
Abstract
Background:
Atherosclerosis is a condition in which the medium to large arteries become inflamed over time. The cornerstone to the atherosclerosis process is endothelial dysfunction. Simvastatin is a cholesterol-lowering drug known for its endothelial cell pleiotropic properties. The role of genetic polymorphisms in simvastatin-resistance difficulties has recently piqued people’s interest. This problem is thought to be linked to the pleiotropic action of simvastatin, particularly in terms of restoring endothelial function. The goal of this study is to see if there is a link between the single nucleotide polymorphism (SNP) c.521T>C and the pleiotropic effect of simvastatin as determined by the endothelial function parameter, flow-mediated dilation (FMD).
Methods:
This research was a multicentre cross-sectional study including 71 hypercholesterolemia patients who have been on simvastatin for at least 3 months. The real-time polymerase chain reaction identified SNP c.521T>C. The right brachial artery ultrasonography was used to measure FMD.
Results:
In 71 hypercholesterolemia patients, the SNP c.521T>C was found in 9.9% of them. On χ2 analysis, there was no significant association between SNP c.521T>C (TC genotype) and FMD (p = 0.973). On logistic regression analysis, the duration of simvastatin medication was linked with an increased incidence (Adj. OR (adjusted odds ratio) = 2.424; confidence interval (CI) = 1.117–5.260, p = 0.025) and a reduction in systolic blood pressure (Adj. OR = 0.92; CI = 0.025–0.333, p = 0.001).
Conclusion:
There was no association between FMD and the SNP c.521T>C (TC genotype). The duration of simvastatin medication and systolic blood pressure were both associated to FMD.
Introduction
Cardiovascular disease (CVD) is the leading cause of mortality globally nowadays. The mortality rate due to this disease is estimated at 17.7 million, with 31% of the death rate worldwide. Among these, 7.4 million were caused by coronary heart disease (CHD) related to the atherosclerosis process.1,2 Arterial endothelial dysfunction is one of the keys to initiating atherogenic processes that occur before the structural changes of atherosclerosis. 3 Endothelial function can be measured by the non-invasive flow-mediated dilation (FMD) test. It is used to measure the diameter of superficial arteries such as the brachial, radial, or femoral arteries. 4
Statins have become one of the main cholesterol-lowering modalities in secondary and primary prevention. Statins also affect the vasculature, which is also called a pleiotropic effect in improving endothelial function. 5 The effect of statins may be different between individuals, one of which is caused by the development of statin resistance. 6 Resistance may also result from differences in the levels of pathways for cholesterol synthesis and lipoprotein metabolism, including HMG CoA reductase (HMGcR). Simvastatin itself is in the form of a pro-drug, which is then metabolized to the active form of simvastatin acid. 7 Plasma concentrations of simvastatin and simvastatin acid were found to vary between individuals, leading to variability in the efficacy and toxicity of simvastatin. The organic anion polypeptide (OATP1B1) transporter is a transporter whose job is to uptake both simvastatin and simvastatin acid toward the liver. 8 The SLCO1B1 gene (GeneID: 10599; MIM: 604843) is the gene encoding OATP1B1 that may influence its function. 9
SLCO1B1 gene encodes a liver-specific member of the organic anion transporter family. The encoded protein is a transmembrane receptor that mediates the sodium-independent uptake of numerous endogenous compounds including bilirubin, 17-beta-glucuronosyl estradiol, and leukotriene C4. This protein is also involved in the removal of drug compounds such as statins from the blood into the hepatocytes. Polymorphisms in the gene encoding this protein are associated with impaired transporter function. In a meta-analysis by Hou et al. (2015), nine studies with 1360 cases and 3082 controls were included. Cases of statin-related myopathy were found to be significantly associated with the variant C allele (TC + CC versus TT: odds ratio (OR) = 2.09, 95% confidence interval (CI) = 1.27–3.43, p = 0.003; C versus T: OR = 2.10, 95% CI = 1.43–3.09, p < 0.001), especially when statin-related myopathy was defined as an elevation of creatine kinase (CK) > 10 times the upper limit of normal (ULN) or rhabdomyolysis (TC + CC versus TT: OR = 3.83, 95% CI = 1.41–10.39, p = 0.008; C versus T: OR = 2.94, 95% CI = 1.47–5.89, p = 0.002). When stratified by statin type, the association was significant in individuals receiving simvastatin (TC + CC versus TT: OR = 3.09, 95% CI = 1.64–5.85, p = 0.001; C versus T: OR = 3.00, 95% CI = 1.38–6.49, p = 0.005), but not in those receiving atorvastatin (TC + CC versus TT: OR = 1.31, 95% CI = 0.74–2.30, p = 0.35; C versus T: OR = 1.33, 95% CI = 0.57–3.12, p = 0.52). 10
The single nucleotide polymorphism (SNP) c.521T>C of the SLCO1B1 gene results in a decrease in the function of the OATP1B1 transporter, resulting in a decrease in the concentration of both simvastatin and simvastatin acid in the liver, as well as an increase in the systemic bioavailability of the two substances.11,12 Increased systemic bioavailability will increase the likelihood of vascular endothelial cell exposure to both simvastatin and simvastatin acid. The parameters for improving endothelial function can be measured by examining the FMD of the brachial artery. 13
This study aims to find the association between SNP of c.521T>C SLCO1B1 gene and simvastatin pleiotropic function as measured by FMD endothelial function parameters in patients with hypercholesterolemia receiving simvastatin therapy.
Methods
This study is an observational analytic study with a cross-sectional research design. The sample of this study were hypercholesterolemic patients who had received simvastatin therapy for at least 3 months at the outpatient clinic of three hospital centers in Surabaya, Indonesia. This study is conducted in the outpatient unit and echocardiography room at the Department of Cardiology and Vascular Medicine of the Dr Soetomo Surabaya Hospital, Dr Soewandhie Surabaya Hospital, and Anwar Medika Krian Sidoarjo Hospital between 15 October 2017 and 14 February 2018. This study was approved by Dr Soetomo General Hospital Surabaya Ethical Committee (reference number: 0133/LOE/301.4.2/V/2017) issued on 22 May 2017, under the name of Andrianto as the principal investigator. All procedures were approved by the relevant ethics committees, and written informed consent was obtained from all study participants.
The sample was taken by purposive sampling, with every patient who meets the research criteria included in the subject research until it meets the specified number of samples. Inclusion criteria in this study were hypercholesterolemic patients who have received simvastatin therapy for at least 3 months. The exclusion criteria included patients with a history of coronary artery disease (CAD); patients with chronic kidney disease; patients with chronic infectious diseases such as tuberculosis, hepatitis, or HIV; patients with uncontrolled hypertension, diabetes mellitus, and cancer; or autoimmune patients.
Patients selected based on inclusion and exclusion criteria will fill out a letter of informed consent to participate in the study. After that, 5 mL of venous blood was taken. Blood sampling for venous blood samples for SNP examination of the SLCO1B1 gene was carried out before being stored in a cooler at −20°C. Quantitative polymerase chain reaction (qPCR) using TaqMan® probe 5′ nuclease assay was carried out on these samples.
Genomic DNA was extracted from blood leukocytes by a salting out procedure optimized by Salazar et al. 14 Genotyping of SLCO1B1 polymorphisms was performed using allele-specific protocols of the Taqman®Assays ID followed for the SLCO1B1 c.388A > G (rs2306383) C___1901697_20 and for the c.521T>C (rs4149056) C__30633906_10. Each 6 μL of PCR mixture contained 2 μL of genomic DNA in a concentration of 5 ng/μL, 2.5 μL of TaqMan® Genotyping Mastermix, 0.25 μL of allele-specific TaqMan® probe and sequence-specific primer kit, and 1.25 μL of DNase-free water. The thermal cycler program started with 10 min at 95°C, followed by 50 cycles of 15 s at 92°C and 90 s at 60°C. The allelic discrimination plot was analyzed by ViiA7™ software (Applied Biosystems, Life Technologies, Germany). Allele 1 was labeled with VIC® dye fluorescence, and allele 2 was labeled with FAM™ dye fluorescence.
We used simvastatin (40 mg daily) because data from previous research showed that 40 mg of simvastatin may improve the median FMD from 2.2% to 5.5%, and from 1.8% to 4.5%, respectively. 15
We used FMD by measuring the diameter of the brachial artery with high-resolution external vascular ultrasound in response to an increase in blood flow (causing shear stress) during reactive hyperemia (induced by cuff inflation and then deflation). Based on qualitative assessment, we divided FMD groups into two groups. Actually, we have been interpreted low FMD as no dilation of the brachial artery in response to shear stress. Normal-high FMD was traditionally widening or dilation of the brachial artery in response to shear stress. In our experiments, we usually take scanning period approximately 30 s before and 90 s after the cuff deflation.
The FMD of the right brachial artery was carried out the following day after the patient had been asked to fast for at least 8 h before the examination. FMD was measured by applying pressure to the brachial artery with a sphygmomanometer cuff of 50 mmHg from systolic blood pressure (SBP) or a maximum pressure of 220 mmHg in the distal cubital fossa (forearm). Then the cuff was removed, and the brachial artery diameter was measured again at 10, 60, and 180 s. The maximum diameter of the three measurements was included in the FMD calculation. The calculation is done by calculating the difference between the maximum diameter of the brachial artery after provocation minus the initial diameter multiplied by 100%. If the result is less than 7%, there is endothelial dysfunction; moderate if the result is greater than or equal to 7% means normal. Brachial artery diameter was measured in the end-diastolic phase based on the initial QRS complex. Measurements were made using echocardiography Logiq P7, Vivid S5, and Vivid S6 GE medical system.
The frequency of the functional SNPs within the SCLO1B1 (c.521T>C) gene was assessed for deviation from the Hardy–Weinberg equilibrium (HWE) using SPSS 20.0. Descriptive statistical analysis was used to describe the general characteristics of patients by using the frequency distribution in the form of percentages and presented in tabular form. A χ2 test will be carried out to test the differences in minor alleles frequencies and haplotype frequencies of SNP31 SLCO1B1 and nominal changes in FMD.
Results
This research was a multicenter observational analytic study. Sampling was conducted using the consecutive sampling method, and as many as 71 research participants who met the inclusion and exclusion criteria were selected. Each research participant was taken anamnesis and pooled medical records to collect basic data. Before the sampling procedure was carried out, the intraobserver variability of the FMD variable was calculated with the result of a kappa value of 0.73 (α = 0.016).
Research participants’ characteristics
The results of the analysis of the baseline characteristics of patients stated that there were no differences in the characteristics of FMD except for two variables (Table 1). The first variable was the patient’s SBP which was measured before the FMD examination, in which 32 participants had an SBP exceeding 130 mmHg, while 39 samples had a blood pressure of 130 mmHg or less.
Baseline characteristics.

ACEI/ARB, angiotensin converting enzyme inhibitor / angiotensin receptor blocker; LDL, low-density lipoprotein; SD, standard deviation.
The second variable that has a difference is the duration of simvastatin administration which is calculated from the beginning of the patient receiving simvastatin therapy until the study sample is taken. The duration of simvastatin therapy was divided into three groups: 17 participants for 3–6 months, 34 participants for 7–12 months, and 20 participants for > 12 months.
However, this study did not collect data on adherence to taking medication or setting the patient’s diet. For users of antihypertensive therapy, blood pressure–lowering drugs are still given according to the daily schedule and recordings of the type of drug used and SBP monitoring before the FMD examination begins.
The study sample alleles and genotype frequencies were estimated with a gene counting method. The agreement with HWE of the observed genotypic distribution for the SLCO1B1 gene was tested with the χ2 test. HWE is used to estimate the number of homozygous and heterozygous variant carriers based on its allele frequency in populations that are not evolving. Our gene data set, with phenotype and inheritance data were retrieved from Online Mendelian Inheritance in Man (OMIM) database. A factor causing deviations from HWE that has not been investigated on a large scale is natural selection.
A study by Santos et al revealed that the frequencies of the 521C allele were highest in Amerindians (28.3%) and lowest in African descent participants (5.7%) compared with Mulatto (14.9%) and Caucasian descent (14.8%). 16 In this study, carriers of the so-called c.521T>C of the SLCO1B1 gene (GeneID: 10599; MIM: 604843) had significantly slower response to statin, thus make smaller reductions in total and low-density lipoprotein (LDL) cholesterol than noncarriers. 16
We used a gnomAD v3 and SciPy python implementation of Graffelman and Moreno method in which mid p, calculated by adding only half of the probability of observed sample to the sum of all probabilities of more extreme cases, was less conservative (i.e. mid p is always smaller than two-sided p), and showed better potential for testing deviations from HWE of rare variants. We did not find any deviations from HWE in our population study.
Association between SNP c.521T>C gene SLCO1B1 and the value of FMD
Based on the results of the qPCR examination of 71 samples, 64 samples were obtained with the wild-type TT genotype and seven samples with the TC genotype (9.9%). The CC genotype was not found on examination. Among 71 patients genotyped for SLCO1B1*5 allelic variant, 64 (90%) had wild TT-variant, 7 (9%) had TC-variant, and 0 had CC. 521T-allele occurrence was 0.96 and incidence of 521C allele was 0.04. Genotype frequencies did not deviate significantly from HWE (χ2 = 3.3; p = 0.171). Table 2 describes the distribution of FMD values and genotypes caused by SNP c.521T>C and their associations. In this study, there was no significant difference between the SNP c.521T>C of the SLCO1B1 gene and the participant’s FMD value (p = 0.973), so it could be concluded that there was no relationship between the two variables. Therefore, further analysis is carried out on the variables that are expected to affect the results of the FMD measurement.
Association between single nucleotide polymorphism c.521T>C SLCO1B1 gene and flow-mediated dilation value.

Relationship of confounding variables and value of FMD
There are differences in data on the characteristics of the duration of simvastatin therapy and diastolic blood pressure on FMD values. Based on these data, further logistic regression analysis was carried out to determine the relationship between the confounding variables and the FMD value (Table 3). Overall, the value of adjusted R2 = 0.521 (α < 0.05; p = 0.002) was obtained from these confounding variables. It can be concluded that these confounding variables can affect FMD. The greatest significance of the effect based on Table 3 was found on the variables of simvastatin therapy duration and SBP of the participants. A separate logistic regression was performed on these two variables to determine the effect of these two variables on FMD.
Confounding variables and flow-mediated dilation value.

ACEI/ARB, angiotensin converting enzyme inhibitor / angiotensin receptor blocker; LDL, low-density lipoprotein; SNP c.521T>C, single nucleotide polymorphism c.521T>C; OR, odds ratio.
Analyzed with logistic regression (α < 0.05; p = 0.002; Adj. R2 = 0.521).
Effect of SBP characteristics and duration of simvastatin therapy on the results of measurement of FMD
Logistic regression was used to perform an analysis of the relationship between SBP and the duration of simvastatin therapy. This analysis aims to eliminate SBP and the duration of simvastatin therapy as confounding variables that do not have a high significance. The value of logistic regression analysis results showed Adjusted R2 = 0.442 (α < 0.05; p = 0.002) (Table 4). These concluded that these two confounding variables affect the measurement results of the FMD value.
Effect of systolic blood pressure and duration of simvastatin therapy to flow-mediated dilation.
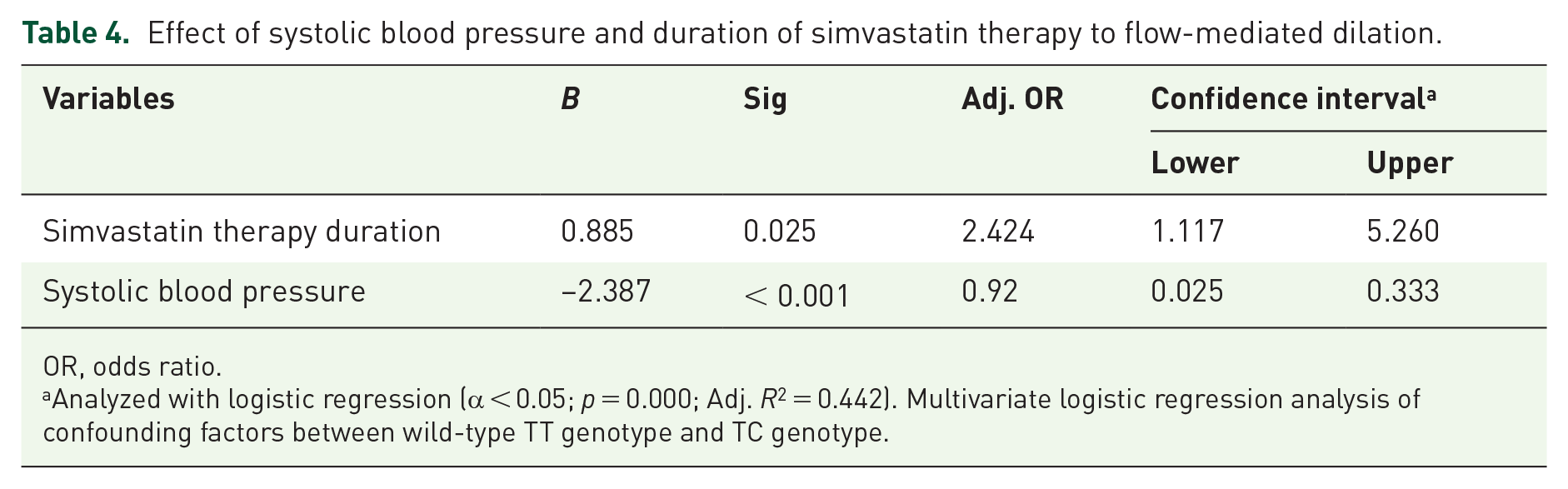
OR, odds ratio.
Analyzed with logistic regression (α < 0.05; p = 0.000; Adj. R2 = 0.442). Multivariate logistic regression analysis of confounding factors between wild-type TT genotype and TC genotype.
Discussion
Hypercholesterolemia is a major cardiovascular risk factor related to atherosclerosis. Atherosclerosis, as the main pathological process that causes CHD, is caused by deposits of LDL cholesterol in the walls of blood vessels which results in plaque formation.1,3 Every 1 mmol/L (40 mg/dL) reduction in LDL cholesterol is associated with a 22% reduction in cardiovascular mortality and morbidity. 17 Arterial endothelial dysfunction that may occur before structural changes of atherosclerosis is one of the essential factors in atherogenic processes.3,18 The change in arterial diameter may be caused by endothelial vasoactive mediators induced by the shear-stress process. This response is mediated mainly by endothelial nitric oxide (NO) released, where this response can be inhibited by the pre-medication of nitric oxide synthase (NOS) inhibitors. 19
Simvastatin is in the form of a pro-drug, which is then metabolized to the active form of simvastatin acid, either through hydrolysis of carboxylesterase in the intestine or by the cytochrome-P450 3A4 (CYP3A4) isoenzyme in the liver. 20 This form of simvastatin acid is the active form that can inhibit cholesterol synthesis and reduce CVD risk. 7 Genetic polymorphism in simvastatin resistance can also affect the pleiotropic effect of simvastatin. The variations in statin response can be influenced by gene polymorphisms that affect the pharmacokinetics and pharmacodynamics of statins. Statin resistance due to gene polymorphisms is related to differences in absorption, transport, intra-hepatic metabolism, metabolism in other organs, and mechanisms of statin elimination. 20
In 2018, Peyser et al have performed the first prospective randomized SLCO1B1 genotype-guided study for statin reinitiation. Although they failed to show that genotyping improved statin adherence, they did show that genotyping led to a greater number of patients reinitiated on statins and meaningful improvements in LDL-C levels. Until now, there are many literatures to discuss prespecified end points. However, to our knowledge, our research is the pilot study to compare SLCO1B1 genetic polymorphism with FMD as one of the pleiotropic effects of statins. Pleiotropic effects of statins include improvement of endothelial dysfunction, increased nitric oxide bioavailability, antioxidant properties, inhibition of inflammatory responses, and stabilization of atherosclerotic plaques.
From our study, a total of 9.9% of study participants with SNP c521T>C were identified in this study. However, analysis by χ2 test showed no association between the c.521T>C SNP of the SLCO1B1 gene and simvastatin pleiotropic function as measured by FMD endothelial function parameters. Similarly, descriptive analysis of the characteristics of the research participants stated that there were no differences between age, sex, ethnicity, history of hypertension, use of antihypertensive agents, body mass index, and LDL levels with low, normal, or high FMD values.
However, two variables of research participant characteristics are significantly different in each FMD group. Based on this, logistic regression analysis was then carried out to determine the effect of confounding variables on the FMD value. The logistic regression results of 15 independent variables showed that these variables could affect the dependent variable of FMD by 52.1% (α < 0.05; p = 0.002) with the highest significance values owned by the variables of simvastatin therapy duration and SBP. The following analysis was again carried out to determine the two variables that had the most significant influence. The second logistic regression results found that although it did not include other possible confounding variables, the independent variables SBP and duration of simvastatin could still affect the measurement results of the dependent variable FMD by 44.2% (α < 0.05; p = 0.002). Based on this, it can be concluded that the two variables have the most significant influence on measuring the FMD value in this study.
Gokce et al. study stated that higher SBP was an independent predictor of low FMD scores. 13 This is following this study with a negative effect between SBP and FMD values (B = –2.387; p < 0.001; Adj. OR = 0.92; CI = 0.025–0.333). The exciting thing is that a different relationship was found in the variables of history of hypertension and the administration of antihypertensive therapy. The two variables in the logistic regression analysis did not significantly affect the measurement of FMD values. The researcher assumed this could be caused by adherence to antihypertensive therapy, angiotensin converting enzyme inhibitor/ angiotensin receptor blocker, beta blockers, calcium channel blocker, and diuretics not homogeneous between the two groups of research participants.
The second variable that influences the FMD value is the duration of simvastatin therapy. There is a positive effect between the duration of simvastatin therapy and the FMD value (B = 0.885; Adj. OR = 2.424; p = 0.025; CI = 1.117–5.260). The same effect did not accompany this relationship as the LDL-level variable. LDL levels in this study did not affect the results of FMD measurements. This follows the theoretical reference, which states that the pleiotropic function of simvastatin is independent of cholesterol reduction. Improvement of endothelial function as measured by FMD parameters in this study is one part of the pleiotropic function of simvastatin. 21
After statin administration, improvements in endothelial function generally begin to appear before LDL-lowering targets are achieved. However, in various studies, the duration from the start of statin therapy to the improvement of endothelial function was different for each type of statin. High-intensity atorvastatin, for example, has shown improvement in vasodilation 39 days after administration of atorvastatin 80 mg/day. In contrast, improvements in vasodilation with simvastatin have only been seen after 1 month and are getting greater within 3 months after administering simvastatin 20 mg/day. 21
Although in the analysis of this study, there was a limitation in regard to the effect between the duration of simvastatin therapy on FMD values, a small number of participants showed low FMD values after simvastatin administration for a longer time. In addition, the majority of LDL data in this study were still above the expected optimal level even though most of them had received simvastatin therapy for a long time. Based on this, the researcher assumes a level of adherence to therapy that is not homogeneous between research participants. Also, the number of the study participants is quite small which may affect or bias the results, and difficulty to conclude in the larger population.
The variable dose of simvastatin in this study was homogeneous at 20 mg. No further analysis was carried out on the effect of different doses on the measurement of FMD. Another variable that has not been included in this study is a high-fat or high-arginine diet for a long period. Dietary factors high in arginine affect the formation of vasodilator NO. In addition, a high-fat diet is also associated with an increase in the speed of cholesterol synthesis by the HMGcR enzyme in the liver so that it can affect the measurement of LDL levels.22,23
Conclusion
It was concluded that there was no association between the SNP c.521T>C of the SLCO1B1 gene and the pleiotropic effect of simvastatin as measured by FMD of endothelial function parameters in hypercholesterolemic patients receiving simvastatin therapy.