
Abstract
Background:
Adherence to treatment after a myocardial infarction (MI) is poor, even in the early postinfarction period. Combining evidence-based drugs into a multicap could improve adherence in this population. No previous randomized trial assessing fixed-dose combination therapy has included patients early after a MI. We aimed to assess if a multicap containing four secondary prevention drugs increases adherence to treatment at 6 months after MI hospitalization. The study was designed as a randomized, parallel, open-label, controlled trial.
Methods:
Patients were randomized within 7 days of a MI to either multicap or control group. The multicap group received a capsule containing aspirin, atenolol, ramipril, and simvastatin. The control group received each drug in separate pills. The primary outcome was adherence at 6 months. We also measured blood pressure, heart rate, serum cholesterol levels, C-reactive protein, and platelet aggregation.
Results:
The study was stopped prematurely when 100 patients were included for futility. At 6 months, 92 (95.8%) patients were adherent to medical treatment: 98.0% in the multicap group and 93.5% in the control group [relative risk (RR) 1.05; 95% confidence interval (CI) 0.96–1.14; p = 0.347].
There were no differences between groups in systolic blood pressure (p = 0.662), diastolic blood pressure (p = 0.784), heart rate (p = 0.533), total cholesterol (p = 0.760), LDL-c (p = 0.979), C-reactive protein (p = 0.399), or in the proportion of patients with adequate platelet aggregation inhibition (p = 0.600).
Conclusions:
The study did not find any improvement in the adherence at 6 months after a MI with a multicap-based strategy (Multicap for Increase Adherence After Acute Myocardial Infarction; [ClinicalTrials.gov identifier: NCT02271178]).
Keywords
Introduction
Patients surviving myocardial infarction (MI) are at high risk of recurrent cardiovascular events and death, and the closer the initial event, the higher the risk. 1 Secondary prevention therapy with statins, β-blockers, angiotensin-converting enzyme (ACE) inhibitors, and aspirin have been shown to substantially reduce recurrent events and mortality after an acute coronary event.2–5 Notwithstanding the overwhelming evidence supporting secondary prevention therapy, globally, more than half of patients with coronary heart disease do not take any preventive drug. 6 One of the reasons cited to explain this underuse of evidence-based drugs is low patient adherence to the prescribed medication regimen. 7
Poor adherence to secondary prevention therapies among patients discharged from hospitals after a MI has been associated with a higher risk of recurrent coronary events and mortality, and it also increases health care system costs.7–9 Consequently, enhancing adherence to secondary prevention therapy after a MI has the potential to improve clinical outcomes and to affect favorably health care-related costs (even in low- and middle-income settings where yearly health-care expenditure per head is low). 10
Several factors have been described that influence adherence to therapy, including socioeconomic-, patient-, condition-, treatment-, provider-, system-, and setting-related factors. 11 Among treatment-related factors, the complexity of the therapeutic regimen (several drugs or many daily doses) has been associated inversely with adherence.12,13 Polypills, which contain a combination of preventive drugs in only one pill, have shown to increase adherence to therapy among patients with a history of cardiovascular disease or at high risk of cardiovascular events. Since no trial has evaluated the effectiveness of this therapy in patients with a recent MI, the effects in this population are not known.14,15
We aimed to assess whether a simplified regimen using a once daily multicap (a single capsule containing aspirin, a β-blocker, an ACE inhibitor, and a statin) as compared with a regimen with each of these drugs in a separate pill, increases adherence at 6 months after a MI hospitalization in a tertiary referral public hospital in a suburban area of Buenos Aires province, Argentina.
Materials and methods
We conducted a randomized, controlled, parallel-group, open-label, single center, clinical trial to test the hypothesis that a simplified therapeutic regimen with one-a-day multicap could increase adherence after a MI. All patients gave written informed consent to participate, and the protocol was approved by the Institutional Review Board and Ethics Committee. The study was designed by the investigators, and the hospital purchased all the study drugs. All authors had full access to the data and made the final decision for publication. The study is registered with ClinicalTrials.gov (identifier NCT02271178).
Patients and randomization
The study population included patients >18 years, with a MI within the previous 7 days, defined as ischemic chest pain associated with electrocardiogram abnormalities (ST elevation or depression, T wave inversion, or new left bundle block) and troponin elevation. Exclusion criteria were left ventricular ejection fraction (LVEF) <40%, contraindication for aspirin, β-blockers, ACE inhibitors or statins, chronic treatment with nonsteroidal anti-inflammatory agents, planned coronary revascularization within 6 months after discharge (surgery or percutaneous coronary intervention), severe chronic kidney disease (estimated creatinine clearance <30 ml/min), hepatic insufficiency or persistently elevated transaminases (>3 times the upper normal limit), fasting serum triglyceride level >500 mg/dl, other non-atenolol based β-blocker therapy clinically appropriate according to physicians, oral anticoagulation, and inability to attend follow-up visits due to geographic reasons. Patients who met inclusion criteria and had none of the exclusion criteria were invited to participate and, after signing written informed consent, were randomized in a 1:1 ratio to multicap or control. Randomization was performed by telephone by administrative personnel not otherwise involved in the study, using a computer-generated randomization list with block sizes of 4 and 6, and stratification according to diabetes (present versus absent) and gender (female versus male). Randomization was done before hospital discharge for the qualifying MI.
Study procedures
Patients assigned to the multicap group received capsules containing aspirin (100 mg), atenolol (50 or 100 mg), ramipril (5 or 10 mg), and simvastatin (40 mg), to be taken once daily. Doses of atenolol and ramipril were individualized for each patient based on the doses of ACE inhibitors and β-blockers used during hospitalization for the index MI. Patients assigned to the control group received aspirin, atenolol, ramipril, and simvastatin given in separate pills, in once daily doses and packaged in blisters as per commercially available presentation (with no calendar reminder). Study medications were given to all participants free of charge and dispensed at every study visit.
Medications were titrated according to the following scheme for both groups: atenolol was uptitrated to 100 mg daily when given at 50 mg daily with ramipril at the maximum dose, only if the heart rate was >55 bpm and systolic blood pressure >100 mmHg; when ramipril was given at 5 mg daily (with atenolol at maximum dose), if systolic blood pressure was >100 mmHg, then the dose was uptitrated to 10 mg daily. When both atenolol and ramipril were at submaximal doses, uptitration was initiated with ramipril. The protocol allowed the dose of atenolol and ramipril to be reduced when symptomatic hypotension or bradycardia were suspected during follow-up visits.
The multicap pill was prepared in the hospital pharmacy according to a standardized procedure. For preparation of the multicap, each individual drug was placed in a hard gelatin capsule by pharmacists, and then stored in bottles with the supply for subsequent visits according to physician prescription. The control group received blister packs with separate pills for each drug. There was no repackaging of the pills for the control group, the main difference from the commercially available presentation was that the study medication for this group was given without the individual packaging for each drug.
Both patients and researchers were aware of the assigned group since the logistics resources required for blinding were not available at the time the study was planned.
Drugs and doses were selected considering national and international guidelines in force at the time the study was planned.16,17
Follow up
Follow-up visits were scheduled at 7 days, 1 month, 3 months, and 6 months. At each follow-up visit, patients were assessed clinically and were asked for potential adverse effects; whenever possible, the study medication was uptitrated. Electronic medical records were also checked to detect potentially missed adverse events. Pills that were not used were returned and counted. The drugs for the next period were then dispensed. Every medication supply included a quantity that exceeded the amount needed until the next visit, taking into account possible delays as prespecified in the protocol.
An electrocardiogram was obtained at the 3- and 6-month visits, and a final blood laboratory test was performed at 6 months, which included serum cholesterol levels, and, in a random sample (31 patients), platelet aggregometry to assess the aspirin effects. Platelet aggregometry was performed with an automated turbidimetric method in platelet-rich plasma using arachidonic acid (500 µg/ml) as an agonist (AggRAM system, Helena Laboratories, Beaumont, Texas, USA).
After each clinical evaluation, the updated medication according to protocol was provided to the patients by the study coordinator. Multicap capsules were prepared on the same day of the visit after follow-up evaluation. There was no stockpiling of multicaps.
Adherence evaluation
Adherence was evaluated using an indirect technique of pill counting. At each follow-up visit, returned pills were counted by an instructed nurse from the protocol. Adherence was measured by the percentage of pills that were missing from the package (as it was assumed they had been taken) of the total amount estimated for the period. In other words, the simplified equation adopted was
Outcomes
The primary outcome was the proportion of patients being adherent to medical therapy at 6 months, assessed by pill counting. Patients who did not attend follow-up visits, and those that permanently discontinued the study medication, were excluded from primary analysis, and were considered as nonadherents in a sensitivity analysis.
Secondary outcomes included blood pressure, heart rate, serum low density lipoprotein cholesterol level (LDL-c), C-reactive protein level (CRP), platelet aggregation, and incidence of adverse events during follow up. Discontinuation of study medication and potential adverse effects were also registered. Blood pressure and heart rate were measured at every follow-up visit, cholesterol and CRP levels were measured at baseline and at 6-month visit, and aggregometry was measured at 6-month visit.
Statistical analysis
It was estimated that 200 patients would give the study 80% power, at a type I error level of 0.05%, to detect a difference between groups of 25% absolute percentage points (from 40% to 65%) in the occurrence of the primary outcome. 18
Continuous variables are presented as means and standard deviations (SD); or median and interquartile ranges (IQR), as appropriate. Categorical data are presented as numbers and percentages. Normal assumption was tested using the Shapiro-Wilk test. Student’s t test and the Mann–Whitney U test were used to compare continuous data between groups, and Pearson’s Chi-square test and Fisher’s exact test were used for categorical data.
Primary outcome is presented as relative risk (RR) with the corresponding 95% confidence intervals (95% CI), and was compared between groups with the Fisher’s exact test. Between-groups differences in systolic blood pressure, diastolic blood pressure, heart rate, serum total cholesterol, serum LDL-c, and CRP (log-transformed) during follow up were analyzed fitting linear mixed-effect models. In these models, the study subjects were introduced as a random factor, and the study visits with outcome measurements (baseline, visit 1, visit 2, visit 3, and final visit for blood pressure and heart rate, and baseline and final visit for total cholesterol, LDL-c, and CRP) and assigned study group (multicap versus control), as fixed factors.19,20 All analyses are two-tailed and a p value < 0.05 was considered statistically significant.
Statistical analyses were conducted with the R statistical package version 3.3.2 for Mac OS X (The R Foundation for Statistical Computing Platform, Vienna, Austria).
Results
Patients
In September 2016, an interim analysis was conducted after inclusion of the first 100 patients. After the results were analyzed, the Institutional Review Board recommended to stop the study since both study groups had higher than expected good adherence rates and it was unlikely that any difference would be detected with the planned sample size. As a result, recruitment was stopped prematurely in September, and randomized patients were followed to complete the 6-month visits.
From April 2014 to September 2016, 236 patients were admitted to hospital with diagnosis of MI; of those, 224 were screened to participate (Figure 1). A total of 100 patients met the inclusion criteria and were randomized to multicap (n = 52) and control (n = 48). There were no losses to follow up for vital status; however, one patient did not return for the final visit and a family member was contacted for vital information.

Study flow.
Baseline characteristics of patients were balanced between groups (Table 1). Mean age was 53.7 (8.3) years and 60% were current smokers. Most MIs were with ST elevation (84%), 79.8% of them received reperfusion therapy and had preserved LVEF. Overall, 88% received P2Y12 inhibitor.
Baseline characteristics.

99 subjects with data.
97 subjects with data.
96 subjects with data.
BMI, body mass index; bpm, beats per minute; CRP, C-reactive protein; HDL-c, high density lipoprotein cholesterol; IQR, interquartile range; LDL-c, low density lipoprotein cholesterol; LVEF, left ventricular ejection fraction; MI, myocardial infarction; PTCA, percutaneous transluminal coronary angioplasty; SD, standard deviation.
Primary outcome
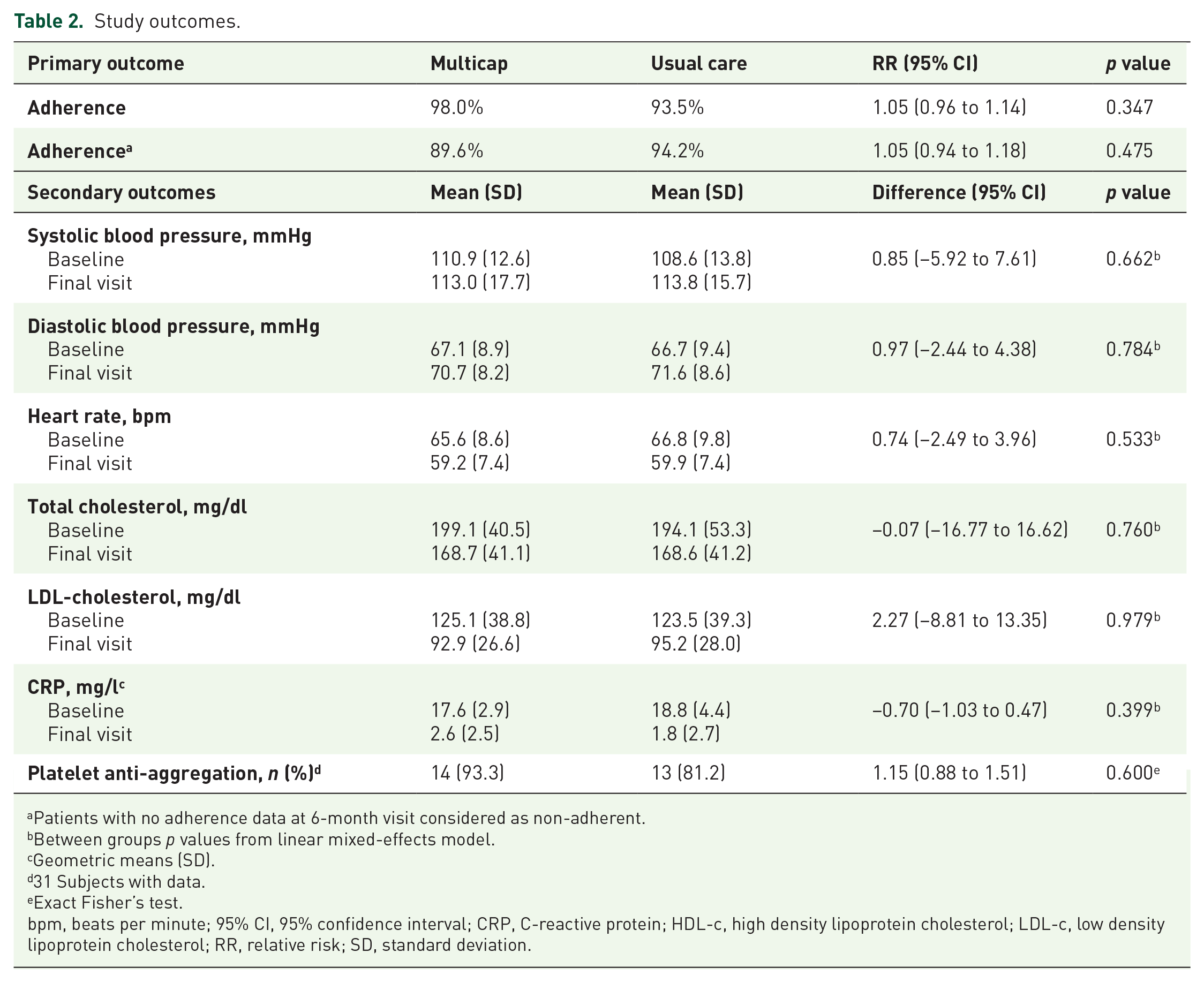
At the 6-month visit, 92 (95.8%) patients were adherent to medical treatment, 98.0% in the multicap group and 93.5% in the control group (RR 1.05; 95% CI 0.96–1.14; p = 0.347) (Table 2). Four patients discontinued study medication prematurely (two in each study group); considering them as nonadherent did not materially change the results (adherents 94.2% versus 89.6%, for multicap and control groups, respectively; RR 1.05; 95% CI 0.94–1.18; p = 0.475).
Study outcomes.
Patients with no adherence data at 6-month visit considered as non-adherent.
Between groups p values from linear mixed-effects model.
Geometric means (SD).
31 Subjects with data.
Exact Fisher’s test.
bpm, beats per minute; 95% CI, 95% confidence interval; CRP, C-reactive protein; HDL-c, high density lipoprotein cholesterol; LDL-c, low density lipoprotein cholesterol; RR, relative risk; SD, standard deviation.
Blood pressure, heart rate, cholesterol levels, and platelet aggregometry
Figure 2 shows systolic blood pressure, diastolic blood pressure, and heart rate during visits in each study group. Although some variation since randomization up to final visit was detected in these variables, there were no significant differences between groups (Table 2). Serum total cholesterol and LDL-c levels decreased significantly from baseline to the last visit in both groups, without significant differences between them. Also, the same pattern was observed in serum CRP levels (Supplemental table).

Blood pressure and heart rate during follow up.
Aggregometry was performed on a random sample of 31 patients (15 assigned to multicap and 16 to control) at the final follow-up visit. There were no significant differences between groups in the proportion of study participants, with adequate response to aspirin, 93.3% (14 patients) versus 81.2% (13 patients) for multicap and control, respectively (p = 0.599).
Adverse events and tolerance to the study medication
Two patients stopped the prescribed study medication prematurely after developing heart failure (one patient in each group). Two patients assigned to multicap were admitted to hospital with diagnosis of non-ST MI during follow up.
One patient in the control group stopped atenolol after visit 3 due to bradycardia (43 bpm). No other patient stopped the study medications for suspected adverse reactions. At final visit, 74.0% and 86.4% of patients assigned to multicap and control, respectively, were taking ramipril 10 mg/day (p = 0.218); and 62.0% and 64.4% of patients assigned to multicap and control, respectively, were taking atenolol 100 mg/day (p = 0.973).
Discussion
The results of our study suggest that a simplified secondary prevention therapy strategy with a multicap containing four drugs (aspirin, atenolol, ramipril, and simvastatin) does not significantly improve adherence at 6 months after a MI. This interpretation should be viewed with caution since the study was stopped prematurely and underpowered to detect small, but still clinically relevant, differences in adherence rates between groups.
Other studies that evaluated fixed-dose combination therapy strategies for secondary prevention showed significant improvements in adherence with this strategy. The UMPIRE (n = 2004), Kanyini GAP (n = 623), and IMPACT (n = 513) trials were part of the SPACE Collaboration, which evaluated the use of a polypill in different settings.14,21–23 All three studies enrolled participants with either established cardiovascular disease (coronary heart disease, ischemic cerebrovascular disease, or peripheral vascular disease) or a 5-year cardiovascular risk of 15%, who were randomized to polypill (two versions) or to usual care. Both individual trials and a meta-analysis (n = 3140 participants, 2046 with established coronary heart disease) showed that polypill improved adherence, defined by taking prescribed regimen for at least 4 days during the week preceding the study visit at 12 months (50% with usual care to 80% with the polypill; p < 0.001). The FOCUS trial enrolled 695 participants from Argentina, Paraguay, Italy, and Spain, with previous MI (mean 42.6 months from the event), and randomized to polypill (containing aspirin, simvastatin, and ramipril) or control. 15 Adherence at 9 months, defined as a Morinsky-Green medication questionnaire score of 20, and taking between 80% and 110% of pills that were prescribed to be taken (assessed by pill counting), was improved from 41.0% in the usual care group to 50.8% in the polypill group (p = 0.019). Differences in study design, populations, control group drug packaging presentation, methods to measure adherence to therapy, and follow-up duration could explain the differences with previous studies. In the UMPIRE trial, the polypill group received the study medication free of charge from trial centers, while the usual care group had to get from their practitioner, and, in some countries, had to purchase them 21 ; in the IMPACT and Kanyni GAP trials, patients had to make a copayment in both groups according to New Zealand and Australian regulations, but this was only one copayment for the polypill and one copayment for each medication in usual care group22,23; in the FOCUS trial all patients received medication free of charge. 15
In our control group, there was a higher than expected adherence rate, with little room for additional improvement. Several factors that have been shown to positively influence the use of secondary prevention medication were favorably affected by design in both groups of our study, and could have operated to increase adherence, particularly in a low income setting (as in our case): free-of-charge medication, ready access to health system facilities, short time elapsed between hospital discharge after MI and first follow-up visit, medical advice and effective communication with the medical team, and follow up by cardiologists.11,16,24–28 Also, the recentness of the MI could have been a factor that increased adherence to therapy.
Our study has several limitations that must be considered when interpreting the results. The premature termination could have affected our ability to detect a small, but still important, improvement in adherence; however, since the study was underpowered with the planned sample size, and it was not feasible to increase the sample size, we decided to follow the recommendation to stop the trial. Although it has been suggested that the chosen method to measure adherence has weaknesses because patients could discard pills in order to appear more adherent to treatment that they actually are, this strategy has practical advantages and reproduces what has been used in other polypill trials.7,14
Since the control group received individual pills packaged in blisters (with no calendar reminder) and there is evidence suggesting that this kind of packaging improves adherence in chronic conditions, it is possible that packaging increased adherence in the control group.29,30 Blister packaging is the most common commercial presentation of cardiovascular medications in Argentina; therefore, any benefit on adherence should be proved against this standard.
Usual care after MI in the setting where the study was conducted includes purchase of medication by the patient, and there are barriers to access to health care providers in the public system. It is likely that the study design influenced adherence by other multiple mechanisms since the medication was dispensed free of charge, the study visits were arranged and scheduled according patient possibilities/wishes, there were telephone reminders prior to visits, and there was facilitated access to a tertiary health care center whenever they had doubts or symptoms. On the other hand, the relatively short follow up of 6 months could be too short allow important differences in adherence between study groups to emerge. Finally, the open-label design in our, and other, trials could affect estimates of adherence in both groups, and these limitations should be considered in future trials.
It is possible that simplification of the secondary prevention therapy in both study groups (i.e. multicap and blister packaging, in multicap and control groups, respectively) enhanced adherence in both groups, and could bias the results toward the null. The control group had an unexpectedly higher adherence rate than previously reported; this observation may be the result of the study design, which included close follow up, access to health care and medication, blister packaging in the control group, and fluid communication with the heath care team. 18 Future studies should evaluate the effects of alternative strategies to improve adherence, particularly in low income settings, where application of evidence-based medicines after a MI is still poor. Also, other studies evaluating strategies to improve adherence to therapy in patients with recent MI might contemplate longer follow-up time, since adherence decreases as time passes from the qualifying event. 31
Our study evaluating a multicap found no additional effect on adherence to treatment at 6 months after a MI. The locally produced multicap, with individualized doses of atenolol and ramipril, proved to be biologically active and feasible since it carries very low additional costs.
Supplemental Material
Supplemental_Table_1 – Supplemental material for Multicap to improve adherence after acute coronary syndromes: results of a randomized controlled clinical trial
Supplemental material, Supplemental_Table_1 for Multicap to improve adherence after acute coronary syndromes: results of a randomized controlled clinical trial by Javier Mariani, Andrés Rosende, Maximiliano De Abreu, Gabriel Gonzalez Villa Monte, Heraldo D’Imperio, Laura Antonietti, Gabriela Lemonnier, Alejandra de Bonis and Carlos Tajer in Therapeutic Advances in Cardiovascular Disease
Footnotes
Acknowledgements
The authors thank Gloria Luna for her valuable collaboration and support during the study conduction.
Author contributions
JM and CT contributed to the conception and the design of the work. JM, AR, MDA, GGVM, HD’I, LA, GL, AdB, and CT contributed to the acquisition, analysis or interpretation of the data for the work. JM and CT drafted the manuscript. AR, MDA, GGVM, and HD’I critically revised the manuscript. All authors gave final approval and agree to be accountable for all aspects of work ensuring integrity and accuracy.
Authors’ Note
Gabriel Gonzalez Villa Monte is now affiliated to General Director of Teaching, Research and Professional development, Minitry of Health of Buenos Aires City, Ciudad Autónoma de Buenos Aires, Argentina.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.