
Abstract
Objectives:
The aim of the study was to explore the association between hypertensive retinopathy, grades of retinopathy and cardiac remodelling.
Methods:
This was a cross-sectional observational study. A total of 500 consecutive hypertensive adults from the in-patient population were studied for the presence of hypertensive retinopathy by dilated fundoscopy. The presence of cardiac remodelling due to hypertension was studied both by electrocardiography (ECG) and echocardiography. Hypertensive target organ damage in other organs was also screened. In addition, the association of grades of hypertensive retinopathy with target organ damage was also analyzed.
Results:
Systolic blood pressure (BP) at presentation and duration of hypertension showed no relationship with markers of hypertensive heart disease. However, diastolic BP was significantly higher in patients with retinopathy. Hypertensive retinopathy was diagnosed in 324 subjects of whom 90 had grades 3 and 4 retinopathy. Patients with grades 3 and 4 retinopathy had significant associations with ECG evidence of left ventricular (LV) strain pattern and left atrial enlargement, and a weaker association with left ventricular hypertrophy (LVH) using QRS voltage criteria (Sokolov–Lyon). On echocardiography, grades 3 and 4 retinopathy were significantly associated with LVH, left atrial enlargement and reduced left ventricular ejection fraction (LVEF), as well as with higher creatinine values. A large number of these patients presented with heart failure. Cardiac remodelling was not seen in patients without retinopathy and was uncommon in patients with grades 1 and 2 retinopathy.
Conclusion:
Grades 3 and 4 retinopathy demonstrated a significant association with LV strain pattern and left atrial enlargement on ECG, LVH and reduced LVEF on echocardiography as well as with heart failure. There was no relationship with systolic BP and duration of hypertension, while diastolic BP showed a significant positive correlation. Signs of hypertensive heart disease were practically absent in patients without hypertensive retinopathy and uncommon in those with grade 1–2 alterations.
Introduction
Hypertension has a varied clinical presentation, very often being undetected due to a lack of symptoms. At the time of diagnosis, target organ damage usually exists in most patients [Kannel et al. 1987]. The target organ damage reflecting cardiovascular risk such as left ventricular hypertrophy (LVH) and diastolic dysfunction can result in congestive heart failure and ischaemic heart disease [Neves et al. 2012]. Hypertensive retinopathy has been documented to be an independent predictor of cardiovascular and cerebrovascular disease, irrespective of other hypertensive target organ damage [van den Born et al. 2005]. It is associated with cardiac remodelling, namely concentric LVH as demonstrated by electrocardiography (ECG) and echocardiography. Further, hypertensive retinopathy has been classified into four grades depending on the degree of vascular damage. When prospectively studied, patients with grades 1 and 2 were found to develop hypertension. Grades 3 and 4 were associated with cardiovascular target organ damage, reflected by the presence of left ventricular (LV) remodelling in terms of LVH [Cuspidi et al. 2004].
We wanted to study the association of the grades of hypertensive retinopathy with the degree of cardiac remodelling. We also wanted to test our hypothesis that the more advanced grades of retinopathy are associated with more extensive cardiac remodelling. The marker for cardiac remodelling was LVH and left atrial enlargement as assessed by ECG and two-dimensional (2D) echocardiography. We also assessed the association of grades of retinopathy with other hypertensive target organ damage.
Methods
We studied 500 consecutive patients with hypertension who were in-patients at the cardiology department of St. John’s Medical College Hospital, Bangalore, India. They were admitted for a variety of indications, summarized in Table 1. The study was approved by the Institutional Review Board. All patients were diagnosed to have hypertension according to the Joint National Commission 7 guidelines [Chobanian et al. 2003]. All patients underwent a dilated fundoscopy in the ophthalmology department, and were examined by two ophthalmologists who were blinded to the findings of hypertensive target organ damage. Hypertensive retinopathy was graded according to the Keith–Wagener–Barker classification [Downie et al. 2013]. All patients were screened for hypertensive LV remodelling by ECG and 2D echocardiography criteria. 2D echocardiography was carried out in all patients according to American Society of Echocardiography (ASE) recommendations [Gottdiener et al. 2004], and the LV dimensions in systole and diastole, LV end diastolic volume and end systolic volume, and left atrial dimension were noted. The left ventricular ejection fraction (LVEF) was calculated according to Simpson’s rule. The LV inflow Doppler was interrogated and evaluated for the presence of LV diastolic dysfunction, which was graded according to the ASE guidelines [Nagueh et al. 2009]. Other target organ damage was also noted. Urine was screened for the presence of casts and albumin. The blood sugar, serum creatinine, lipid profile and haemoglobin values were also noted.
Admission diagnosis in hypertensive patients. Demographic details of the patient study population. Numbers of patients with diabetes mellitus, dyslipidemia, history of smoking and urinary albuminuria are highlighted.

Statistical analysis
All continuous normally distributed data were reported as mean ± standard deviation and as median (quartile 1, quartile 3), if not normally distributed. Categorical data were reported as n (%). The normal distribution of continuous data was examined using normal Q–Q plots. Continuous data were compared between patients with and without hypertensive retinopathy using independent sample Student’s t-test or nonparametric Mann–Whitney U test. The association of hypertensive retinopathy with categorical characteristics was examined using the chi-square test. All characteristics statistically significant in these analyses were considered in a multiple variable logistic regression of hypertensive retinopathy. The adjusted odds ratio (OR) and corresponding 95% confidence interval (CI) were reported. All analyses were performed in SPSS V 18.0 and statistical significance was considered at p < 0.05.
Results
There were 500 hypertensive adults, 322 men and 178 women. Baseline characteristics such as patients’ age, duration of hypertension, duration of diabetes mellitus and systolic blood pressure (BP) were comparable between those with and without hypertensive retinopathy (Table 2). Patients with retinopathy had a small but significantly higher diastolic BP (94.15 ± 15.3 mmHg versus 90.6 ± 14.3 mmHg, p = 0.013) and heart rate (87.6 ± 20.7 bpm versus 83.8 ± 16.4 bpm, p = 0.035). There was no significant difference between patients with hypertensive retinopathy and those without with respect to other target organ damage. A multiple variable logistic regression analysis was performed where hypertensive retinopathy was found to be significantly associated with higher diastolic BP when compared with patients without hypertensive retinopathy. Diastolic BP alone was statistically significant in the multivariable logistic regression such that there were higher odds of hypertensive retinopathy with increasing diastolic BP (OR = 1.025, 95% CI 1.01–1.04, p < 0.001) (Figure 1).
Comparison of clinical characteristics of hypertensive patients with and without hypertensive retinopathy.


The odds ratio of hypertensive retinopathy and its associations.
As it has been documented that the early stages of hypertensive retinopathy reflected by grades 1 and 2 of the Keith–Wagener–Barker classification have no association with evidence of cardiovascular and other target organ damage, we compared the advanced grades of retinopathy for their association with cardiovascular and other target organ damage [Cuspidi et al. 2009].
Fundoscopic examination found hypertensive retinopathy in 324 patients (grades 1–2 in 234 and grades 3–4 in 90); 176 patients did not demonstrate hypertensive retinopathy. It has been documented that detection of the early stages of hypertensive retinopathy, mainly grades 1 and 2 are associated with inter-observer and intra-observer variability, whereas detection of grades 3 and 4 have negligible inter-observer and intra-observer variability [van den Born et al. 2005]. In our study, the inter-observer and intra-observer variability for the detection of grades 3 and 4 hypertensive retinopathy was not significant.
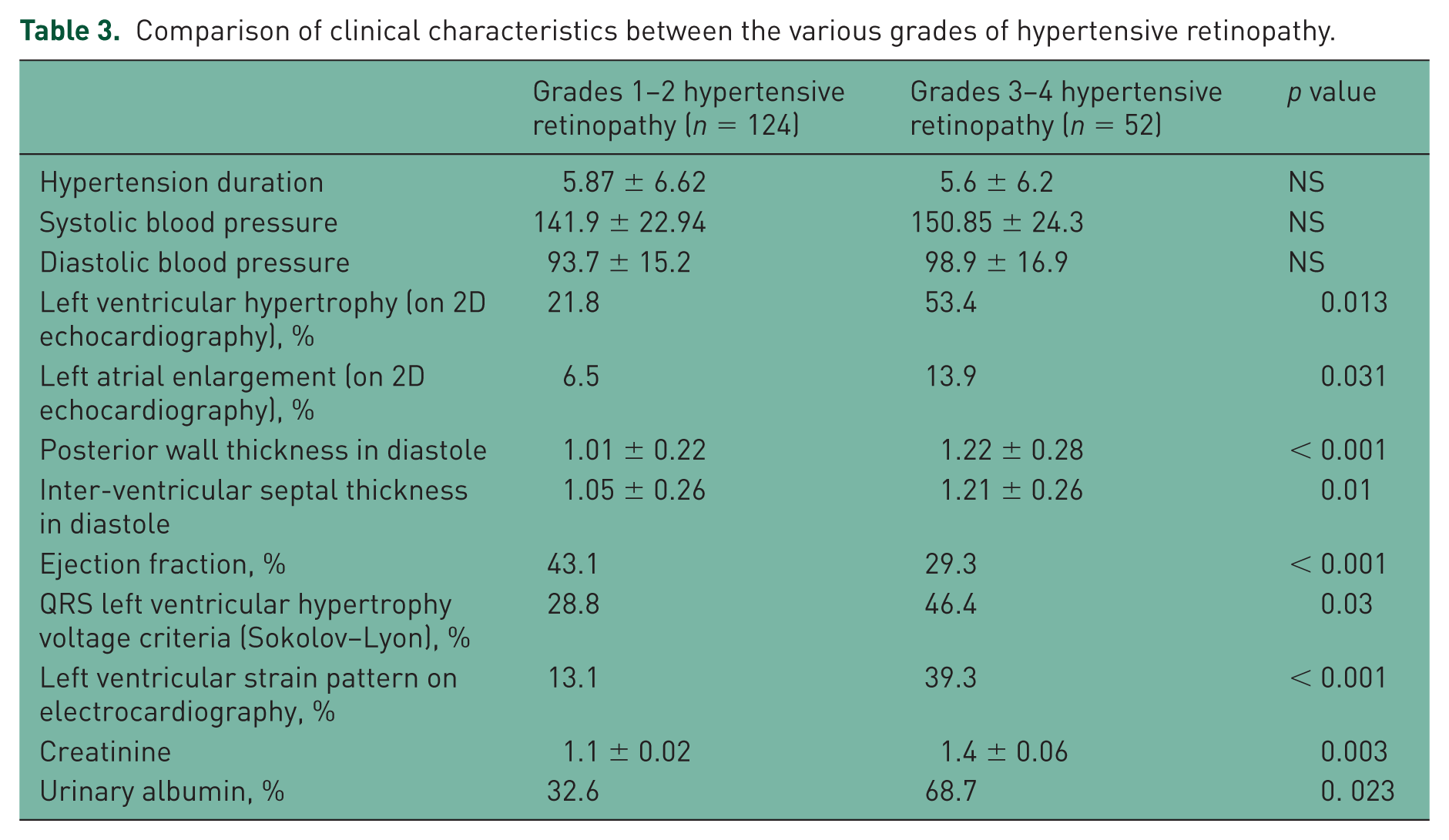
In patients with greater degrees of microvascular retinal changes, grades 3 and 4 were compared with grades 1 and 2 for associations with other hypertensive target organ damage, patients with grades 3 and 4 hypertensive retinopathy had significantly greater heart rates (95.6 bpm versus 86.9 bpm, p = 0.037), greater degrees of left atrial enlargement (13.9% versus 6.5%, p = 0.031), LVH on ECG (46.4% versus 28.8%, p = 0.013), strain pattern on ECG (39.3% versus 13.1%, p < 0.0001), the LV posterior wall dimensions were also greater (1.2 cm versus 1.0 cm, p < 0.0001), as was the interventricular thickness (1.17 cm versus 1.03 cm, p = 0.001) on 2D echocardiography. Serum creatinine was also greater with grades 3 and 4 retinopathy (123.7 µmol/L versus 97.2 µmol/L, p = 0.003), as was the 24 h urinary albumin excretion. There were significantly more admissions for congestive heart failure with lower LVEFs in patients with grades 3 and 4 hypertensive retinopathy when compared with patients with grades 1 and 2 hypertensive retinopathy (Table 3).
Comparison of clinical characteristics between the various grades of hypertensive retinopathy.
Discussion
Hypertension is often associated with asymptomatic target organ damage. Ideally, screening should include ECG abnormalities like LVH, microalbuminuria, carotid intima-media thickness and arterial pulse wave velocity. Hypertensive retinopathy, which is a target organ damage, is often associated with other target organ damage and helps in prognostication of hypertension. By comparing patients with all grades of hypertensive retinopathy as a group with those with normal fundus, there was no significant difference in end-organ damage, namely the presence of left atrial enlargement on ECG, LV chamber dilatation, LVEF, left atrial enlargement, inter-ventricular septal thickness, posterior wall thickness and LV diastolic dysfunction on 2D echocardiography. There was also no significant association with creatinine levels and urinary sediments.
In the whole group of patients with hypertensive retinopathy there was a significantly positive association with the presence of LVH and a weakly significant association with increased diastolic BP. An association of hypertensive retinopathy with target organ damage has been documented in prospective follow-up studies, helping in prognostication of these patients. Cross-sectional studies have not documented a significant association [Grassi et al. 2007; Wong et al. 2002]. A significantly positive association of LV remodelling with advanced grades of retinopathy, namely grades 3 and 4 has been documented [Cuspidi et al. 2004].
Hypertensive retinopathy has been graded into four stages of increasing severity by the Keith–Wagener–Barker classification. The relevance of this classification has been the centre of debate for several years [Dimmit et al. 1989]. This is especially true due to the wide inter-observer variability of 20–40% and intra-observer variability of 10–30% applicable to stages 1 and 2 [Grassi et al. 2007]. Guidelines do not recommend fundoscopy as a screening tool for hypertension and have restricted it for prognostication of hypertension, especially in the presence of haemorrhages and exudates, indicative of grades 3 and 4 [Wong et al. 2002, 2004].
Lesser degrees of microvascular retinal changes (arteriovenous nicking, generalized or focal arteriolar narrowing, and arteriovenous ratio) were considered weaker indicators of vascular and target organ damage.
Here, we screened an in-patient adult hypertensive population for the presence of hypertensive target organ damage in terms of LV remodelling and the presence of other target organ damage. Most patients were admitted with clinical manifestations of cardiovascular target organ damage, mainly congestive heart failure and unstable angina. There was a significantly greater number of patients with grades 3 and 4 retinopathy admitted with congestive heart failure. These patients with advanced grades of retinopathy also had a lower LVEF, which was reflected clinically as heart failure admissions.
Taking into account data regarding greater associations of target organ damage with advanced retinopathy, we re-analysed patients with hypertensive retinopathy and subdivided them into two groups according to the presence and severity of fundoscopic alteration: group 1 with grades 1–2 and group 2 with grades 3–4 degree alterations. The results are shown in Table 3.
ECG strain pattern as a prognostic predictor in arterial hypertension
The presence of a typical strain pattern on ECG in hypertensive patients identifies those at higher risk of cardiovascular mortality and morbidity [Salles et al. 2006]. Patients with strain pattern have been shown to have a five-fold increased risk of congestive heart failure mortality [Okin et al. 2006]. As a rule, LV strain is associated with a greater increase in LV mass and LV hypertrophy (more often concentric) and signs of other end-organ damage (e.g. renal damage evidenced by hyper creatininaemia and albuminuria) [Cordeiro et al. 2014].This prognostic value of ECG strain pattern has been shown to be independent of the presence of ECG LVH as indicated by QRS voltage criteria by Sokolov–Lyon [Salles et al. 2006; Ehara et al. 2014]. ECG strain pattern classically refers to changes in transmembrane action potential duration of contiguous layers of the thickened LV wall. The Losartan Intervention for Endpoint Reduction in Hypertension (LIFE) trial showed regression of ECG alterations after aggressive antihypertensive treatment, which was followed by a significant thinning of the LV wall [Okin et al. 2006]. ST depression and T-wave inversion might also reflect true subendocardial ischaemia, independent of coronary disease, if the compensatory increase in coronary bed is inadequate for the increase of LV mass and thickness [Salles et al. 2006]. Our results suggest a third hypothesis, having demonstrated a statistical correlation between fundoscopic microvascular alterations (hypertensive retinopathy grades 3–4) and ECG alterations of LV strain pattern and LVH, which were absent in patients without fundoscopic alterations and present in about 10% of patients with grades 1–2 retinopathy. Almost 40% of those with clear signs of microvascular involvement (exudates and haemorrhages) had associated LV strain pattern on ECG. Microvascular coronary involvement in hypertensive patients with advanced retinopathy is likely from these findings.
The association of hypertensive retinopathy and coronary heart disease has not been consistent, although an increased risk of coronary events was observed in hypertensive women [Breslin et al. 1966]. This gender-related observation may reflect the higher risk of coronary microvascular disease among women than in men. Myocardial perfusion reserve measured after maximal vasodilation with adenosine reflects microvascular changes in the coronary circulation and may contribute to the risk of coronary heart disease in hypertensive patients independent of obstructive stenosis in the epicardial arteries. In a cross-sectional study, decreased myocardial perfusion reserve was associated with narrower retinal arterioles [Wang et al. 2008].
In essential hypertension, vascular remodelling occurs early in small arteries with a lumen diameter of 100–350 µm, of which the sizes are similar to the diameter of retinal arterioles. In hypertensive patients, endothelial dysfunction has been documented in systemic, coronary, renal and retinal circulations [Delles et al. 2004], leading to increased wall:lumen ratio in these arteries. Prospective studies have defined the arteriolar narrowing in the retinal circulation corresponding with the increase in wall:lumen ratio as indicative of microvascular changes in the coronary circulation, predictive of cardiovascular mortality [Wong et al. 2002; Wang et al. 2008; Kothwade and Noel Bairey Merz, 2011]. The association of ECG strain pattern with cardiovascular morbidity and mortality has been established in patients with chronic kidney disease [Cordeiro et al. 2014].
In our cross-sectional study, there was a significant positive association between the presence of ECG strain pattern and advanced grades of hypertensive retinopathy, which was greater than its association with LVH on ECG. This also correlated with LVH on 2D echocardiography and serum creatinine. Grades 3 and 4 hypertensive retinopathy, which are markers of greater retinal damage due to hypertension, have been reported to have an association with LVH on 2D echocardiography [Cuspidi et al. 2004]. Clinically, patients with grades 3 and 4 hypertensive retinopathy were associated with lower LVEFs. We do not have coronary angiographic data on all these patients and hence cannot document the presence of high-grade epicardial coronary artery stenosis in them.
We report the association of ECG strain pattern and presence of LVH on 2D echocardiography with advanced microvascular retinal changes, which generates a hypothesis of microvascular involvement in the myocardial coronaries.
Limitations
This being a cross-sectional study, it had its inherent limitations in defining associations of hypertensive retinopathy with other target organ damage. In our study, the presence of LVH on ECG correlated positively with hypertensive retinopathy, while higher grades of retinopathy correlated well with LVH on 2D echocardiography. It has been well established that LVH by ECG and LVH by echocardiographic criteria are independently associated with cardiovascular mortality [Sundström et al. 2001], validating our findings. We have not carried out carotid Doppler to evaluate carotid intima-media thickness, which would have further qualified our results along with the pulse wave velocity. We do not have LV strain data for these patients. We have quantified LV function by LVEF. Reduced global LV strain has been well established as a surrogate sensitive marker of LV dysfunction. The association of reduced LV global strain with hypertensive retinopathy is well established. For documentation of the association of coronary artery disease with hypertensive retinopathy, we do not have coronary angiographic data on our patients to define the presence of high-grade epicardial coronary stenosis. We have not carried out myocardial perfusion studies to document microvascular disease due to logistic constraints. In addition, we do not have prospective data on these patients that would have helped define the associations of retinopathy and ECG changes with cardiovascular morbidity and mortality.
Conclusion
In a cross-sectional study, grades 3 and 4 retinopathy demonstrated a significant association with LV strain pattern and left atrial enlargement on ECG, LVH on echocardiography, higher incidence of congestive heart failure and reduced LVEF. There was no relationship with duration of hypertension and systolic BP, while diastolic BP was significantly higher. Signs of hypertensive heart disease and other target organ damage were practically absent in patients without hypertensive retinopathy and uncommon in those with grade 1–2 alterations.
Footnotes
Acknowledgements
We gratefully acknowledge the expert guidance of Professor Fabio Fantini, MD, Retired Professor of Cardiology, University of Florence, Italy, in preparing the manuscript.
Funding
This research received no grant from any funding agency in the public, commercial or not-for-profit sectors.
Conflict of interest statement
The authors declare that there is no conflict of interest.