causing undesirable effects and need for safer drugs especially for older adults. Furthermore, Nifedipine contributed the most (77.1%) to the ADRs in our setting. Clinical trials recommend use of long acting CCBs because they have proven efficacy and safety in older adult patients with hypertension.39,40
Non-adherence accounted for almost one-fifth (19.1%) of the antihypertensive-related DTPs. This was mainly (52.9%) attributed to inability to afford drug therapy since patients must use their ‘out-of-pocket money’ to buy drugs from private pharmacies. This finding is lower than 32.8% reported in study conducted in Ethiopia. 10 The difference in findings could be due to variations in socio-economic status, provision of adherence counseling services and adherence assessment tools used. Our study used the hill-bone medication adherence tool which is specific to hypertensive patients whereas the later used the Morisky medication adherence tool. Although uncontrolled BP could be attributed to other different factors such as lifestyle characteristics of patients, ‘dosage too low’; non-adherence could be an important factor among our study participants. Non-adherence to antihypertensive drugs accounts for 30%-50% and is often linked to uncontrolled blood pressure. 41 This therefore, implies that healthcare professionals should strengthen adherence counseling to raise awareness and knowledge in relation to BP control.
The multivariate logistic regression analysis showed that study participants that had uncontrolled BP were 4.17 times (AOR,4.17; 95%CI, 2.33-7.45, P-value < 0.001) more likely to have DTPs as compared to those with controlled BP, which was in agreement to findings in a study conducted by Hussen and Daba who reported that patients with uncontrolled BP were 7.68 times more likely to have DTPs. 25 The most likely cause of uncontrolled BP could be non-adherence to antihypertensive drugs. From our study, non-adherence contributed to 19.1% of the total number of DTP related to antihypertensives. A study conducted in Iran reported that there was a significant relationship between adherence level and BP control. 42 A systematic review and meta-analysis in low- and middle-income countries also reported a similar finding that adherence was related to BP control. 43
In addition, patients who had routine laboratory test results were 1.87 times (AOR, 1.87; 95%CI, 1.04-3.36, P-value = 0.036) more likely to have DTPs than those that didn’t have them. The more the laboratory tests are performed, the more the safety profile of a drug in a patient is known and the more we are able to identify DTPs. Bolivar et al. 44 also emphases that laboratory monitoring helps to detect the risk of unnecessary ADRs.
In Contrary to the present study, other studies identified total number of drugs, low family income, age, presence of co-morbidity and substance use as factors associated with DTPs among hypertensive patients.7,14,16,26 This difference in findings could be attributed to variations in study population, underlying co-morbid conditions, patient characteristics and DTP assessment. In our study, only antihypertensive-related DTPs were assessed unlike other studies. Our study reported a prevalence of 58.3% for co-morbidities while other studies reported 43% and 34.4%.14,16 The current study had 43.4% study participants who were 60 years and above which was similar to 42.7% by Mahammedsied et al. 16 However, this finding was different from 5.4% and 23.4% among adults above 65 years reported by Weldegebreal et al. 14 and Kefale et al. 26 respectively.
Study limitation and strength
Conducting this study at a single health facility was one limitation identified as the findings may not generate sufficient evidence that could be generalized to the larger population.
Our study strength was involving a team of pharmacists and a medical resident in data collection which might have contributed to the quality of data. In addition, the study used a standardized DTP identification criteria as well as standard tools to assess for both ADRs and adherence.
Conclusion
This study reports that almost two-thirds of study participants had antihypertensive-related DTPs. The most common antihypertensive-related DTPs were ‘dosage too low’ and ‘adverse drug reactions’ which each accounted for almost a third of the total DTPs. Uncontrolled BP and availability of routine laboratory test results were significantly associated with antihypertensive-related DTPs among the study participants. Our study emphasizes the need for improved patient care by devoted healthcare professionals such as clinical pharmacists to identify and prevent DTPs among hypertensive patients.
Supplemental Material
sj-docx-1-tak-10.1177_17539447231160319 – Supplemental material for Prevalence and factors associated with drug therapy problems among hypertensive patients at hypertension clinic of Mbarara Regional Referral Hospital, Uganda: a |cross-sectional study
Supplemental material, sj-docx-1-tak-10.1177_17539447231160319 for Prevalence and factors associated with drug therapy problems among hypertensive patients at hypertension clinic of Mbarara Regional Referral Hospital, Uganda: a |cross-sectional study by Merab Babirye, Tadele Mekuriya Yadesa, Robert Tamukong and Paul Stephen Obwoya in Therapeutic Advances in Cardiovascular Disease
Footnotes
Acknowledgements
First of all, we would like to thank Pharm-Biotechnology and Tradiotional Medicince Center, Word Bank’s ACE-II project at Mbarara University of Science and Technology, for funding this study. We would also like to express our sincere gratitude to the research assistants, who were involved in data collection, the hypertensive patients that participated in the study and the staff of the hypertension clinic, Mbarara Regional Referral hospital for their support and guidance during the data collection period. The authors would also like to express their heartfelt gratitude to Dr. Eriwala William for all support rendered.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.