
Abstract
Atherosclerotic cardiovascular disease (ASCVD) is a common disease among the general population, and includes four major areas: (1) coronary heart disease (CHD), manifested by stable angina, unstable angina, myocardial infarction (MI), heart failure, and coronary death; (2) cerebrovascular disease, manifested by transient ischemia attack and stroke; (3) peripheral vascular disease, manifested by claudication and critical limb ischemia; and (4) aortic atherosclerosis and aortic aneurysm (thoracic and abdominal). CHD remains the leading cause of death for both men and women in the United States. So, it is imperative to identify people at risk of CHD and provide appropriate medical treatment or intervention to prevent serious complications and outcomes including sudden cardiac death. Coronary artery calcification (CAC) is a marker of subclinical coronary artery disease. Therefore, coronary artery calcium score is an important screening method for Coronary artery disease (CAD). In this article, we performed a comprehensive review of current literatures and studies assessing the prognostic value of CAC for future cardiovascular disease (CVD) events. We searched PubMed, MEDLINE, Google Scholar, and Cochrane library. We also reviewed the 2018 American College of Cardiology (ACC)/American Heart Association (AHA) guideline on the assessment of CVD risk. A CAC score of zero corresponds to very low CVD event rates (∼1% per year) and hence a potent negative risk marker. This has been referred to as the ‘power of zero’ and affords the lowest risk of any method of risk calculation. It is now indicated in the 2018 ACC/AHA Cholesterol guidelines to be used to avoid statins for 5–10 years after a score of zero, and then re-assess the patient.
Introduction
In the United States, over 16.5 million people suffer from coronary heart disease (CHD), and the cost of care for these patients exceeds $300 billion per year. Despite great advances in treatment, CHD remains one of the leading causes of death in the United States for both sexes; with approximately 25% of these deaths occurring suddenly. 1
CHD risk factors include elevated LDL (low-density lipoprotein), cigarette smoking, diabetes mellitus, hypertension, family history of premature CHD, obesity, older age, male sex, post menopausal, sedentary life style, low HDL (high-density lipoprotein), metabolic syndrome, rheumatologic diseases (such as rheumatoid arthritis, systemic lupus erythematosus, and psoriasis), high levels of fibrinogen and coagulation factor VII, anemia, high levels of lipoprotein(a), microalbuminuria, mediastinal radiation, psychosocial factors, depression, and genetics which contribute to 40–60% of the cases.2,3
Atherosclerosis is responsible for almost all cases of CHD. This pathological process starts with fatty streaks that progress overtime and culminate in thrombotic occlusions and coronary events. Several risk assessment systems are used for determining the risk of CHD (Table 1). It is mainly based on age, sex, diabetes mellitus, total cholesterol, HDL cholesterol, tobacco smoking, and systolic blood pressure (SBP).4,5
Different ASCVD risk assessment systems.
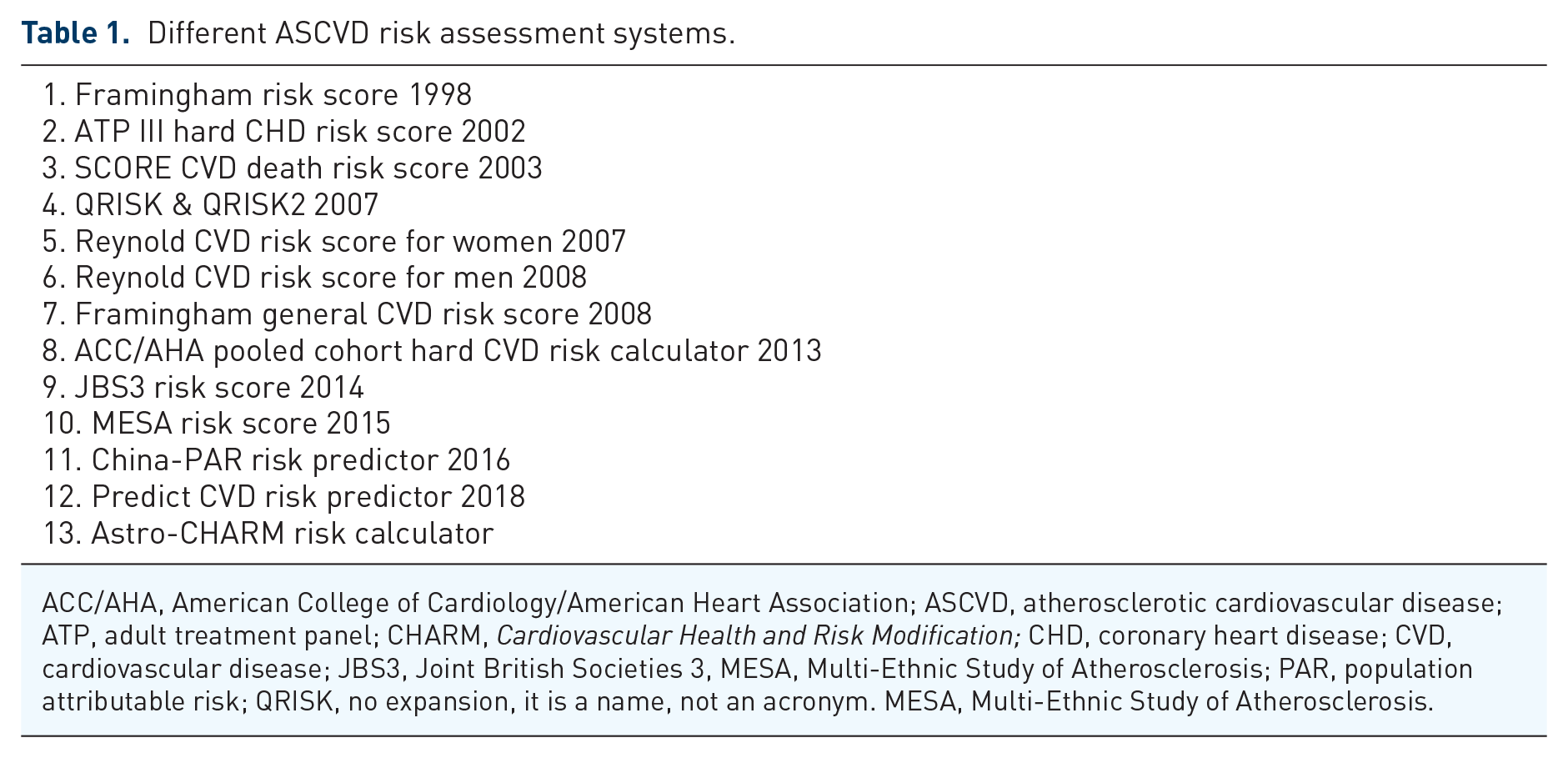
ACC/AHA, American College of Cardiology/American Heart Association; ASCVD, atherosclerotic cardiovascular disease; ATP, adult treatment panel; CHARM, Cardiovascular Health and Risk Modification; CHD, coronary heart disease; CVD, cardiovascular disease; JBS3, Joint British Societies 3, MESA, Multi-Ethnic Study of Atherosclerosis; PAR, population attributable risk; QRISK, no expansion, it is a name, not an acronym. MESA, Multi-Ethnic Study of Atherosclerosis.
Coronary artery calcification (CAC) is a marker of subclinical atherosclerosis. CAC implies a measure of atherosclerotic plaque burden regardless of traditional risk factors and is a strong predictor of atherosclerotic cardiovascular disease (ASCVD) events. 6
The aim of this study is to review the literature on assessing CAC to improving risk assessment in intermediate-risk asymptomatic population after formal risk assessment, and using the coronary artery calcium score to guide Aspirin/statin therapy.
Discussion
ASCVD risk assessment
Cardiovascular disease (CVD) risk assessment is an important screening method for primary prevention to guide preventive/therapeutic measures. The first step in assessing CVD risk is to determine the presence of the traditional risk factors (hyperlipidemia, hypertension, diabetes mellitus, cigarette smoking, premature family history of CVD, Obesity, etc.). The second step is to estimate CVD risk using a risk calculator. Many risk models have been developed to estimate the risk of CVD in healthy, asymptomatic individuals (Table 1). Each risk calculator is used based on patient-specific characteristics (e.g. age, sex, ethnicity).7–9
The 2013 ACC/AHA ASCVD risk estimator
The 2013 American College of Cardiology/American Heart Association (ACC/AHA) pooled cohort hard CVD risk calculator was developed to estimate ASCVD risk and guide statin therapy. It provides sex- and race-specific estimates of the 10-year risk of ASCVD for non-Hispanic African American and White men and women 40–79 years of age. The included variables for the pooled cohort equations are age, sex, total cholesterol, HDL cholesterol, systolic BP, diabetes mellitus, and current smoking status. As decision for statin therapy is based on individual’s absolute risk, risk assessment models should have good calibration (accurately estimates the absolute observed risk level) and discrimination (whether individuals with higher predicted risk are more likely to have events) to effectively balance the risks and benefits of statin therapy for primary prevention.7,10,11
However, three external validation cohorts – the Women’s Health Study, Physician’s Health Study, and Women’s Health Initiative Observational Study – were performed to evaluate the calibration and discrimination of these equations for predicting ASCVD risk, and concluded that ACC/AHA Pooled Cohorts risk equations over-estimate ASCVD risk.11,12
Overestimation of ASCVD risk has also been noted in the Multi-Ethnic Study of Atherosclerosis (MESA),
8
short-term follow-up of the REGARDS (REasons for Geographic and Racial Differences in Stroke) study by Muntner et al.,
11
and Rotterdam study cohort.
13
A large, multiethnic population study by Rana et al.,
14
to estimate the accuracy of the ACC/AHA Pooled Cohort risk equation, concluded that the risk equation substantially overestimated actual 5-year risk. Rana et al. reported, In each 5-year predicted ASCVD risk category, observed ASCVD risk at 5 years was substantially lower: 0.20% for predicted risk less than 2.50%; 0.65% for predicted risk 2.50% to less than 3.75%; 0.90% for predicted risk 3.75% to less than 5.00%; and 1.85% for predicted risk greater than 5.00% (C statistic: 0.74).
The estimated rates were approximately 5 times the observed rate, leading to gross overestimation of risk with this risk calculator in a population of over 300,000 persons without diabetes. Cook and Ridker, 15 reported in women’s health study (WHS) that use of statin, percutaneous coronary intervention (PCI), or under-ascertainment of events do not explain the discrepancy between observed rates of ASCVD and those predicted by the ACC/AHA pooled cohort equations.
Coronary artery calcium score (CAC score)
Technical aspect and history
Coronary artery calcium scoring (CAC) is a method used to calculate the amount of calcium in the coronary arteries using electrocardiogram (ECG) gated non-contrast computed tomography (CT) scan of the heart. It is quick (less than 10 s), minimal radiation exposure (less than 1 mSv), and does not require special preparation or intravenous contrast. CAC was first studied by fluoroscopy in the late 1950s. Electron beam computed tomographic scanning (EBCT), so-called ‘ultrafast CT’ was developed in 1980s allowing noninvasive and quantitative detection of CAC. The most widely used measure of CAC is the Agatston score. 16 Advancement of the temporal and spatial resolution of multi-detector row or multi-slice CT scanners (MDCT or MSCT) has improved cardiac imaging quality with no or little motion artifact. MDCT is considered state-of-the-art and most studies of Coronary artery calcium (CAC) is performed with this technology allowing for imaging with <1 millisievert and widespread adoption. 17
Refinement of ASCVD risk estimation
Global risk estimation equations including 2013 ACC/AHA pooled cohort equations are based on traditional risk factors. However, CAC directly measures the disease (coronary atherosclerosis burden), and yields a superior and potent risk marker. CAC can be used to upgrade ASCVD risk in younger and middle-aged patients with greater than 75% of age-, sex-, and race/ethnicity predicted CAC. Similarly, CAC can be potentially used for downgrading or de-risking patients with CAC-0 who are otherwise recommended for statin therapy based on risk estimation, or uncertain about decisions related to CAC. A CAC score of zero corresponds to very low CVD event rates (∼1% per year) and hence a potent negative risk marker.18–20 This has been referred to as the ‘power of zero’ and affords the lowest risk of any method of risk calculation. It is now indicated in the 2018 ACC/AHA Cholesterol guidelines to be used to avoid statins for 5–10 years after a score of zero, and then re-assess the patient.
Association of coronary artery calcium with ASCVD: prediction of CVD events and mortality
The presence and extent of CAC is considered a marker of overall burden of coronary atherosclerosis. Several studies have established a direct relationship between CAC score and histologic, intracoronary ultrasonic, and angiographic measures of coronary artery atherosclerosis and plaque burden.21–25
In a large MESA Cohort study by Detrano et al., 26 6722 men and women (38.6% White, 27.6% Black, 21.9% Hispanic, and 11.9% Chinese) with no clinical CVD had a coronary calcium scanning and were followed for a median of 3.8 years. The results showed 162 coronary events. In this study, it was reported that those with coronary calcium scores between 101 and 300 had a 7.73-fold increased risk of coronary events, and those with Calcium scores above 300 had an increased risk by a factor of 9.67 in comparison with participants with no coronary calcium (p < 0.001 for both comparisons). It was also noted that for each doubling of the calcium score, there was a 15–35% increase in the risk of a major coronary event. The study concluded that the CAC score strongly predicts incident CHD and provides incremental predictive information beyond that provided by cardiovascular risk factors. 26
A study by Yeboah et al., 27 in the MESA, compared improvement in prediction of CVD of six risk markers [CAC, brachial flow–mediated dilation (FMD), carotid intima–media thickness (CIMT), high-sensitivity C-reactive protein (hs-CRP), ankle-brachial index (ABI), and family history of CHD (FH)] in participants at intermediate-risk (Framingham Risk Scores (FRS >5%–<20%). In this study, 1330 of 6814 MESA participants without diabetes mellitus who had intermediate risk (FRS >5%–<20%) and had complete data on all six of the novel risk markers were enrolled and followed for a median of 7.6 years. CAC, ABI, hs-CRP, and FH were independently associated with incident CHD in multivariable analyses [hazard ratio (HR), 95% confidence interval (CI): 2.60 (1.94–3.50), 0.79 (0.66–0.95), 1.28 (1.00–1.64), and 2.18 (1.38–3.42), respectively]. CAC afforded the highest increment (0.623 versus 0.784), and for incident CHD, the net reclassification index (NRI) with CAC was 0.659, FMD 0.024, ABI 0.036, CIMT 0.102, FH 0.160, and hs-CRP 0.079. The study concluded that coronary artery calcium provided superior discrimination and risk reclassification within intermediate-risk individuals compared with other risk markers. Many other studies have shown that coronary calcification is a strong predictive of coronary events independent of standard risk factors.28–40
Kavousi et al. 41 evaluated and compared newer risk markers for CHD risk classification (CAC, the N-terminal fragment of prohormone B-type natriuretic peptide, uric acid levels, Von Willebrand factor antigen, chronic kidney disease, fibrinogen levels, homocysteine levels, hs-CRP, leukocyte count, peripheral arterial disease, CIMT, and pulse wave velocity) to the FRS. Kavousi et al. found that adding CAC scores to the FRS improved the accuracy of risk predictions [c-statistic increase, 0.05 (95% CI: 0.02–0.06); net reclassification index, 19.3% overall (39.3% in those at intermediate risk, by FRS)]. The study concluded that CAC provided the highest increment in area under the curve (AUC) and NRI over the FRS.
Using coronary artery calcium score to guide statin therapy
A score of zero (absence of CAC) has been shown to be associated with a very low cardiovascular event rate in asymptomatic populations, leading to de-escalation of both aspirin and statin therapy. Multiple studies have documented the low risk and low event rates in persons with zero scores. Taylor et al., 36 Budoff et al., 42 and Detrano et al. 26 reported event rate of 0.6/1000 person-years in patients with CAC-0. Whereas Arad et al. 34 reported an event rate equivalent to 1/1000 person-years, Raggi et al. 32 reported an event rate equivalent to 1.1 events/1000 person-years, Shaw et al. 39 reported event rate of 1.5 events/1000 person-years, and LaMonte et al. 38 reported 1.6 events/1000 person-years.
Conversely, the presence and severity of CAC can identify patients most likely to benefit from statin for the primary prevention of ASCVD. 43 Individuals with CAC = zero have very low risk for ASCVD morbidity and mortality for up to 15 years. Whereas individuals with CAC > 100 have a risk for a first ASCVD event nearly equivalent to a recurrent event in patients with established ASCVD (secondary prevention). So, measuring CAC score can help identify and risk stratify individuals with CAC = 0 to avoid overtreatment and those with CAC > 100 to avoid undertreatment.44–47
Evidence from randomized control trials (RCTs) of statin therapy for primary prevention supports the use of statins in all men and women above 55 years of age, which will lead to lower compliance in asymptomatic patients and increase health care costs. However, almost 50% of those who are statin-eligible based on RCTs had CAC = 0 and a very low event rate (can defer statin and aspirin for 5 years), and one-fourth had CAC > 100 and a high event rate. Thus, CAC can provide better risk stratification and match risk with intensity of therapy, which ultimately improves overall individual compliance and decreases health care costs. 47
In the St. Francis Heart Study Randomized Clinical Trial (randomized double-blind placebo controlled trial of atorvastatin in the prevention of cardiovascular events among individuals with elevated CAC score) by Arad et al., 34 a total of 1005 healthy men and women age 50–70 years with elevated CAC were studied. A total of 490 received 20 mg atorvastatin and 515 received placebo, with mean treatment of 4.3 years. Atorvastatin treatment reduced clinical endpoints by 30% (from 9.9% to 6.9%, absolute benefit 3% or number needed to treat of only 33), and myocardial infarction (MI) and death by 44% (number needed to treat (NNT) 30). Event rates were more significantly reduced in participants with baseline CAC scores of >400 (8.7% versus 15.0%, p = 0.046 (resulting in a 42% reduction with a number needed to treat of 16. 34
Mitchell et al. 43 reported in a retrospective analysis of Walter Reed cohort that CAC score >100 was associated with a greater reduction in major adverse cardiovascular event (MACE) with statin therapy. Subsequently, CAC score >100 is considered the cut-off point to choose patients with the greatest benefit from statin therapy. More importantly, he demonstrated that there was absolutely no benefit to treating patients with a statin. In his study of 13,644 patients (average age 50 years; including 71% men, with median follow-up of 9.4 years), Mitchell et al. demonstrated statin therapy was associated with reduction in the risk of MACE for those patients with CAC (subhazard ratio: 0.76; with 95% CI: 0.60–0.95; p = 0.015). There was no benefit in those without CAC (subhazard ratio: 1.00; 95% CI: 0.79–1.27; p = 0.99). The greater the severity of CAC, the greater the benefit of statin use on MACE (p < 0.0001). The NNT to prevent one MACE outcome over a decade ranged from infinity (CAC of zero) to 100 (CAC 1–100) to 12 (CAC >100). This observational study strongly supports the ACC/AHA Guidelines which call for deferred statin use in scores of zero, consideration of higher risk patients with CAC 1–99, and use of statins in persons with scores >100.
Using coronary artery calcium score to guide aspirin therapy
Aspirin use in primary prevention of CVD is recommended to be limited to high-risk individuals. Clinical trials had shown that aspirin use in low-risk individuals will decrease CVD events rate, but cause equivalent increase in bleeding risk. Practically, liberal use of aspirin would include treatment of low-risk populations resulting in small benefit outweighed by high bleeding risk, while limiting aspirin use to high-risk populations would likely abrogate the chance to prevent significant number of CVD events.48–52 Therefore, it is important to identify individuals with the most favorable risk/benefit outcome by improving ASCVD risk assessment. CAC score measures total atherosclerotic plaque burden in the coronaries and can provide a significant improvement in net risk reclassification.
Miedema et al. 53 studied Aspirin risk and benefit based on CAC score using data from large MESA study. The study reports patients with CAC > 100; FRS < 10%, NNT was 173, FRS > 10%, NNT was 92. While patients with CAC = 0, FRS > 10%, NNT was 808, recommending that patients with CAC > 100 will benefit from aspirin.
Using coronary artery calcium score to guide initiation and intensification of antihypertensive therapy
In 2014, the eighth panel appointed to the Joint National Committee on Detection, Evaluation, and Treatment of High Blood Pressure (JNC-8) recommended initiation of treatment for hypertension when blood pressure ⩾ 150 mm Hg in adults 60 years of age, who are non-diabetic or with no chronic kidney disease. 54 However, Systolic Blood Pressure Intervention Trial (SPRINT) reported there is significant improvements in both ASCVD and heart failure in hypertensive populations when treatment target is 120 mm Hg instead of standard target of 140 mm Hg. 55 Karmali et al. 56 reported high ASCVD events in individuals with BP levels considered at goal by JNC-8, and majority of them were individuals with high ASCVD risk. Many studies have proposed the use of ASCVD risk estimates to guide treatment decisions for hypertension to avoid overtreatment in low-risk populations and intensifying treatment in high-risk population. CAC is a powerful predictor of ASCVD risk and can provide a prognostic value to risk estimates.57–60
McEvoy et al. 61 reported combined CAC and ASCVD risk assessment can guide SBP goals (standard goal of 140 or intensive goal of 120 mm Hg), especially among individuals with ASCVD risk 5–15% and pre-hypertension or mild hypertension. McEvoy reported that ASCVD risk < 15% and SBP of either 120–139 or 140–159 mm Hg has increasing HRs for events with CAC 1–100 [1.7 (95% CI: 1.0–2.6) or 2.0 (1.1–3.8)] and CAC > 100 [3.0 (1.8–5.0) or 5.7 (2.9–11.0)]. NNT10 was 99 for CAC = 0 and 24 for CAC > 100, when SBP was 120–139 mm Hg.
Does CAC scanning improve ASCVD outcomes?
The presence and severity of CAC in young individuals without cardiovascular risk factors is strongly and independently associated with MACE events (MI, stroke, and cardiovascular death) and mortality. CAC scoring may significantly improve the assessment of individual ASCVD risk and guide the application of preventive therapies. 62
The EISNER (Early Identification of Subclinical Atherosclerosis by Noninvasive Imaging Research) Prospective Randomized Trial by Rozanski et al. showed that CAC score may effectively triage care – evaluation and intensification of therapy – without increasing cost. In this study, compared with the group who did not undergo scanning, the scan group demonstrated a favorable change in blood pressure (p = 0.02), waist circumference (p = 0.01), LDL cholesterol (p = 0.04), and weight loss among overweight subjects (p = 0.07). There was an improvement of FRS compared with no scan group. 63
When to repeat CAC testing?
If the initial CAC score is zero, it is reasonable to repeat the scan 5 years after the initial scan if the statin therapy decision remains uncertain. However, the scan can be repeated sooner in smokers, diabetic patients, and patients with peripheral vascular disease due to rapid progression of atherosclerosis in those patients, and progression of CAC has been demonstrated to independently predict future ASCVD events.30,42,64,65
Test cost, radiation, and limitations
CAC testing does not require especial preparation or intravenous contrast. Time acquisition is usually less than 10 s. It costs $75 to $100 in the United States. The radiation exposure is minimal, < 1 mSv per scan, and equivalent to the dose and cost of a screening mammogram. 66 Because CAC cannot provide information about noncalcified plaque or severity of coronary stenosis, it cannot be utilized to evaluate patients with acute chest pain concerning for ischemic heart disease, but has been shown to risk stratify patients with stable chest pain syndromes. 67
CAC in 2018 ACC/AHA guidelines
The 2018 ACC/AHA Guidelines on the Management of Blood Cholesterol states, In adults 40 to 75 years of age without diabetes mellitus and with LDL-C levels ⩾70 mg/dl-89 mg/dl (⩾1.8–4.9 mmol/L), at a 10-year ASCVD risk of ⩾7.5%-19.9%, if a decision about statin therapy is uncertain, consider measuring CAC. If the CAC score is zero, treatment with statin therapy may be withheld or delayed, except in cigarette smokers, those with diabetes mellitus, and those with a strong family history of premature ASCVD. A CAC score of 1-99 favors statin therapy, especially in those > 55 years of age. For any patient, if the CAC score is ⩾100 Agatston units or ⩾75th percentile, statin therapy is indicated unless otherwise deferred by the outcome of clinician–patient risk discussion (Class IIa).
68
Conclusion
ASCVD is a major cause of morbidity and mortality. The 2013 ACC/AHA pooled cohort hard CVD risk calculator as a screening tool had shown overestimation of CVD risk. CAC is an established marker of subclinical coronary atherosclerosis. CAC is pathognomonic of coronary atherosclerosis and represents a reliable anatomic estimate of plaque burden.
CAC can be measured by CAC scoring and help risk stratify intermediate-risk population and guide Aspirin/Statin therapy for better adherence and cost-effective therapy, that is, CAC = 0 (don’t treat) or CAC > 100 (treat and ensure long-term adherence).
CAC score of 0 is a negative risk factor in intermediate-risk asymptomatic individuals, allowing for de-risking of the patient and less therapies.
Footnotes
Author contributions
Ahmed M. Shafter, Kashif Shaikh, Amit Johanis and Matthew J. Budoff all contributed by writing the article. Dr Budoff is responsible for the final version and editing
Conflict of interest statement
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Budoff reports grant support from General Electric. No other author has a conflict of interest.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.