
Abstract
Objectives:
The Quality and Care Model Committee for a clinically integrated network requested a comparative analysis on the projected cardiovascular benefits of implementing either the 2013 and 2014 cholesterol guideline in a South Carolina patient population. A secondary request was to assess the relative risk of the two guidelines based on the literature.
Methods:
Electronic health data were obtained on 1,580,860 adults aged 21–80 years who had had one or more visits from January 2013 to June 2015; 566,688 had data to calculate 10-year atherosclerotic cardiovascular disease (ASCVD10) risk. Adults with end-stage renal disease (n = 7852), congestive heart failure (n = 19,818), alcohol or drug abuse (n = 68,547), or currently on statins (n = 154,964) were excluded leaving 315,508 for analysis. Estimated reduction in ASCVD10 assumed that: (a) moderate-intensity statins lowered low-density lipoprotein cholesterol (LDL-C) by 35% and high-intensity statins by 50%; (b) ASCVD events declined 22% for each 1 mmol/l fall in LDL-C.
Results:
Among the 315,508 adults in the analysis, 131,289 (41.6%) were eligible for statins according to the 2013 guideline and 137,375 (43.5%) to the 2014 guideline. The 2013 and 2014 guidelines were estimated to prevent 6780 and 5915 ASCVD events over 10 years with: (a) relative risk reductions of 29.0% and 21.8%; (b) absolute risk reductions of 5.2% and 4.3%; (c) number needed-to-treat (NNT) of 19 and 23, respectively. The greater projected cardiovascular protection with the 2013 guideline was largely related to greater use of high-dose statins, which carry a greater risk for adverse events. The literature indicates that the NNT for benefit with high-intensity versus moderate-intensity statins is 31 in high-risk patients with a number needed-to-harm of 47.
Conclusions:
The 2013 guideline is projected to prevent more clinical ASCVD events and with lower NNTs than the 2014 guideline, yet both have substantial benefit. The 2013 guideline is also expected to generate more adverse events, but the risk-benefit profile appears favor .
Introduction
Hypercholesterolemia is a major, modifiable risk factor for atherosclerotic cardiovascular disease (ASCVD). Statins are first-line therapy for the primary and secondary prevention of ASCVD [Taylor et al. 2013; Stone et al. 2014]. Hypercholesterolemia is treated less often than hypertension [Muntner et al. 2013; Egan et al. 2014]. Thus, the number of preventable ASCVD events is potentially large. Moreover, the US population is aging and with increasing proportions of racially and ethnically diverse groups that have greater cardiometabolic risk [Jacobsen et al. 2011; Passel and Cohn, 2008]. These population and demographic changes are projected to increase cardiovascular-related healthcare costs from US$460 billion in 2010 to US$1.1 trillion in the USA by 2030 (constant 2008 dollars) [Heidenreich et al. 2011]. In the USA, the southeast has higher cardiovascular mortality than other regions, which is associated with, but not fully explained by, lower socioeconomic and educational status as well as a proportionately larger African-American population [Shikany et al. 2015].
The National Cholesterol Education Program/Adult Treatment Panel–3 (NCEP/ATP–3) guideline was initially published in 2001 and updated in 2004 [NCEP, 2001; Grundy et al. 2004]. The 2013 cholesterol guideline includes new evidence since 2004, is a stronger predictor of ASCVD and coronary calcium scores [Pursnani et al. 2015], and would treat approximately 12.8 million more adults for hypercholesterolemia than NCEP/ATP–3 [Pencina et al. 2014]. These observations suggest that population cardiovascular health should improve by implementing the 2013 guideline [Stone et al. 2014].
In 2014, the Veterans Administration and Department of Defense published a cholesterol guideline that had two major differences from the 2013 guideline [Downs and O’Malley, 2015]. First, the 2013 guideline included a strong recommendation for high-intensity statins in subgroups of eligible patients, for example, clinical ASCVD and low-density lipoprotein cholesterol (LDL-C) at 4.9 mmol/l or higher [Stone et al. 2014], whereas the 2014 guideline recommended moderate-dose statin for all statin-eligible adults largely over safety concerns with high-dose statins. Second, the 2013 guideline has a strong recommendation for treating adults with ASCVD10 ⩾ 7.5%, while the 2014 guideline reserves clear advice for statins to adults with ASCVD10 > 12% [Stone et al. 2014; Downs and O’Malley, 2015].
Evidence that high-intensity statins lower LDL-C further and prevent more ASCVD than moderate-intensity statins is strong, especially for coronary heart disease death and nonfatal myocardial infarction, and fatal and nonfatal stroke [Stone et al. 2014; Mills et al. 2011]. Recent evidence supports the notion that greater percentage reductions in LDL-C prevent more ASCVD [Cannon et al. 2015; Robinson et al. 2015; Sabatine et al. 2015; Bangalore et al. 2015]. Our study explores the potential for preventing ASCVD in a diverse practice improvement network in South Carolina, USA. MyHeathFirstNetwork (MyHFN), a clinically integrated network in the Upstate of South Carolina, is the largest member of that network. As a prelude to providing a recommendation to the board of directors for MyHFN, the Quality and Care Model Committee of myHFN requested an analysis of the relative benefits and risks of the 2013 and 2014 cholesterol guidelines when applied to statin-eligible but untreated adults [Egan et al. 2015].
Methods
Human subjects
This study used electronic health data from patients at approximately 400 clinical sites in the Care Coordination Institute quality improvement network. Data were de-identified by patient, provider, and practice. Some patients were included in a prior report on the 2013 guideline [Egan et al. 2015]. Each clinical partner in the Care Coordination Institute signed an approved Business Associate Agreement, which permits use of de-identified data for research.
Inclusion and exclusion criteria
The primary analysis included adults aged 21–80 years with a minimum of one valid blood pressure (BP), lipid profile, and medication for any disease state as well as cigarette smoking, cardiovascular disease, and diabetes status, between 1 January 2012 and 30 June 2015. Exclusion criteria were limited to failure to meet any inclusion criteria, congestive heart failure, estimated glomerular filtration rate lower than 15 ml/1.73 m/min, that is, stage 5 chronic kidney disease, or a diagnosis of drug or alcohol abuse.
Operational definitions
BP (mmHg) at the most recent visit was used to calculate ASCVD10 risk. A valid BP was defined as systolic BP of 60–300, diastolic BP of 30–240, and systolic BP greater than diastolic BP.
LDL-C was calculated as total cholesterol – [high-density lipoprotein cholesterol (HDL-C) + triglycerides/5] [Friedwald et al. 1972]. If triglycerides were higher than 4.5 mmol/l, then LDL-C was not calculated. A valid LDL-C value was defined by the range 0.5–18.1 mmol/l. Valid HDL-C was defined by values of 0.05–3.6 mmol/l.
ASCVD10 risk was calculated using methods from the 2013 guideline [Stone et al. 2014]. The risk calculation was based on sex (male, female), race (White, Black, other), ages 40–79 years, total and HDL-C, systolic BP, hypertension treatment (yes/ no), diabetes (yes/no), and current smoking status (yes/no). ASCVD10 risk was not calculated in adults with ASCVD.
Estimating ASCVD10 reduction with statin therapy relied on two assumptions: (a) ASCVD events would decline 22% for each 1.0 mmol/l reduction in LDL-C [Stone et al. 2014; Cholesterol Treatment Trialists Collaboration, 2010]; (b) LDL-C would decline 35% with moderate-intensity and 50% with high-intensity statin therapy. Estimates are conservative as LDL-C falls 30–50% with moderate-intensity and 50% or more with high-intensity statins [Stone et al. 2014].
An ASCVD10 risk of 34.5% was assigned to patients with clinical ASCVD. The estimate was based on evidence that adults with clinical coronary heart disease (CHD) have a 26% 10-year risk of recurrent CHD and that adults with CHD risk equivalent status have a 10-year CHD risk of 20% or higher [LIPID Study Group, 1998; Sacks et al. 1996; Crouse et al. 1995; NCEP, 2002]. The 26% and 20% 10-year CHD event rates in patients with clinical ASCVD were averaged. We assumed risk for any ASCVD event including CHD was 50% greater than CHD risk alone, that is, 23% × 1.5 = 34.5%. The assumption that ASCVD risk is 50% greater than CHD risk is conservative as there are approximately 735,000 myocardial infarctions, 795,000 strokes, and 185,000 arterial bypass or lower extremity amputations for vascular disease in the USA annually [CDC, 2015; Million Hearts, 2015; Goodney et al. 2009; Limb Loss Resource Center, 2015].
Defining statin-eligible adults for each guideline and mutually exclusive categories was determined in a sequential manner (Table 1). When more than one dose of statin was recommended, we estimated the proportion within each group that would receive each dosing level. In the 2013 guideline, for adults with diabetes and ASCVD10 risk ⩾7.5%, we assumed 50% would receive moderate-intensity (1A), while 50% would receive high-intensity statins (IIaB), given greater reduction in ASCVD with benefit >> risk. In nondiabetic adults with ASCVD10 risk ⩾7.5%, we assumed that 75% would receive a high-dose statin (1A for both moderate-intensity and high-intensity), while 25% would receive moderate-intensity statin.
Criteria for defining adults eligible for cholesterol-lowering therapy according to the 2013 and 2014 cholesterol guidelines.

I = benefit >>> risk; A = multiple randomized clinical trials or meta-analyses.
IIa = benefit >> risk; B = single randomized trial or nonrandomized studies.
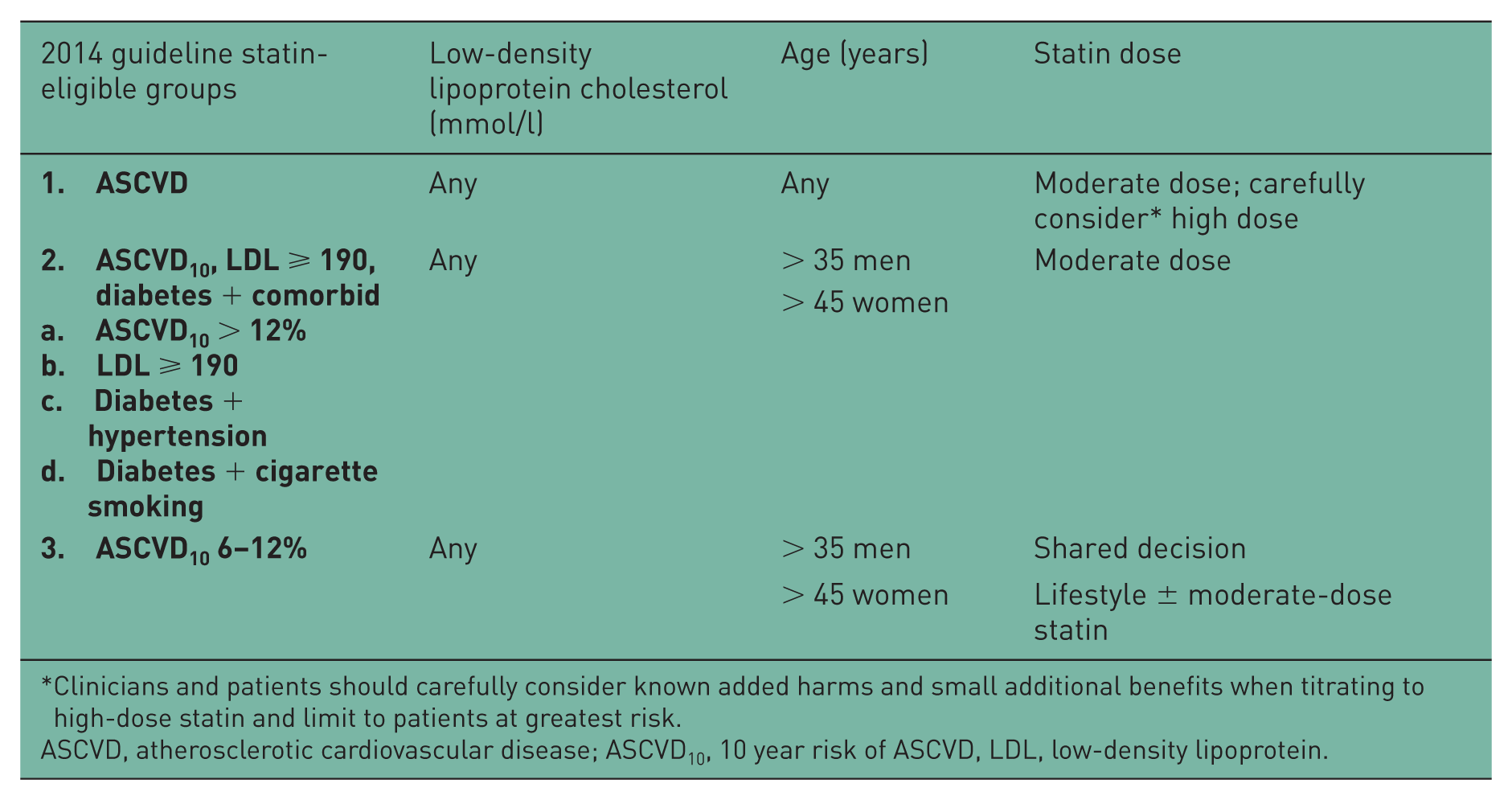
Clinicians and patients should carefully consider known added harms and small additional benefits when titrating to high-dose statin and limit to patients at greatest risk.
ASCVD, atherosclerotic cardiovascular disease; ASCVD10, 10 year risk of ASCVD, LDL, low-density lipoprotein.
In the 2014 guideline, clinicians were advised to prescribe moderate-dose statins for patients with ASCVD and to consider carefully added harms and small additional benefits when titrating to a high dose. We assumed 75% of patients would receive moderate-dose and 25% high-dose statins. The other groups were assumed to receive recommended moderate-dose statins.
Data reporting and analysis
Descriptive statistics were generated for adults with and without a statin prescription. Analyses were conducted including all statin-eligible adults and when excluding a low-risk group where the recommendation for statins was less compelling. The Student’s t-test was applied for continuous variables and the chi-square test was used for categorical variables. SAS Enterprise Guide 7.1 was used for all analyses with a priori two-tailed p < 0.05 denoting statistical significance.
Results
Among 1,580,860 adults aged 21–79 years with an office visit between 1 January 2013 and 30 June 2015, 315,508 (approximately 20%) met inclusion criteria for assessing statin eligibility (Figure 1). Reasons for exclusion in a sequential, stepwise fashion were missing gender designation (15,744 [1.0%]), lack of a complete lipid profile (998,428 [63.2%]), end-stage renal disease (7852 [0.5%]), congestive heart failure (19,818 [1.3%]), and alcohol or drug abuse (68,546 [4.3%]). Of the remaining 470,472 patients, 154,964 (32.9%) were on statins.
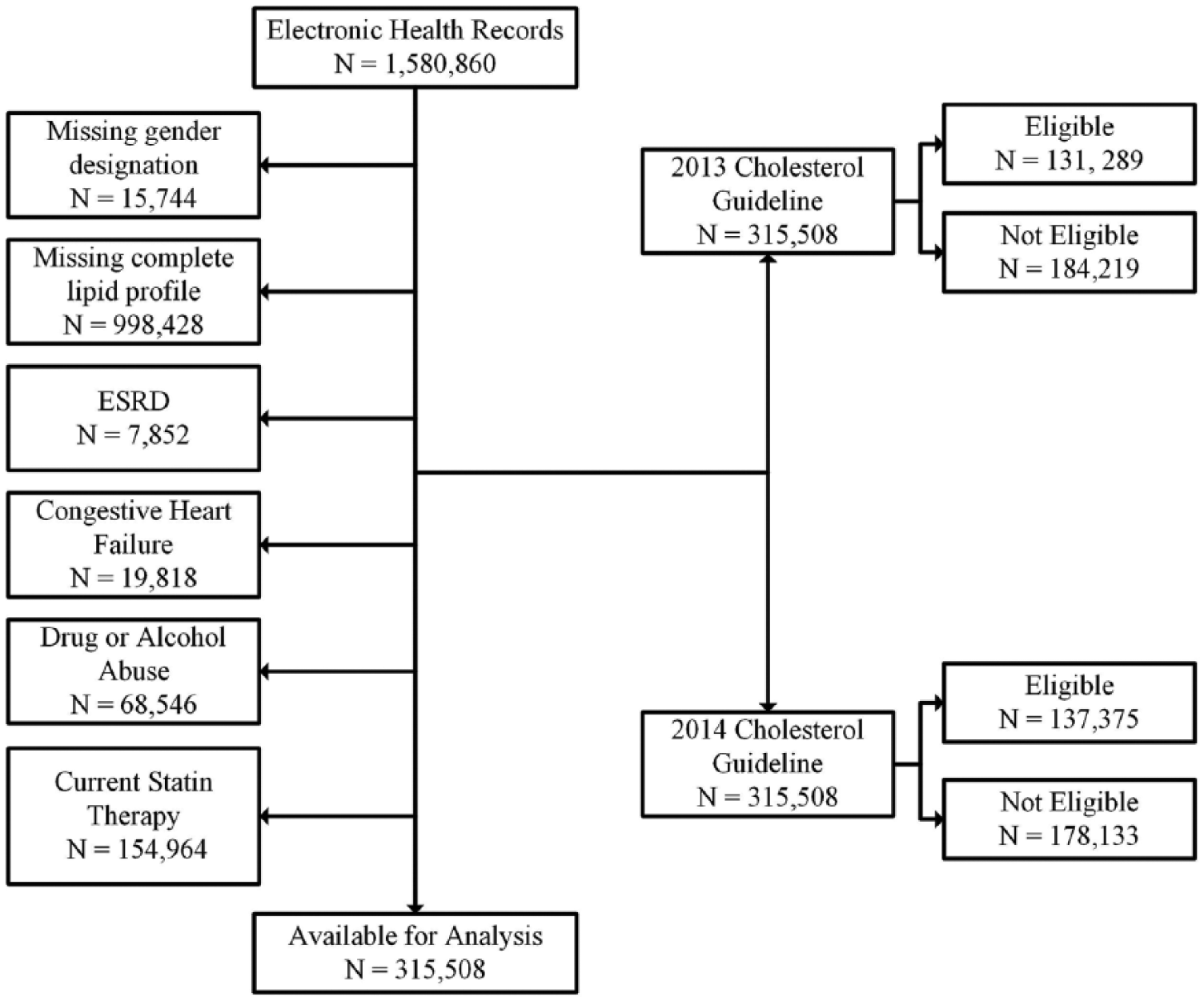
Process for selecting adults not on statins who are statin-eligible by the 2013 or 2014 cholesterol guideline.
Adults on statins were older and statin therapy was more likely to be prescribed for men than women (Table 2). Those on statins were more likely to have diabetes, hypertension, and ASCVD. The percentage of cigarette smokers in both groups was similar, although statistically significant given the large sample size. Systolic BP was higher in adults prescribed statins, whereas diastolic BP, total C, HDL-C and LDL-C were higher among adults not prescribed statins.
Characteristics of adult patients by current statin therapy.

Data are presented as mean ± standard error unless otherwise specified. ASCVD, atherosclerotic cardiovascular disease; ASCVD10, 10 year risk of ASCVD; C, cholesterol; DBP, diastolic blood pressure; HDL, high-density lipoprotein; LDL, low-density lipoprotein; SBP, systolic blood pressure.
In adults not on statins, 41.6% (n = 131,289) were eligible according to the 2013 guideline and 43.5% (n = 137,375) were eligible according to the 2014 guideline (Table 3). Applying the 2013 guideline, the largest proportion of statin-eligible individuals comprised adults without diabetes who had an absolute ASCVD10 risk ⩾ 7.5% followed by individuals with clinical ASCVD. These same groups also contributed more than other groups to absolute numbers of ASCVD events expected over 10 years before and with statin therapy. The smallest absolute risk reduction and largest number needed-to-treat (NNT) was seen in diabetics with ASCVD10 < 7.5%, that is, a 0.9% absolute risk reduction and NNT 116. For the total statin-eligible group, absolute risk reduction was 5.2% with NNT 19. Removing the low-risk group with a IIaB recommendation for treatment, that is, patients without diabetes and ASCVD10 risk 5–7.5% increased absolute risk reduction to 5.9% and reduced NNT to 17. The patients with diabetes and risk of lower than 7.5% were retained in the analysis given a 1A recommendation, despite an NNT of 116.
Predicted atherosclerotic cardiovascular disease events and number needed to treat among statin-eligible but currently untreated adults using the 2013 or the 2014 cholesterol guideline.

ASCVD, atherosclerotic cardiovascular disease; ASCVD10, 10 year risk of ASCVD; DM, diabetes mellitus; LDL, low-density lipoprotein.
Applying the 2014 guideline, more than 50% of statin-eligible adults fell in the middle category of ASCVD10 risk > 12% or LDL-C ⩾ 190, or diabetes with hypertension or smoking. This group had an absolute risk reduction of 4.6% and NNT 22. The absolute risk reduction among patients eligible for a statin was 4.3% with NNT 23. Removing the lowest risk group, that is, those with an ASCVD10 risk of 6–12%, resulted in a greater absolute risk reduction of 5.2% with NNT 19.
Discussion
Statins are efficacious for primary and secondary ASCVD prevention [Taylor et al. 2013; Stone et al. 2014]. The Quality and Care Model Committee for MyHFN requested a comparative analysis of the 2013 and 2014 cholesterol guidelines before offering a recommendation to the board of directors for implementation across the network. The principal objectives of this analysis were to compare the number of adults eligible for statins and estimate the number of ASCVD events prevented and NNT to prevent an ASCVD event with the 2013 and 2014 guidelines. Adverse effects of high-dose versus moderate-dose statins were considered.
The first comparison of the two cholesterol guidelines assumed all eligible adults would receive the recommended dose of statin. Of note, a larger percentage of adults currently not on statins were eligible for treatment by the 2014 guideline (43.5%) than the 2013 guideline (41.6%). In this scenario, the 2013 guideline treated 1.9% fewer adults currently not on a statin, yet was estimated to prevent more ASCVD with a lower NNT (19 versus 23) than the 2014 guideline.
The second scenario excluded a low-risk group with less compelling recommendations for statin therapy from each guideline. For the 2013 guideline, adults without diabetes and ASCVD10 risk 5.0–7.5% were removed (16.0% of statin-eligible adults). For the 2014 guideline, adults with ASCVD10 6–12% were removed (28.1% of statin-eligible adults). In this analysis, the 2013 guideline treated 11,465 more adults, yet prevented an estimated 1315 more ASCVD10 events, and had a lower NNT of 17 versus 19. The 2013 guideline also appears more efficient than the 2014 guideline for ASCVD prevention when excluding adults with less compelling recommendations for statins.
Two main differences between the 2013 and 2014 guidelines account for variance in estimated ASCVD events prevented and NNT. First, the 2013 guideline includes a strong (1A) recommendation for treating three groups of adults with high-intensity statins (Table 1), which includes adults without diabetes and ASCVD10 risk ⩾ 7.5% (moderate-high intensity statins) [Stone et al. 2014]. Evidence that high-dose statins reduce LDL-C more than low-dose statins is strong [Stone et al. 2014; Mills et al. 2011; Egan et al. 2015; Preiss et al. 2011]. Although the 2013 and 2014 guidelines did not provide targets for LDL-C, recent evidence confirms the impression that a greater percentage LDL-C reduction is better for ASCVD outcomes [Cannon et al. 2015; Robinson et al. 2015; Sabatine et al. 2015]. Statin dose and percentage LDL-C reduction emerge as more important determinants of outcomes than achieving a target LDL-C lower than 1.8 mmol/l [Sabatine et al. 2015]. Thus, our analysis may have underestimated the benefits of high-dose versus moderate-dose statins for ASCVD reduction, since all of the advantage was attributed to the percentage LDL-C reduction.
In contrast, the 2014 guideline provides a qualified recommendation that patients with ASCVD and their clinicians carefully examine the known added harms and small additional benefits, when considering high-dose versus moderate-dose statins [Downs and O’Malley, 2015]. Second, the 2013 guideline provides a strong (1A) recommendation for statins in adults with ASCVD10 ⩾7.5%. In contrast, the 2014 guideline reserves advice for statins to adults with ASCVD10 >12%. Given different perceptions of risk and benefit between the 2013 and 2014 guidelines, a review of evidence is prudent.
A 2011 meta-analysis, which included 10 randomized-controlled trials, noted that high-intensity versus moderate-intensity statins prevented more CHD death and nonfatal myocardial infarction with risk ratio (RR) 0.90 (95% confidence interval [CI] 0.86–0.96), nonfatal myocardial infarction (RR 0.82, CI 0.76–0.89), and fatal and nonfatal stroke (0.86, CI 0.77–0.96) [Mills et al. 2011]. However, all-cause mortality (RR 0.92, CI 0.83–1.03) and CVD death (RR 0.89, CI 0.78–1.01) were not significantly reduced. In another analysis, the 5-year NNT with high-intensity versus moderate-intensity statins to prevent a major vascular event was 31 versus a number needed-to-harm (NNH) of 100 for diabetes [Preiss et al. 2011]. With regard to excess of all events leading to discontinuation with high-intensity versus moderate-intensity statin, the NNH is 47. Rhabdomyolysis, a rare event, was not different [Silva et al. 2007; LaRosa et al. 2005].
Among adults not prescribed statins, implementing either the 2013 or 2014 guideline is projected to reduce ASCVD. The MyHFN Quality and Care Model Committee recommended implementation of the 2013 guideline across our clinically integrated network in the South Carolina Upstate based on the benefit-to-risk assessment presented. Given proven benefits of statins and relative safety for reducing ASCVD [Taylor et al. 2013; Stone et al. 2014; Mills et al. 2011; Preiss et al. 2011; Silva et al. 2007; LaRosa et al. 2005], it is important to mitigate barriers to implementing and adhering to these guidelines.
The greatest barrier was lack of a lipid profile to assess ASCVD10 risk in 63.2% of patients. A previous report indicated that roughly two-thirds of all adults aged 20 years or older reported a cholesterol measurement in the past 5 years. The question did not specify whether cholesterol was checked by their clinician or at a health screen, which may not have included a full lipid profile or inclusion in their electronic health record data. The requirement for a fasting sample to obtain an accurate LDL-C is a barrier [Downs and O’Malley, 2015]. In fact, more than 50% of adults in the National Health and Nutrition Examination Surveys do not have an LDL-C, whereas more than 95% have a non-HDL-C [Egan et al. 2013]. Moreover, non-HDL-C, calculated from total and HDL-C, does not require fasting and is a stronger predictor of cardiovascular outcomes than LDL-C [Ramjee et al. 2011].
Health-system barriers such as lack of care coordination contribute to geographic variations in patient nonadherence [Fang et al. 2014; Sengstock et al. 2012]. The growth of accountable care organizations combined with healthcare payment reform, provide incentives for integrated care and case management that improve health and prevent costly disease. Recent studies noted improvements in guideline implementation, yet barriers remain including clinician disagreement and uncertainty with recommendations, clinical inertia, and time [Deedwania, 2015; Pronovost, 2013]. Team-based care and engaging the healthcare delivery team in guideline development can identify and minimize barriers [Pronovost, 2013; Martin et al. 2014]. Computerized point-of-care reminders, guideline implementation checklists, and other information support systems can improve physician performance and prescribing behaviors [Fang et al. 2014]. Numerous patient factors can affect adherence including race/ethnicity, cost of medications, comorbidities as well as trust in, and communication with, their healthcare providers [Chakraborty, 2013; Cheetham et al. 2013; Lewey et al. 2013]. One modifiable variable that improved statin adherence and cardiac outcomes in Medicare beneficiaries was prescribing generic rather than proprietary statins [Gagne et al. 2014].
Limitations of this analysis include a regional, clinic-based rather than national, population-based sample. Thus, implications beyond the population studied are limited. Healthcare professionals that serve populations with different cardiovascular risk characteristics or who use different assumptions on the relative effectiveness and safety with moderate-intensity versus high-intensity statins may prefer the 2014 guideline. Moreover, the majority of adults did not have a lipid profile to estimate risk, so the number of adults that could benefit from statins is likely larger than our data suggest. Given physician resistance to prescribing and patient experience of adverse effects or other reasons for resistance to long-term adherence with statin therapy, the predicted (versus actual) benefits of statin therapy on ASCVD events would be less than projected. Finally, data on previous statin therapy in patients currently not prescribed statins were not reliably available, that is, some untreated patients may be intolerant of statins.
In summary, implementing either the 2013 or 2014 cholesterol guideline in statin-eligible but currently untreated adults would likely reduce clinical ASCVD events. We prefer the 2013 guideline based on our benefit-to-risk assessment among patients receiving care in healthcare clinics and systems in southeast USA participating in our quality-improvement network. The approach described may be useful to other health systems and quality-improvement organizations when assessing the comparative effectiveness and safety of different guidelines prior to implementation in the patient population they serve.
Footnotes
Acknowledgements
The authors appreciate the essential support provided by David Ramsey and Shaun Wagner for building and maintaining the Care Coordination Institute clinical data repository and Lauren Henslee for logistical support with the publication. We are indebted to the physicians and staff in clinics and health systems that participate in the Care Coordination Institute.
Funding
This research was supported in part by funding from the Centers for Disease Control through the South Carolina Department of Health and Environmental Control.
Conflict of interest statement
BME has received royalties from UpToDate, research support from Medtronic and Quintiles, and income as a consultant from AstraZeneca and Medtronic. None of the other authors has anything to disclose.