
Abstract
Background:
Clopidogrel is by far the most prescribed platelet adenosine diphosphate (ADP) antagonist in Puerto Rico despite the advent of newer agents (prasugrel and ticagrelor). Given the paucity of data on clopidogrel responsiveness in Hispanics, we sought to determine the association between clinical characteristics and platelet reactivity in Puerto Rican patients on clopidogrel therapy.
Study population:
A total of 100 Puerto Rican patients on clopidogrel therapy were enrolled and allocated into two groups: Group I, without high on-treatment platelet reactivity (HTPR); and Group II, with HTPR. Platelet function was measured ex vivo using the VerifyNow® P2Y12 assay.
Results:
The cohort was comprised of Hispanic patients with coronary artery disease (57%), peripheral artery disease (32%), carotid artery stenosis (7%), cerebral artery aneurysm (2%), and stroke (2%). Mean platelet reactivity was 200 ± 61 P2Y12 reaction units (PRUs) (range: 8–324), and 35% of patients had HTPR (PRUs ⩾ 230). Multivariable logistic regression analysis determined that diabetes mellitus (DM) [odds ratio (OR) = 3.27; 95% confidence interval (CI): 1.20–8.96], use of proton-pump inhibitors (PPIs) (OR = 3.60; 95% CI: 1.09–11.82), and calcium channel blockers (CCBs) (OR = 3.10; 95% CI: 1.09–8.83) were independent predictors of HTPR (p < 0.05) after adjusting for other clinical variables.
Conclusions:
In a sample of 100 Puerto Rican Hispanic patients on clopidogrel, 35% had HTPR. Furthermore, DM, PPIs and CCBs predicted HTPR. Clinical outcome data are needed to identify appropriate PRU thresholds for risk prediction in the Puerto Rican population.
Introduction
Platelet adenosine diphosphate (ADP) receptor antagonists are the standard of care for prevention of recurrent atherothrombotic events. Despite the advent of newer agents (i.e. prasugrel, ticagrelor), clopidogrel remains the most prescribed ADP receptor antagonist used by up to 40 million patients worldwide. 1 However, significant variability in clinical response and platelet inhibition has been observed among individuals, leading to failure in reducing adverse cardiovascular outcomes in some patients. 2 Several clinical and genetic factors have been suggested as possible determinants for clopidogrel response variability.3–6 Yet, current evidence is inconsistent about whether clinical factors are independent predictors of high on-treatment platelet reactivity (HTPR). 7
Data on antiplatelet drug response in Hispanics, who are often under-represented in clinical studies are very limited, 8 underscoring the need for studies designed specifically for this high-risk patient population. Moreover, prior studies have demonstrated that Hispanics have a proinflammatory risk status that may contribute to their increased propensity to develop atherosclerotic disease,9,10 as well as a higher prevalence of cardiovascular risk factors, recurrence rate of thrombotic events and worse cardiovascular outcomes when compared to non-Hispanic Whites.11–13 In addition, clopidogrel is preferred among ADP receptor blockers in Puerto Rico, largely because of its availability as a generic drug and lower cost.
Since more emphasis is necessary on the relevance in a resource-poor setting of determining clopidogrel responsiveness and given that clinical predictors of impaired response to clopidogrel are not currently known in Caribbean Hispanics, we sought to determine potential predictors of high platelet reactivity in a small sample of Puerto Rican patients on clopidogrel therapy.
Methods
Study design and ethics
This was a multicenter cross-sectional study of Puerto Rican patients receiving antiplatelet therapy recruited from January to February 2017. The study was approved by the Institutional Review Board (Protocol No. A4070416) and it was conducted in accordance with the Declaration of Helsinki in compliance with Good Clinical Practice. Verbal and written informed consent was obtained from all participants included in the study.
Patient population and data collection
A total of 100 patients, males and females, of Hispanic Puerto Rican descent on clopidogrel therapy for any diagnosis, were consecutively recruited from all geographic regions of the island. Patient information was gathered from the medical record by a single physician. The study included Puerto Rican Hispanics >21 years old who were receiving 75 mg/day maintenance dose of clopidogrel for at least 7 consecutive days. Patients taking any oral anticoagulant or who were recently treated with glycoprotein IIb/IIIa inhibitors were excluded. Other exclusion criteria were Hematocrit (Hct) ⩽ 25%, platelet count < 100,000/mm3, Blood Urea Nitrogen (BUN)/creatinine > 30/1.5 mg/dl or active hepatic disease. The study cohort was divided into two groups based on P2Y12 reaction units (PRUs) cutoff values previously reported in the GRAVITAS study: 14 Group I (65 patients) without HTPR (PRUs < 230) and Group II (35 patients) with HTPR (PRUs ⩾ 230).
Platelet function testing
An initial 2 ml blood sample was collected from each participant and saved for other laboratory tests as part of the preadmission process. A second tube containing 3.2% sodium citrate was then collected with 2 ml blood for platelet function testing. The blood was collected from a peripheral vein and platelet reactivity was assessed within 4 h of blood sampling. Platelet function was measured ex vivo using the United Stated Food and Drug Administration (US FDA)-approved point-of-care VerifyNow P2Y12 analyzer following manufacturer instructions (Accumetrics, Inc. San Diego, CA, USA).
Statistical analysis
Continuous variables were compared using the two-tailed Student’s t-test, and categorical data were assessed using either Chi-square or Fisher’s exact tests as appropriate. Spearman or Pearson correlation tests were used to determine the association between all measurements. A multiple logistic regression was performed to determine predictors of HTPR and a multiple linear regression was used to describe the contribution of clinical characteristics towards PRU values. Receiver operating characteristic (ROC) analysis was used for the evaluation of predictive models. Statistical analyses were performed using SAS software version 9.4 (SAS Institute, Cary, NC, US.), and p-values <0.05 were considered statistically significant.
Results
Study population
The study cohort (n = 100) consisted of patients with coronary artery disease (CAD; 57%), peripheral artery disease (PAD; 32%), carotid artery stenosis (7%), cerebral artery aneurysm (2%), and stroke (2%) on clopidogrel therapy for secondary prevention of thromboembolic events. All patients were on 75 mg/day maintenance dose of clopidogrel for more than 7 days. Among all enrolled patients, the mean platelet reactivity was 200 ± 61 PRUs (range: 8–325) and 35 had HTPR (PRUs ⩾ 230). Figure 1 illustrate the wide distribution of platelet reactivity in the studied population. Moreover, patient baseline characteristics are depicted in Table 1. The non-HTPR and HTPR groups significantly differed in their history of diabetes mellitus (DM), use of proton-pump inhibitors (PPIs), and calcium channel blockers (CCBs) (p < 0.05). No patient reported being on morphine or amiodarone.

Distribution of platelet reactivity as measured by P2Y12 reaction units (PRUs).
Baseline clinical characteristics of the study patients according to on-treatment platelet reactivity.

Values are mean ± SD or n (%).
BMI, Body mass index; HTPR, high on-treatment platelet reactivity.
Correlation between clinical characteristics and HTPR
Significant univariate correlations were observed between HTPR and DM, as well as use of PPIs and CCBs (p < 0.05). No other clinical variables were associated with HTPR. A total of five clinical characteristics (age, DM, active smoking, PPIs, CCBs) previously reported to affect the pharmacokinetics and pharmacodynamics of clopidogrel among non-Hispanics were included in a multivariable logistic regression analysis. Only history of DM, use of PPIs and CCBs were independently correlated with HTPR [odds ratio (OR) = 3.27, 95% confidence interval (CI): 1.20–8.96; OR = 3.60, 95% CI: 1.09–11.82; OR = 3.10, 95% CI: 1.09–8.83; respectively] after adjusting for all other clinical variables (Table 2). Additionally, 28% of the total variation in PRUs was explained by these five clinical factors (R2 = 0.28, p < 0.01).
Stepwise logistic regression analysis to determine the best predictor of high on-treatment platelet reactivity.
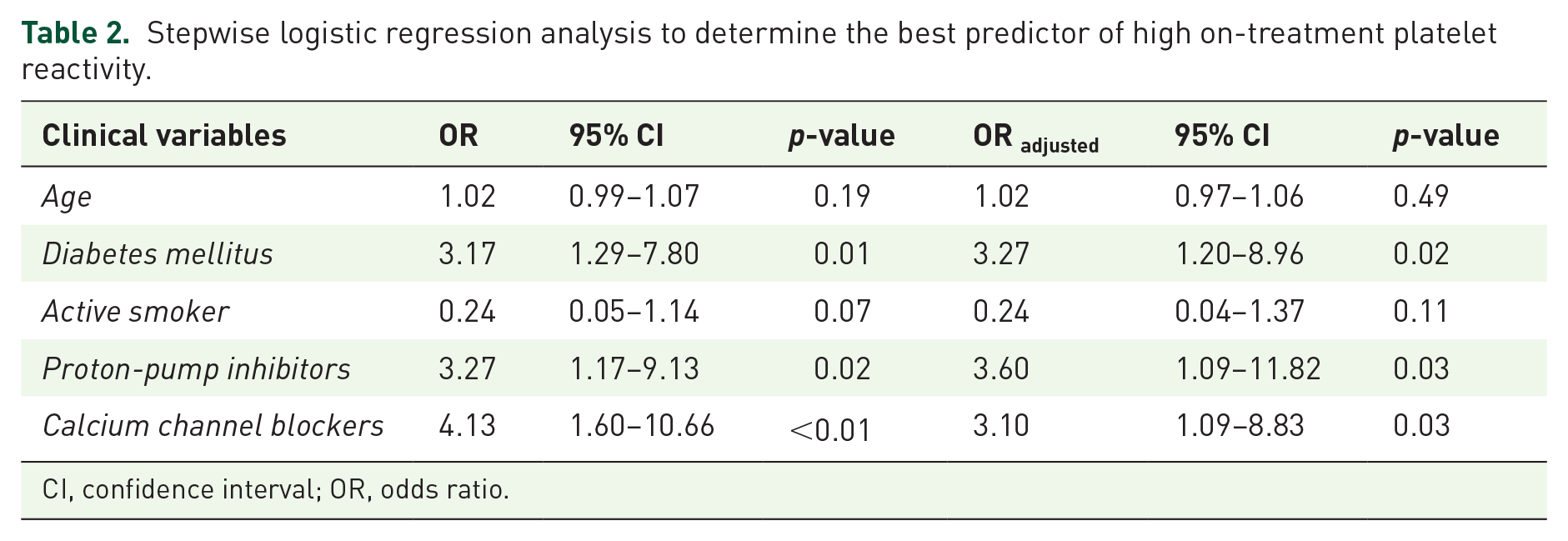
CI, confidence interval; OR, odds ratio.
Development of an HTPR predictive model
Several predictive models to estimate the log odds of HTPR were obtained using both simple and multivariate logistic regression analysis. The best fit model was selected based on the area under the curve (AUC) obtained by a receiver operating characteristic (ROC) analysis and it is represented as follows:

As noticed, the proposed model included all the variables independently associated with HTPR (DM, PPIs and CCBs), as they all together showed the higher AUC (0.7319, 95% CI: 0.6359–0.8278) when compared with the nested simple models (Figure 2).

Receiver operating characteristic curves for HTPR predictive model diagnostics.
Discussion
The paucity of studies exploring the association between clinical factors and HTPR in non-White populations prompted our study on the clinical variables of on-treatment platelet reactivity, which identified a novel association between selected clinical variables and HTPR in a heterogeneous cohort of Puerto Rican Hispanics on clopidogrel therapy.
Similar to other studied populations, history of DM, the use of PPIs and CCBs were independent predictors of HTPR.6,15,16 However, other clinical characteristics such as current smoking status and use of statins were not significantly associated with HTPR in our study cohort. Clinical variables accounted for ~28% of the observed variation in platelet responsiveness. This predicted value is higher than the addition of both clinical and pharmacogenetic factors, previously reported by Larsen and collaborators. 17 The effect of this interaction may be more prominent in Puerto Ricans as they are disproportionately affected by DM and other cardiovascular risk factors when compared with other ethnic groups. 18
High platelet reactivity is an objective measurement of poor clopidogrel responsiveness that has been associated in several studies with an increased risk for thrombotic events.19–21 However, due to a lack of consensus on a standard PRU threshold value to define HTPR, comparisons of reported HTPR prevalence rates are difficult to make and are at high risk for bias. Recent systematic reviews have estimated the prevalence of HTPR to be between 16–50% among patients treated with clopidogrel.21,22 However, proposed HTPR cutoff values are imprecise, and are likely highly dependent on the unique clinical and pharmacogenetic characteristics of each specific studied population. 23 Using the VerifyNow P2Y12 assay, a PRU cutoff value between 230–240 has been reported as prognostic for subsequent major adverse cardiovascular events (MACEs).14,24
We also developed a fitting model to predict HTPR in Puerto Rican Hispanics on 75 mg/day maintenance dose of clopidogrel for at least 7 consecutive days. This model may be useful to target those patients with a high likelihood of having poor response to clopidogrel and consequently, facilitate an early therapy optimization to prevent further adverse cardiovascular events. However, this model, although novel for this population, may benefit from additional clinical, genetic or epigenetic predictors.
One of the limitations of this study is its relatively small sample size, which may decrease its power. However, our intent was to make a preliminary exploration about possible trends in the association between clinical variables and platelet reactivity using VerifyNow point-of-care testing in Puerto Rico. To our knowledge, this is the first time that such a relationship has been studied in the Caribbean. In addition, the cohort does not currently include patients with acute coronary syndromes, so our results may not be generalizable to this specific indication. However, many of our patients were scheduled to undergo percutaneous coronary intervention (PCI) or other vascular stenting procedures shortly after being enrolled in our study. Although most reported studies are focused on the influence of HTPR on MACEs in PCI patients after a loading dose of clopidogrel, the impact of reaching an adequate platelet reactivity value or switching antiplatelet therapy based on clopidogrel responsiveness several days before this procedure remains unclear. Also, despite all patients self-reporting their adherence to clopidogrel, it is possible that some of the enrolled patients may not have been completely adherent. Finally, this study did not include CYP2C19 or other candidate genes reported to influence clopidogrel responsiveness; however, pharmacogenetic analyses are currently underway, which will form the basis of a subsequent manuscript on this important and under-represented population.
Conclusion
We identified specific clinical characteristics (DM, use of PPIs and CCBs) to be independently associated with HTPR (PRUs ⩾ 230) in a Hispanic Puerto Rican patient population treated with clopidogrel antiplatelet therapy. Further studies are warranted to determine if CYP2C19 or other pharmacogenetic determinants of clopidogrel responsiveness are relevant, as well as the role of platelet reactivity in guiding antiplatelet therapy and predicting future adverse cardiovascular events in the Puerto Rican population. Additionally, clinical outcomes data are needed to identify appropriate PRU thresholds for risk prediction in this population.
Footnotes
Acknowledgements
This publication was partially supported by the National Institute on Minority Health and Health Disparities of the National Institutes of Health (NIH) Award Numbers CCTRECD-R25MD007607, HiREC-S21MD001830 and the Research Minority Institutions (RCMI) award 8G12 MD007600. Its contents are solely the responsibility of the authors and do not necessarily represent the official views of the NIH. SAS was supported in part by the National Institute of General Medical Sciences of the NIH, through grant K23GM104401. JD is supported in part by the SC1 grant HL123911 from the National Heart, Lung and Blood Institute (NHLBI) and the MBRS SCORE Program of the National Institute of General Medical Sciences (NIGMS). Also, we would like to acknowledge Dr. Estela Estapé, the staff members of the Preadmission/Admission Department and Public Relationships Office at the Cardiovascular Center of Puerto Rico and the Caribbean, as well as the Endovascular Department of the University of Puerto Rico School of Medicine for their support during the development of this study.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The authors declare that there is no conflict of interest.