
Abstract
Objectives:
New-generation coronary stents including zotarolimus- and everolimus-eluting stents (ZES and EES) have been shown to decrease the risk of restenosis. The purpose of this study was to compare the safety and efficacy of ZES and EES over a 12-month clinical follow up, in routine clinical practice.
Methods:
This is an observational study in which 1029 consecutive patients treated with ZES (n = 669) or EES (n = 360) were enrolled. The study endpoint was major adverse cardiac events (MACE), defined as cardiac death, nonfatal myocardial infarction (MI), and target lesion or vessel revascularization at 12 months.
Results:
Follow up was completed among 94.9% of the patients. The overall MACE occurred in 4 (0.6%) and 7 (2.0%) patients in the ZES and EES group, respectively. The occurrence of other cardiac events including nonfatal MI and target vessel or lesion revascularization was 1 (0.2%) versus 1 (0.3%) and 7 (1.1%) versus 5 (1.4%), respectively, in the ZES and EES groups of patients. Despite a slightly lower rate of MACE and cardiac death in the ZES group, the difference between these two groups was not significant (n = 0.064 for overall MACE, p = 0.129 for cardiac mortality, n = 0.999 for nonfatal MI, n = 0.468 for target vessel and n = 0.999 for target lesion revascularization).
Conclusions:
According to our results, it could be concluded that the difference in the rate of MACE between the ZES and EES groups was not statistically significant at 12-month follow up.
Introduction
Percutaneous coronary intervention (PCI) has become the most widely used method to treat patients with coronary artery disease. The high rate of restenosis with this procedure can be reduced with stent implantation [Serruys et al. 1994; Fischman et al. 1994]. Initially the bare-metal stent (BMS) reduced the rate of restenosis. However, the BMS was associated with a high rate of in-stent restenosis that usually developed within 3–12 months of initial stent implantation [Ferguson et al. 2010]. Previously published randomized controlled trials have shown lower rates of clinical and angiographic restenosis and major adverse cardiac events with the drug-eluting stent (DES) [Indolfi et al. 2005; Tanabe et al. 2003; Colombo et al. 2003; Ong et al. 2005; Morice et al. 2002; Hermiller et al. 2005; Bavry et al. 2005]. First-generation DESs included the sirolimus-eluting cypher stent in 2003 and the paclitaxel-eluting taxus express stent in 2004, both approved by the Food and Drug Administration for use [Carlsson et al. 2009]. Early randomized clinical trials have demonstrated the safety and efficacy of first-generation DESs [Stone et al. 2007; Moses et al. 2003]. Second-generation DESs have subsequently been developed with the aim of further improving the safety and efficacy profile of the DES [Smits 2010]. Second-generation DESs such as everolimous- and zotarolimus-eluting stents (EESs and ZESs, respectively) are presumed to display a better safety profile compared with first-generation DESs; however, long-term, largescale clinical data supporting this hypothesis are lacking [Camici et al. 2010]. The Resolute ALL COMERS trial demonstrated no significant difference in the rate of the primary endpoint of target vessel failure (cardiac death, any myocardial infarction (MI), or clinically indicated target lesion revascularization within 12 months) between the ZES and EES. The ZES was also noninferior to the EES with respect to in-stent restenosis or in-stent late-lumen loss. The rate of stent thrombosis was not significantly different between the two groups (2.3% versus 1.5%, respectively) [Serruys et al. 2010]. Data presented by Stone and colleagues showed no clinically significant differences between DESs of varying designs [Lee, 2004].
There are many randomized clinical trials comparing different types of the DES. Some randomized clinical trials are inherently limited by their rigid inclusion criteria, predisposing them to some kind of selection bias [Grapow et al. 2006]. Clinical outcome data from everyday practice was very limited for both the EES and ZES until recently, and the differences in efficacy and safety between these two new-generation stents were not statistically significant. In an attempt to compare the clinical outcomes of the ZES and EES, we reviewed the Angioplasty Registry of the Tehran Heart Center (THC).
Methods
The data were extracted from the Tehran Heart Center Registry of Interventional Cardiology (THCRIC), a single-center nonrandomized computerized data registry in which all adult patients who undergo single or multi-vessel PCI are enrolled without any specific exclusion criteria. Detailed data on demographic and clinical characteristics such as previous medical status and history of risk factors in conjunction with procedural data, including lesions characteristics, type of procedure and stent used, complications, discharge disposition and destination, medication, and clinical follow-up data were documented in our registry. The follow-up data, first and foremost amongst which details of major adverse cardiac events (MACE) were obtained, were collated through organized clinical visits or telephone contact by trained research physicians and nurses at hospital discharge at one, six, and twelve months after PCI. All the data were recorded in formal datasheets and afterwards entered into a computerized data bank [Salarifar et al. 2013]. The institute review board approved the study protocol, overseeing the participation of human subjects in research at Tehran University of Medical Sciences.
Study population
In this study, adult patients with at least one significant stenotic lesion (⩾ 70%) who underwent PCI and deployed at least one DES (ZES or EES) were included. There was no restriction on the total number of treated lesions, treated vessels, lesion length, and number of stents. Patients with the following conditions were excluded from the study: left main artery stenosis (⩾ 50%), primary PCI, left ventricular ejection fraction [(LVEF) < 30%], previous history of coronary artery bypass grafting (CABG) or PCI, chronic renal dysfunction (Cr > 2.5 mg/dl or under dialysis), and deployment of more than one type of the DES in the session. Between January 2006 and May 2009, of all 9906 patients who underwent PCI in our center, 1029 cases met our inclusion criteria. Of these cases, 669 (65.01%) patients were treated with the ZES and 360 (34.99%) received the EES.
Angioplasty procedure
The EES (Xience V, Abbott Vascular, USA; Xience Prime, Abbott Vascular, USA; and Promus, Boston Scientific, USA) was available in diameters of 2.50 mm, 2.75 mm, 3.00 mm, and 3.50 mm and in lengths of 12, 15, 18, 23, and 28 mm for Xience V; and 12, 15, 18, 23, 28, 33, and 38 mm for Xience Prime and Promus. The ZES (Endeavor, Medtronic, USA) was available in diameters of 2.50 mm, 2.75 mm, 3.00 mm, and 3.50 mm and in lengths of 12, 14, 18, 24, 30, and 38 mm. Before PCI, the patients were pretreated with aspirin 325 mg, clopidogrel loading 600 mg (at least 2 hours ‘beforehand’), and weight-adjusted intravenous unfractionated heparin. Additionally, they were administered intracoronary nitroglycerine before PCI and had a final angiogram view taken. Lesion balloon predilation was attempted as needed. The goal of the stenting was full-lesion coverage even with one or more stents. The selection of the size and type of the stent was based on the interventional cardiologists’ decision. Cardiac enzyme (CK-MB) was checked twice, and ECG was obtained after PCI and before discharge. The patients were discharged on clopidogrel 75 mg/d for 12 months and aspirin 325 mg/d for at least 3 months and 80 mg/d for an indefinite period after PCI. For each patient undergoing PCI, the following information was collected: demographics, coronary risk factor, type, location and severity of lesion, type of the stent, and periprocedural complication.
Definitions
Periprocedure MI was defined by at least one of the following criteria: 1 evolutionary ST-segment elevation, development of new Q-wave in 2 or more contiguous ECG leads, or new or presumably new left-bundle branch-block pattern on the ECG; and biochemical evidence of CK-MB mass at least 3 times the upper limit of normal: for our lab, normal limit of CK-MB mass is 6.73 for males and 3.77 for females. After discharge, MI was defined as a rise and fall in cardiac enzyme (CK-MB or troponin) with one of the following: development of pathologic Q wave, ischemic ECG change, and ischemic symptoms. The study endpoint was the occurrence of MACE during the follow up, defined as cardiac death, nonfatal MI, target-lesion revascularization, and target-vessel revascularization (PCI or CABG). Target lesion revascularization was defined as either repeat percutaneous or surgical revascularization for a lesion anywhere within the stent or 5 mm borders proximal or distal to the stent. Target-lesion revascularization was considered ischemia-driven if the target lesion diameter stenosis was at least 50% at angiography with either objective evidence of ischemia on noninvasive study or symptoms, or if the lesion stenosis was at least 70% of the vessel diameter in the absence of ischemia signs. Target-vessel revascularization was defined as intervention for chest pain or positive test (exercise stress test, stress echocardiogram, resting electrocardiographic evidence of ST-segment depression or elevation in at least one lead, or radionuclide study showing reversible defect) for ischemia (PCI or CABG) driven by lesion in the same epicardial vessel, otherwise priority lesion as that initially treated.
Statistical methods
The results are presented as mean values ± SD (standard deviation) for the quantitative variables and are summarized by absolute frequencies and percentages for the categorical variables. The continuous variables were compared using the Student t-test, and the categorical variables were compared using the chi-square or Fisher exact test, as required, across the two groups of patients who received the EES or ZES. The Kolmogorov–Smirnov test was applied to verify data distribution normality. The Kaplan–Meier method was used to determine survival, and the log-rank test was utilized to compare the effects of these two different DESs on survival.
A paucity of events during the follow-up period precluded a multivariable analysis and adjustment for potential confounders, although a trend favoring the ZES use was observed in the univariate analysis.
For the statistical analyses, the statistical software SPSS version 13.0 for Windows (SPSS Inc., Chicago, IL) was employed. All the p values were two-tailed, with statistical significance defined by a p value ⩽ 0.05.
Results
Amongst the 1029 patients who were enrolled in our study, 669 (65.01%) patients were treated with the ZES and 360 (34.99%) received the EES. The baseline demographic and clinical characteristics of the study population are depicted in Table 1. According to our results, it seems that the EES was used more commonly for female patients, patients with a history of diabetes mellitus and NSTEMI. The procedural characteristics are presented in Table 2. Type B2 and C lesions (according to the American College of Cardiology/American Heart Association lesion classification), bifurcations, and total occlusion were more common in the EES group. Total lesion length was similar between the two groups (p value = 0.661), whereas total stent length was significantly higher in the ZES group (p value = 0.007). Also, postdilation pressure was significantly higher in the EES group.
Baseline demographic and clinical characteristics.

Data are presented as mean ± SD or n (%). SD, standard deviation; CAD, coronary artery disease; MI, myocardial infarction; STEMI, ST-segment elevation myocardial infarction; NSTEMI, non-ST-segment elevation myocardial infarction; CVA, cerebrovascular accident; LVEF, left ventricular ejection fraction.
Procedural characteristics.

Data are presented as mean ± SD or n (%). PCI, percutaneous coronary intervention; LAD, left anterior descending artery; LCX, left circumflex artery; RCA, right coronary artery; TIMI, thrombolysis in myocardial infarction.
According to American College of Cardiology/American Heart Association Classification.
Twelve-month clinical outcome
The one-year clinical outcomes were compared between the EES and ZES groups of patients (Table 3 and Figure 1). The twelve-month clinical follow up via clinical visit or telephone contact was complete in 94.9% of the patients. The overall twelve-month MACE rate was higher in the EES group than that in the ZES group (2.0% versus 0.6%, respectively), but the difference between the two groups was not statistically significant (p value = 0.064). Amongst the patients receiving the EES, there was 1 (0.3%) case of in-hospital mortality during hospitalization after PCI; target vessel revascularization was performed in 4 (1.1%) cases, and 1 (0.3%) case underwent target-lesion revascularization. There was no case of CABG. The incidence of nonfatal MI was 0.3% (1 case) in the EES group, and there were 2 (0.6%) cardiac deaths during the follow up.
Twelve-month MACE.
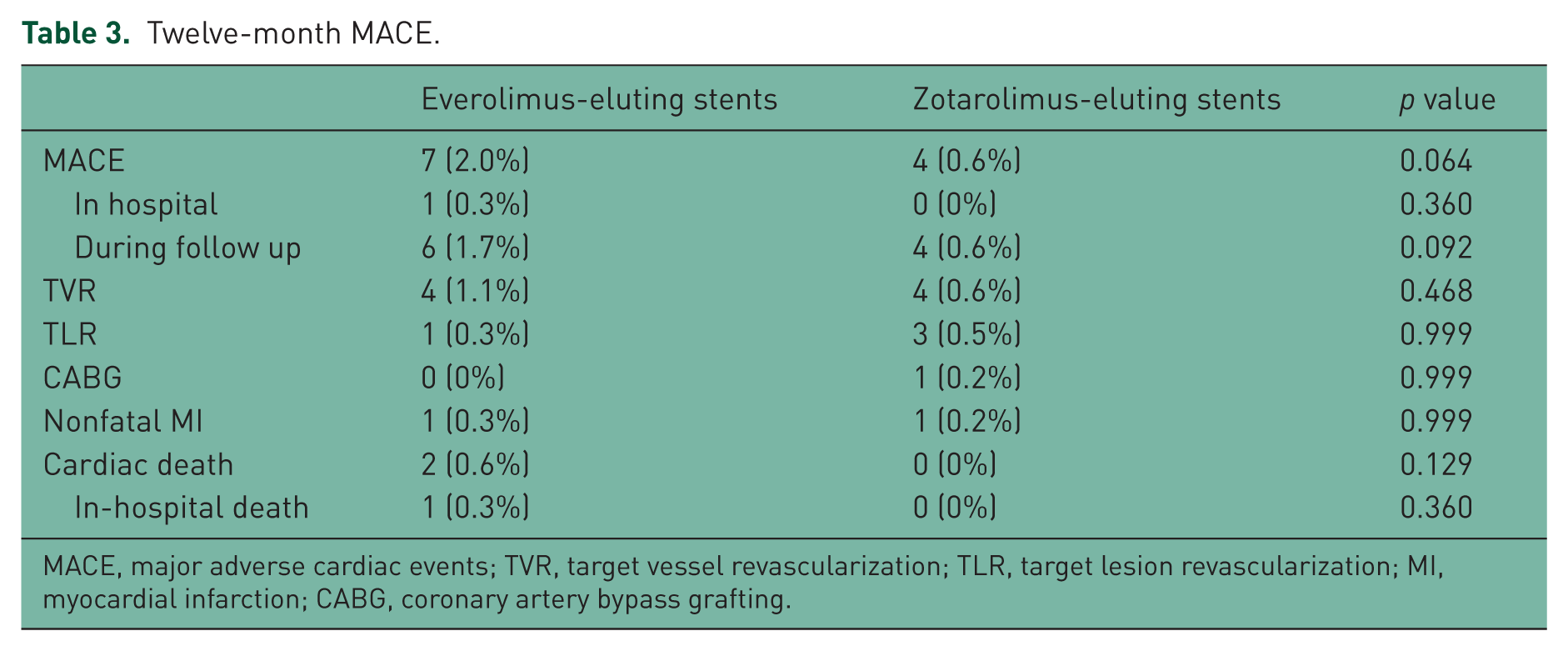
MACE, major adverse cardiac events; TVR, target vessel revascularization; TLR, target lesion revascularization; MI, myocardial infarction; CABG, coronary artery bypass grafting.

Kaplan–Meier plot of cumulative survival of MACE to 12 months for patients receiving drug-eluting stents.
In the ZES group, there was no case of in-hospital mortality and nor was there any case of mortality during the follow-up period. The difference in the mortality rate between the two groups was not statistically significant (p value = 0.129). Nonfatal MI occurred in 1 (0.2%) of the patients in the ZES group. Four (0.6%) cases underwent target vessel revascularization, and there was 1 (0.2%) case of CABG. The incidence of target lesion revascularization was 0.5%, it having been performed for 3 cases. A comparison between the two groups showed no significant difference in terms of the twelve-month rates of target-vessel revascularization, target-lesion revascularization, CABG, and nonfatal MI.
Discussions
In the present study, we sought to compare the clinical endpoints between the patients receiving the ZES and EES during a follow-up period of one year. We enrolled 1029 consecutive unselected PCI patients in the THCRIC Registry who had received the EES (35.0%) or ZES (65.0%) and compared the twelve-month clinical outcomes between these two groups. Follow-up data were available for 978 of the 1029 patients, yielding an account of a 94.9% 1-year follow-up rate. According to our results, despite a slightly lower rate of MACE and cardiac death in the ZES group compared with the EES group (0.6% versus 2.0% for total MACE and 0% versus 0.9% for cardiac death), the differences in terms of efficacy and safety between these two new-generation stents were not statistically significant.
There was a dearth of data in the existing literature on the comparison between the ZES and EES. Indeed, the editorial by Mukherjee and Moliterno stressed the need to accelerate obtaining real-world experience data on the outcomes of second-generation stents [Mukherjee and Moliterno, 2009]. In a clinical trial by Serruys and colleagues, where 2292 patients were randomly enrolled, they demonstrated that the ZES was noninferior to the EES (primary endpoint occurred in 8.2% and 8.3% of patients, respectively) in a population with minimal exclusion criteria (p value < 0.001 for noninferiority). They found that there were no significant differences in the rate of mortality, target-vessel revascularization, target-lesion revascularization, and MI between the two groups [Serruys et al. 2010]. Also, another study by Mahmoodi and collegues investigated the safety and efficacy of the ZES and EES in the treatment of patients with coronary artery disease during a 6-month follow-up period, demonstrating no difference in the incidence of MACE between the ZES and EES at 6 months (the MACE rate was 4.1% in the EES group and 5.0% in the ZES group, p value = 0.61) [Mahmoudi et al. 2010]. Recently, the results of the TWENTE (the real-world endeavor Resolute versus Xience V drug-eluting stent study in TWENTE) trial also revealed that, after two years of follow up, Resolute ZES and Xience V EES showed similar results in terms of safety and efficacy for treating patients with a majority of complex lesions and off-label indications for drug-eluting stents [Tandjung et al. 2013].
The THCRIC is a single-center nonrandomized data registry in which all adult patients who undergo single- or multi-vessel PCI have been enrolled without any specific exclusion criteria since 2004. In our study, in tandem with previous studies that drew upon data from the THCRIC [Alidoosti et al. 2008; Kassaian et al. 2006], the rate of the MACE amongst patients who underwent PCI in our center is comparatively low [Serruys et al. 2010; Onuma et al. 2009; Lotan et al. 2009]. One of the remarkable plausible causes leading to these outcomes in our center might be the lower mean age of our patients compared with that in other studies [Serruys et al. 2010; Onuma et al. 2009; Lotan et al. 2009; Kedhi et al. 2010]. The mean age of our patients was almost 10 years lower than the mean age of the patients included in the Resolute ALL COMERS trial and the TWENTE trial. This is related to the epidemiology of coronary artery disease (CAD) and high prevalence of premature CAD in our country as a developing country. Among the 11 MACEs that occurred in our patients, 4 MACEs occurred in patients with premature CAD.
First and foremost amongst the limitations of the present study is that we were not able to adjust the observed significant differences between the EES and ZES groups in Tables 1 and 2 for their probable confounding effects, avoiding the ‘overfitting’ problems. The results of multivariate models having fewer than 10 outcome events per independent variable are, in general, thought to have questionable accuracy [Concato et al. 1993; Harrell et al. 1985; Harrell, 1983; Saia et al. 2008]. Since the number of cases with MACE was low in our study (totally, 11 cases in the two groups), we could not adjust the probable confounders in this sample size. In addition, routine angiographic follow up was not scheduled for our patients, not only because of ethical and cost considerations but also because of the fact that our center is a tertiary and high-volume center (more than 2000 PCI procedures per year).
Be that as it may, for all the limitations of the present study and the paucity of data comparing the EES and ZES clinical outcomes in the existing literature, it can be concluded in light of our results that there is no statistically significant difference in the rate of MACE between the EES and ZES groups at twelve-month follow up. It is also deserving of note that our study results chime in with those of previous limited studies on the similarity between these two second-generation stents.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The authors declare that there is no conflict of interest.