
Abstract
Background:
Patients who undergo percutaneous coronary intervention (PCI) for severely calcified coronary lesions have long been known to have worse clinical and economic outcomes than patients with no or mildly calcified lesions. We sought to assess the likely cost-effectiveness of using the Diamondback 360® Orbital Atherectomy System (OAS) in the treatment of de novo, severely calcified lesions from a health-system perspective.
Methods and results:
In the absence of a head-to-head trial and long-term follow up, cost-effectiveness was based on a modeled synthesis of clinical and economic data. A cost-effectiveness model was used to project the likely economic impact. To estimate the net cost impact, the cost of using the OAS technology in elderly (⩾ 65 years) Medicare patients with de novo severely calcified lesions was compared with cost offsets. Elderly OAS patients from the ORBIT II trial (Evaluate the Safety and Efficacy of OAS in Treating Severely Calcified Coronary Lesions) [ClinicalTrials.gov identifier: NCT01092426] were indirectly compared with similar patients using observational data. For the index procedure, the comparison was with Medicare data, and for both revascularization and cardiac death in the following year, the comparison was with a pooled analysis of the Harmonizing Outcomes with Revascularization and Stents in Acute Myocardial Infarction (HORIZONS-AMI)/Acute Catheterization and Urgent Intervention Triage Strategy (ACUITY) trials. After adjusting for differences in age, gender, and comorbidities, the ORBIT II mean index procedure costs were 17% (p < 0.001) lower, approximately US$2700. Estimated mean revascularization costs were lower by US$1240 in the base case. These cost offsets in the first year, on average, fully cover the cost of the device with an additional 1.2% cost savings. Even in the low-value scenario, the use of the OAS is cost-effective with a cost per life-year gained of US$11,895.
Conclusions:
Based on economic modeling, the recently approved coronary OAS device is projected to be highly cost-effective for patients who undergo PCI for severely calcified lesions.
Introduction
Patients with severely calcified lesions who undergo percutaneous coronary intervention (PCI) have been shown to have worse clinical outcomes compared with patients with no, mildly, or moderately calcified lesions [Bangalore et al. 2011; Bourantas et al. 2014; Généreux et al. 2014; Madhavan et al. 2014], and are associated with considerably greater healthcare utilization and costs [Chambers et al. 2014a]. The Diamondback 360® Coronary Orbital Atherectomy System (OAS) (Cardiovascular Systems Inc., St. Paul, MN, USA), approved in late 2013 by the US Food and Drug Administration (FDA) specifically indicated for the treatment of de novo, severe coronary artery calcification (CAC), represents the first major advance in many years for coronary lesion preparation dedicated to heavily calcified lesions. The pivotal clinical study, the Evaluate the Safety and Efficacy of OAS in Treating Severely Calcified Coronary Lesions (ORBIT II) trial, was a single-arm trial carried out at 49 US sites and included 443 patients [Chambers et al. 2014b], and was the first prospective study to focus exclusively on the treatment of severely calcified coronary lesions.
Given the ongoing changes in healthcare policy and financing in the postreform era, payers, clinicians, patients, and policymakers must increasingly consider both the cost and the clinical effectiveness of therapeutic devices, including not only the initial inpatient or acute care costs but also the postacute care costs over a longer period of time. In addition, as recommended in the recent American College of Cardiology/American Heart Association statement on cost/value methodology [Anderson et al. 2014], it is important to assess societal-level cost and value information. These data are critical for developers of clinical guidelines and performance metrics, as well as for health technology assessment and adoption considerations.
The primary objective of this analysis was to assess the potential cost-effectiveness of the Diamondback Coronary OAS device for severe CAC from a health-system perspective by modeling: (a) the expected cost offsets, both during the acute and postacute care periods; (b) the potential reduction in patient mortality and morbidity; (c) the comparison of mortality and morbidity impacts in relation to the overall cost impact of device use via a cost-effectiveness analysis. Given the lack of a control arm in the pivotal trial, an indirect comparison was made with other clinical trial results and relevant observational data to assess the cost-effectiveness. This economic analysis compared the ORBIT II study population with: (a) a comparison sample of elderly Medicare beneficiaries; (b) a new subanalysis of data from the Harmonizing Outcomes with Revascularization and Stents in Acute Myocardial Infarction (HORIZONS-AMI)/Acute Catheterization and Urgent Intervention Triage Strategy (ACUITY) trials pooled (H-A/AP) analysis that was published recently [Généreux et al. 2014]. This study compared the cost of the OAS device with potential savings that may be attributed to lower stent-procedure costs and lower revascularization rates in treated patients as well as the projected impact on patient mortality.
Methods
Study design
In October 2013, the FDA approved the OAS technology for coronary use. The covered indication is “to facilitate stent delivery in patients with coronary artery disease (CAD) who are acceptable candidates for percutaneous transluminal coronary angioplasty (PTCA) or stenting due to de novo, severely calcified coronary artery lesions” [FDA, 2013]. The approval was based on a single-arm study (ORBIT II), for which safety and efficacy were compared with historical data for a range of major adverse cardiac events (MACEs) at 30 days postprocedure [Chambers et al. 2014b]. The study met both endpoints: efficacy (procedural success, 88.9% versus 82% target; 95% confidence interval [CI], 85.5–91.6) and safety (freedom from 30-day MACEs, 89.6% versus 83% target; 95% CI, 86.7–92.5) [Chambers et al. 2014b].
In the absence of a head-to-head trial and long-term follow up, this assessment of the potential cost-effectiveness of the intervention was based on a modeled synthesis of relevant, available data, both clinical and economic, in comparison with the current standard of care for severely calcified lesions, which is the use of balloon angioplasty to prepare the stent-placement site. Although a rotational atherectomy device is available, it was likely used in only a small percentage of cases. A simple cost-effectiveness model was used to project the essential elements of the likely economic impact. To estimate the net cost impact (the numerator in the cost-effectiveness ratio), the cost of using the OAS in elderly (⩾ 65 years) Medicare patients with de novo, severely calcified lesions was compared to any cost offsets. The potential cost offsets due to OAS use fall into three major categories: (a) reduced procedural costs related to stent implantation; (b) reduced revascularization events in the 30 days following the initial hospitalization; (c) reduced revascularization events between day 30 and 1 year. Effectiveness (the denominator in the cost-effectiveness ratio) was measured in two ways: (a) patient survival at the end of 1 year; (b) life-years gained over a lifetime horizon.
To a considerable extent, the structure and limitations of the available data defined the type and breadth of the economic comparison that was made at this early stage of commercialization. ORBIT II patients were followed through 1 year postprocedure. In addition, a new International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) diagnosis code (414.4) for CAC was instituted in the last quarter of 2011, and data for elderly Medicare patients through to the end of 2012 (the latest period for which these data are available) were examined. Given the small numbers, it was not possible to estimate postprocedure revascularization in the Medicare sample: instead, a new subanalysis of the elderly population from the H-A/AP sample was used [Généreux et al. 2014]. This combination of information allowed us to compare the two groups for 1 year postprocedure.
Economic model
The cost-effectiveness analysis was based on a mathematical model that integrated data on costs and MACE rates from several sources in order to compare the performance of the OAS technology versus standard treatment in stenting de novo, severely calcified lesions in a specific set of patients, i.e. elderly Medicare patients. The analysis was from the perspective of a health system, which considers direct costs as well as patient outcomes. Given current data limitations, the focus was on the key drivers for which evidence is currently available.
Figure 1 provides a simple schematic of the comparison. Elderly OAS patients from the ORBIT II trial were compared with a similar sample of Medicare patients with de novo, calcified lesions for the index stent placement and with the H-A/AP sample following the index procedure. Thus, the cost comparison was constructed as the sum of three intervals: (a) the initial index procedure; (b) patient status at 30 days following the procedure; (c) patient status from the period between postprocedure day 31 and 1 year. The primary effectiveness endpoints were based on the survival difference at 1 year following the procedure and were measured in two ways: cost per ‘life saved’ and cost per ‘life-years gained’. The latter required a projection of expected lifetime for a typical (median) patient (a 74-year-old man) in the ORBIT II elderly subsample.

Cost and effectiveness models.
Cost of the OAS device
The manufacturer’s suggested list price of the OAS device in this analysis was set at US$3795 and did not vary in the analysis. It is a disposable, one-time-use device.
Costs of stent-implantation procedure
To assess the impact on medical care resource use and cost, elderly (age ⩾ 65 years) ORBIT II patients were compared with a sample of elderly Medicare coronary-stent patients with reported CAC. As shown in Table 1, the ORBIT II and Medicare comparison samples were similar in terms of baseline characteristics with the exception of the Charlson comorbidity index score [Delong et al. 1997]. This may be due, in part, to coding differences in the two datasets: the documentation of comorbidities in the clinical trial database was less thorough and clear because only those reported during the index hospitalization were included. A generalized linear model with a gamma distribution was used with the following covariates: age group, gender, and Charlson index, and censored costs were taken into account using the Basu-Manning method [Basu and Manning, 2010].
Baseline characteristics.
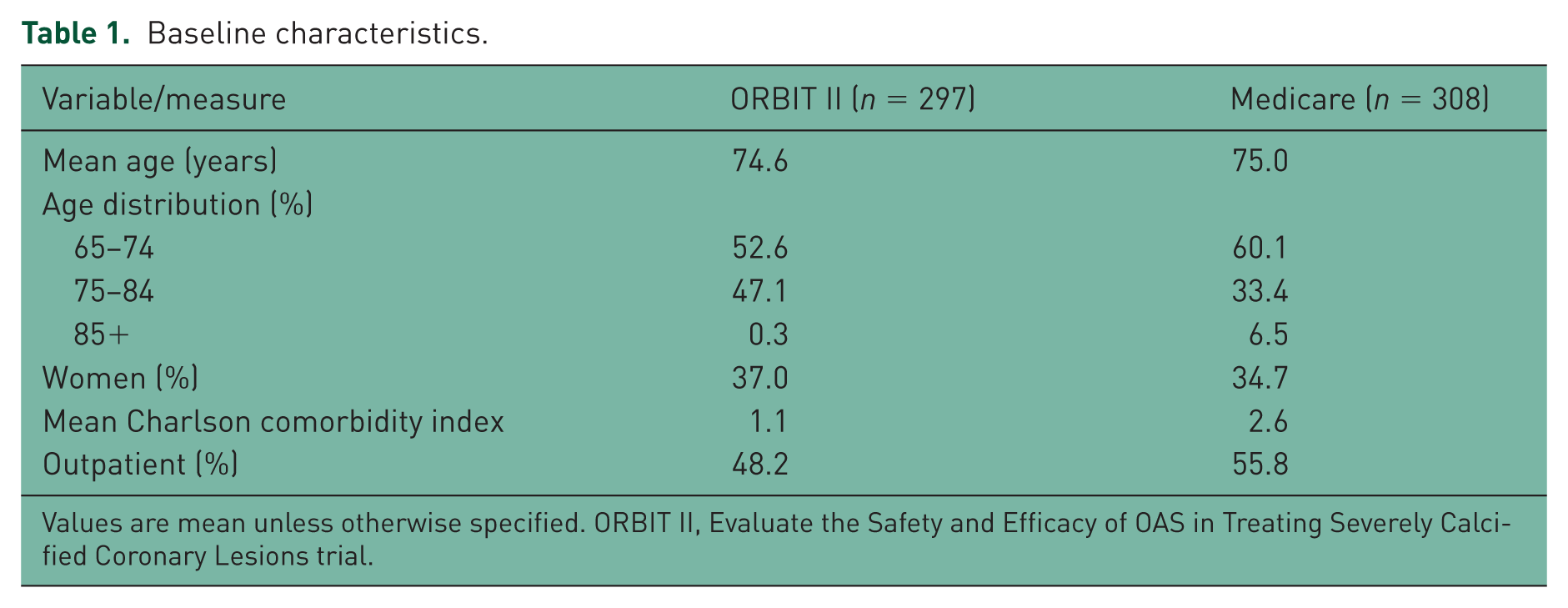
Values are mean unless otherwise specified. ORBIT II, Evaluate the Safety and Efficacy of OAS in Treating Severely Calcified Coronary Lesions trial.
ORBIT II patients
Uniform inpatient billing records were obtained for the elderly ORBIT II patients (n = 297) and compared with a sample (n = 308) of elderly Medicare coronary-stent patients with reported CAC. Inpatient charges were adjusted to costs using hospital-specific, cost-to-charge ratios.
Medicare patients
The Medicare comparison sample was drawn from the 100% Standard Analytical File (SAF) for the period September 2011 through December 2012. While a new ICD-9-CM diagnosis code (414.4) was introduced late in 2011 for severe CAC, actual documentation of CAC via administrative coding practice has lagged. For example, only 1.7% of patients with de novo PCIs were reported to have CAC, and the significant degree of underreporting of CAC in the Medicare population has recently been described [Garrison et al. 2015]. This is the first published cost-effectiveness analysis that relies to any extent on the reporting and use of this ICD-9 code for de novo PCI patients in the elderly Medicare population.
The principal data sources for the control-arm index procedure cost and survival analyses were from the Medicare SAFs. The SAFs contain seven datasets with detailed claims information about healthcare services rendered to Medicare beneficiaries in fee-for-service Medicare. SAFs were available for institutional (e.g. inpatient, outpatient, skilled nursing facility, hospice, or home health agency) and noninstitutional (e.g. physician and durable medical equipment providers) claim types. Data were organized at the claim level and included basic beneficiary demographic information, date of service, diagnosis and procedure code, provider number, and reimbursement amount. Two SAF databases were used: the Medicare 5% SAF and 100% SAF. The 5% random sample of beneficiaries included all relevant claims (e.g. inpatient, outpatient, physician, durable medical equipment, etc.) except drugs, which are tracked and reported separately via Medicare Part D and not readily accessible for evaluation. The 100% files include inpatient and outpatient claims only and include all fee-for-service beneficiaries; Medicare Advantage program members are not included.
For this comparison, a special subsample (n = 308) was defined from the 100% SAF that included all hospitals (n = 17) that coded more than 10% of their PCI patients as having CAC (using code 414.4). This sample was used as the control arm under the assumption that this subset was more diligent and accurate in their coding.
H-A/AP data
For the indirect comparison of postindex MACE rates, a new subanalysis, based on the elderly population from the H-A/AP sample [Généreux et al. 2014], was used for patients with severely calcified coronary lesions. This included 205 patients with severe CAC. The mean age was 73.7 years, somewhat older than the average age of 71.4 years seen in the ORBIT II study. Patients included in the H-A/AP study presented with unstable angina, moderate- or high-risk non-ST-segment elevation acute coronary syndrome (ACS), or ST-segment elevation myocardial infarction (MI). As shown in the Supplemental Appendix Table, the ORBIT II and H-A/AP samples had significant and comparable histories of comorbidities, such as diabetes, hypertension, and hyperlipidemia.
MACE rates, target lesion revascularization/target vessel revascularization
For the OAS arm, estimated MACE rates were drawn from the ORBIT II 1-year follow-up analysis [Généreux, 2015]. Estimates for the standard therapy arm were based on the subanalysis of the elderly population patients with severely calcified coronary lesions from the H-A/AP sample However, to simplify the comparison and the model, only differences in target lesion revascularization (TLR)/ target vessel revascularization (TVR) were compared since most MIs would occur during the index procedure.
MACE costs
The cost of MACEs, specifically for revascularization (TLR/TVR), was estimated using the Medicare SAF samples. The 100% SAF sample provides estimates of inpatient and outpatient facility costs, but it does not include physician fees. Inpatient charges were transformed to costs using hospital-specific, cost-to-charge ratios. The cost offsets for days 1–30 and days 31–365 were conservatively based on the difference in revascularization between ORBIT II and H-A/AP. In addition, a conservative episode-cost estimate of US$20,000 was used, based on estimates of facility costs in the Medicare SAF analyses of PCI patients, but this did not include cardiologist or other provider fees.
Health outcomes: survival
For ORBIT II patients, cardiac death was used as the 1-year outcome. For the standard treatment, the estimate of cardiac death was based on the elderly population patients with severely calcified coronary lesions from the H-A/AP sample. For the life expectancy calculation, the life-years gained estimate was based on the median age and gender of an elderly PCI patient (i.e. a 74-year-old man) who would normally have an expected an additional lifetime of 11.5 years. This was then adjusted down to 9.5 years after discounting at 3% per annum, which is the standard practice in cost-effectiveness analyses with a lifetime patient horizon [Gold et al. 1996]. In addition, this is within the expected range of life expectancy (5–11 years) for patients with cardiovascular disease in this age range (Peeters et al. 2002).
Cost-effectiveness
The parameter estimates needed to perform the cost-effectiveness analysis are presented in Table 2.
Key model parameter inputs and assumptions.

HORIZONS-AMI/ACUITY, Harmonizing Outcomes with Revascularization and Stents in Acute Myocardial Infarction/Acute Catheterization and Urgent Intervention Triage Strategy trials; MACE, major adverse cardiac event; OAS, orbital atherectomy system; ORBIT II, Evaluate the Safety and Efficacy of OAS in Treating Severely Calcified Coronary Lesions trial; TLR/TVR, Target Lesion Revascularization/Target Vessel Revascularization.
Sensitivity and scenario analyses
With the exception of the price of the OAS device, all the parameters in the model are subject to some uncertainty; each was addressed by varying the individual parameters within a range of low to high values. The lower and higher values scenarios vary based on the assumption that total cost offsets are lower by 25% or higher by 25%. In addition, the base-case cardiac-mortality differential of 2.6% was varied to 1% in the low-value scenario, and 3% in the high-value scenario. A one-way sensitivity analysis was carried out to identify key drivers of the results. In addition, a probabilistic sensitivity analysis was conducted using the Monte Carlo simulation, varying all of the parameters. Input ranges for sensitivity analysis were estimated at +/- 25%. Normal distributions were assigned to all probabilities and costs. Means and 95% CIs for each of the posterior distributions were computed on the basis of 5000 iterations.
Results
Stent implantation
As shown in Table 3, considering both inpatient and outpatient procedural costs, unadjusted mean costs were lower by US$3198 (p = 0.003) in ORBIT II patients compared with similar Medicare patients. After adjusting for differences in age, gender, and comorbidities, the ORBIT II mean costs were 17% lower (approximately US$2700; p < 0.001). Both unadjusted and adjusted costs are shown in Figure 2. Mean length of stay in hospital was lower in the ORBIT II arm by about 1 day. The lower inpatient costs in the ORBIT II trial were due, in part, to fewer complications (including the occurrence of MACEs), which would lead to a longer hospitalization, and any reductions in the use of other supplies, such as guide wires, would be reflected as well.
Inpatient and outpatient facility costs and length of stay: ORBIT II versus Medicare 100% subsample.

ORBIT II, Evaluate the Safety and Efficacy of OAS in Treating Severely Calcified Coronary Lesions trial; SD, standard deviation.

Stent episode costs: Evaluate the Safety and Efficacy of OAS in Treating Severely Calcified Coronary Lesions (ORBIT II) trial versus Medicare 100% subsample. ORBIT II, Evaluate the Safety and Efficacy of OAS in Treating Severely Calcified Coronary Lesions trial.
MACEs and costs
Key components of the MACE rate were significantly lower in the ORBIT II elderly sample when compared with estimates for elderly patients with severely calcified lesions in the H-A/AP sample. As shown in Figure 3, at 1 year, the cumulative percentage experiencing cardiac death was 3.2% in ORBIT II compared with 5.8% in the pooled sample. The cumulative percentage for revascularization was 4.9% in ORBIT II versus 11.3% in the pooled sample, and for MI, it was 11.0% in ORBIT II versus 11.4% in the pooled sample.

One-year major adverse cardiac events (MACEs) and costs: Evaluate the Safety and Efficacy of OAS in Treating Severely Calcified Coronary Lesions trial (ORBIT II) versus Harmonizing Outcomes with Revascularization and Stents in Acute Myocardial Infarction/Acute Catheterization and Urgent Intervention Triage Strategy trials (HORIZONS-AMI/ACUITY) pooled (H-A/AP).
30-day MACEs and costs
It is important to note that some types of MACE episodes in these patients are much more likely to occur during the index procedure than afterwards. In particular, in the ORBIT II trial, nearly all of the MIs occurred during the index procedure. The same breakdown of MACEs (i.e. during index procedure versus postindex) was not available for the H-A/AP data; hence, a direct comparison was not possible. As shown in Table 4, revascularization rates within the 30 days following the procedure were substantially lower for ORBIT II patients versus H-A/AP patients (0.3% versus 3.8%).
Revascularization rate during the first 30 days and days 31–365: ORBIT II versus HORIZONS-AMI/ACUITY pooled elderly samples.
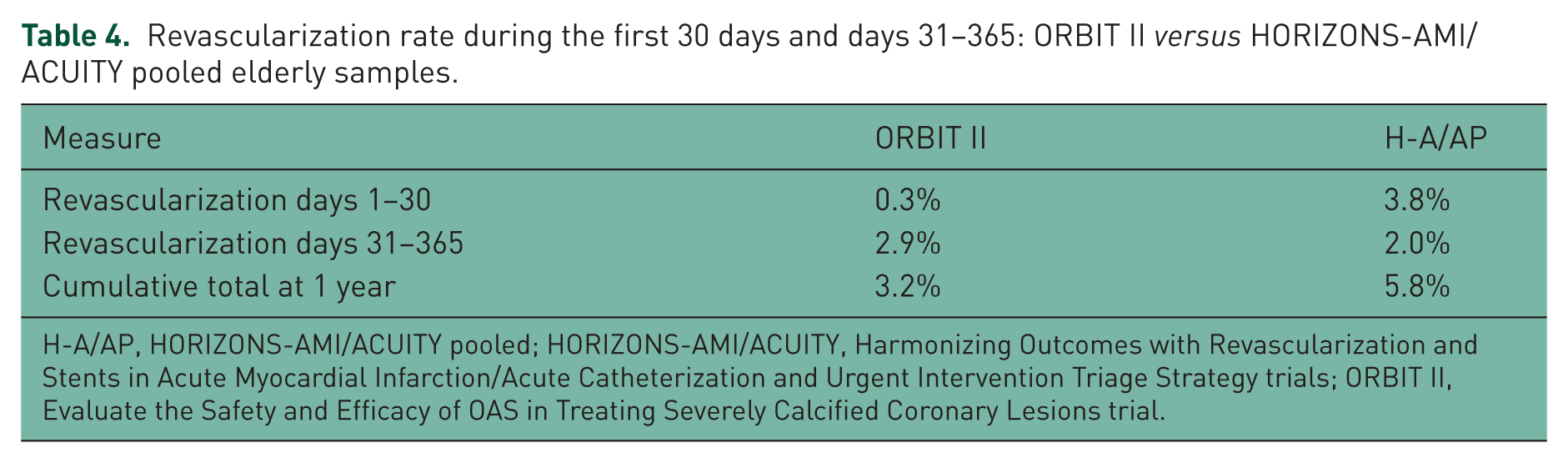
H-A/AP, HORIZONS-AMI/ACUITY pooled; HORIZONS-AMI/ACUITY, Harmonizing Outcomes with Revascularization and Stents in Acute Myocardial Infarction/Acute Catheterization and Urgent Intervention Triage Strategy trials; ORBIT II, Evaluate the Safety and Efficacy of OAS in Treating Severely Calcified Coronary Lesions trial.
31–365-day MACEs and costs
As shown in Table 4, mean revascularization rates in days 31–365 were slightly higher in ORBIT II than in H-A/AP patients, 2.9% versus 2.0%, respectively.
Total first-year costs
The ORBIT II-Medicare comparison indicates substantial cost offsets related to the index procedure episode including associated MACEs. The modeled comparison based on the pooled sample supports cost offsets related to revascularization in the first 30 days. From a facility or health-system perspective, the total projected cost offsets in the first year in this elderly population, on average, would fully cover the cost of OAS technology at US$3795.
Mortality and life-years gained
As shown in Figure 3, cardiac mortality in the overall ORBIT II elderly cohort was 3.2% compared with 5.8% in the H-A/AP analysis cohort. From an economic perspective, this differential amounts to 2.6 lives saved or 29.9 life-years gained for a cohort of 100 patients. Discounting by 3% per annum for time preference, this amounts to 0.247 years per OAS patient, i.e. about one-quarter year per patient.
Cost-effectiveness
Table 5 presents the cost-effectiveness results for both the base case and for alternative low-value and high-value scenarios. In the base case, it is estimated that the use of OAS technology would enable a slight cost savings of about 1.2%. In addition, the average patient would expect to gain 0.247 (discounted) life-years. On average, the documented lower cost with better outcomes, technically termed as ‘dominant’, suggests that the use of OAS technology is the clear treatment of choice. At the more optimistic end of the range, the cost savings could be as high as US$1118 (US$4913 in savings compared with US$3795 for the device). This savings projection strongly supports clinical use of the OAS technology for severely calcified patients, with the average patient gaining 0.36 life-years. Even with more pessimistic assumptions, use of the device offers good value at US$11,895 per life-year gained. This is far below the ‘high-value’ threshold of a US$50,000 cost per healthy life-year [Anderson et al. 2014].
Cost-effectiveness estimates.
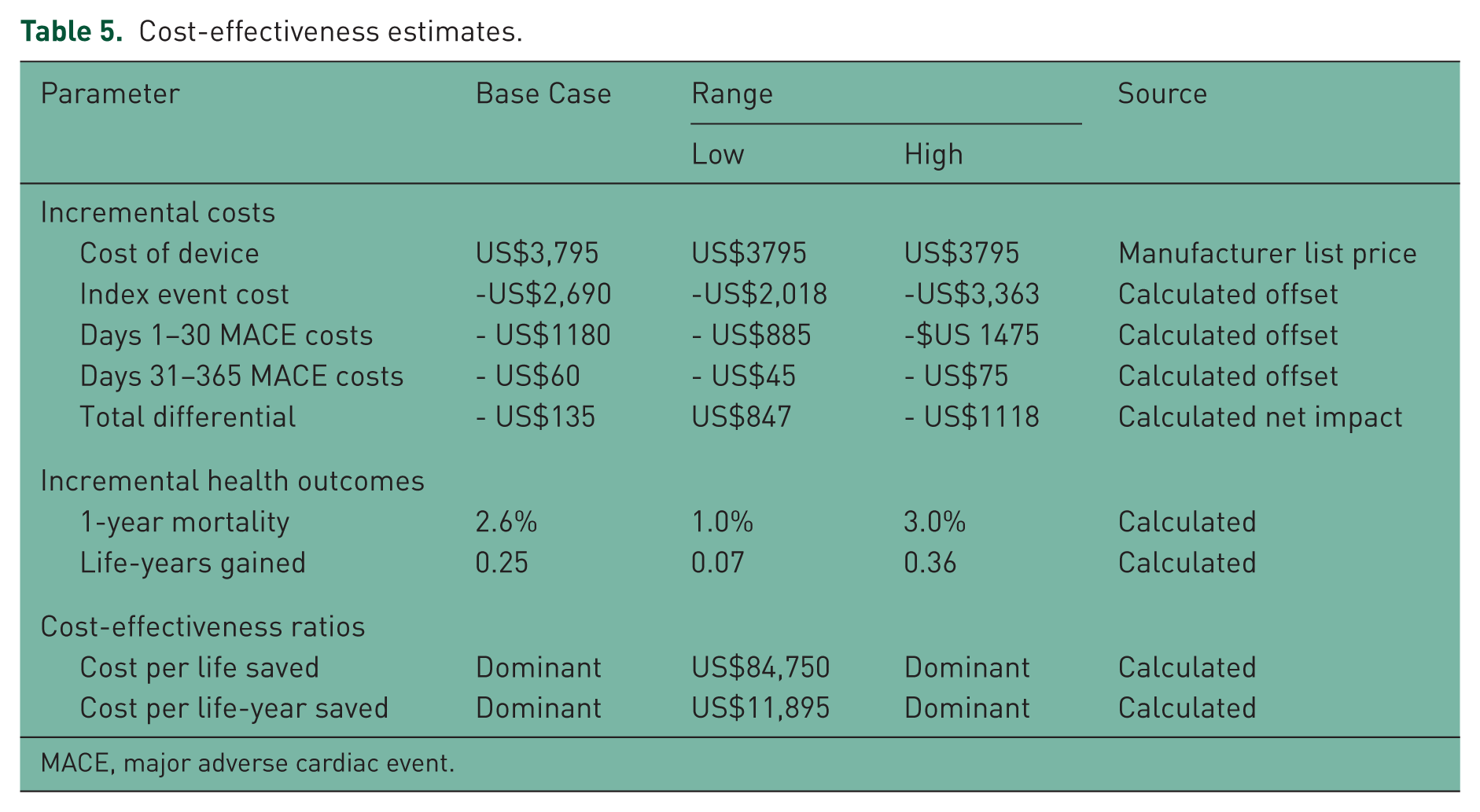
MACE, major adverse cardiac event.
Sensitivity analyses
Figure 4 summarizes the one-way sensitivity analysis in a tornado diagram. Not surprisingly, the two key drivers are the price of the OAS device and the cost offset during the index event. The rates and cost of revascularization are also influential. However, in any case, even with a 25% change (in either direction) of key parameters, the projection suggests that the use of OAS technology is highly cost-effective.

Tornado diagram of one-way sensitivity analysis change in cost-effectiveness ratio with variable uncertainty.
Figure 5 presents the results of the probabilistic sensitivity analysis in a scatterplot of projected cost-effectiveness ratios. The analysis showed that the 95% CI for the incremental cost-effectiveness ratio of OAS technology compared with standard treatment was dominated, US$2657 per life-year. The figure depicts the resulting cost and effectiveness (in life-years) from 5000 simulations of OAS technology and standard treatment. OAS results were dominant, which suggests that OAS technology is less costly and more effective than the standard treatment in 58.5% of simulation cases. Using a conservative (high value) willingness to pay US$50,000 per life-year, OAS technology was projected to be cost-effective and thus high value in approximately 99.9% of simulations [Anderson et al. 2014].

Scatterplot of results of probabilistic sensitivity analysis. WTP, willingness to pay.
Discussion
These parallel, indirect comparisons to the Medicare claims data and to previous stent trials suggest that the additional cost of the OAS technology in treating de novo, severely calcified coronary lesions would likely be offset by other downstream health-system cost savings. These results represent a conservative estimate of potential savings. A less optimistic set of assumptions for OAS technology use suggested a modest increase in overall costs (US$848), but still produced a cost-effectiveness ratio that is deemed to be high value when mortality reductions are considered. Given the expectation of better health outcomes in terms of improved survival and fewer MACE episodes, it is highly likely that this intervention will be cost-effective from a health-system perspective that considers both payer medical care costs and health benefits to patients themselves.
The major cost driver is the projected cost offset due to reduced length of stay in hospital (by avoiding complications) and lower costs during the index procedure itself. The cost differential in the index procedure reflects a variety of possible factors, including fewer in-hospital MACEs (particularly MIs), fewer complications that lead to longer stays, and reduced use of supplies, such as guide wires. The impact on physician costs was not included since neither dataset includes them.
The second major cost consideration was attributed to differences in the postprocedure MACE rate, and particularly the need for revascularization in the remainder of the first year. The H-A/AP analysis of elderly patients showed a higher overall revascularization rate in the first year, but with the major difference appearing in the first 30 days following the index procedure. This would be important to facilities that are at financial risk for the cost of postoperative re-admissions in the first 30 days. The significance of, and reasons for the slightly higher mean revascularization rates in days 31–365 for ORBIT II versus H-A/AP patients are unclear, however, the difference is small and does not greatly affect the overall 1-year differential. The mean age in the ORBIT II trial was 71.4 years [Chambers et al. 2014b], which is slightly less than the 73.7 years in severely calcified patients in the H-A/AP analysis. Older patients in general have worse outcomes. Furthermore, the ORBIT II study may have more patients with stable angina compared with the H-A/AP sample. Patients with unstable angina or acute MI are more likely to have recurring events versus a stable angina population. This could bias the projected savings upwards, though probably only slightly. In any case, the sensitivity analysis demonstrates that, even at the lower bound of the mortality advantage, use of the OAS technology would be highly cost-effective at about US$12,000 per life-year gained. Even with an adjustment for lower quality of life compared with a perfectly healthy person, which was not calculated in this analysis, this cost would be far below the high-value threshold of US$50,000 per quality-adjusted life-year proposed by Anderson and colleagues [Anderson et al. 2014].
This analysis had several limitations. First, there was lack of a direct comparator, as ORBIT II was a single-arm study. Second, coding of CAC in the Medicare data has lagged since its introduction and therefore, was highly likely to have been underreported at the time of this analysis. Third, since the degree or severity of calcification is not always known or estimated, it was unclear how well the Medicare SAF sample compared with the ORBIT II trial. While the retrospective comparison of this cohort has inherent bias, the H-A/AP trials represent the largest cohort of patients with severely calcified lesions ever published. While using different cohorts with different demographic characteristics is a limitation, we believe that these cohorts are the best available population in the current literature, and that they are appropriately matched for calcification severity. Fourth, although the multivariate cost equation for differences in the index PCI is potentially subject to unmeasured confounding, the adjustment for the Charlson index and other measured variables was likely biased downwards due an underestimate of the Charlson index in the ORBIT II sample. Thus, their actual costs are lower than predicted. Fifth, the HORIZONS-AMI [Stone et al. 2008] and ACUITY [Stone et al. 2006] trials enrolled patients with ACS. Patients with ACS have been shown to have worse outcomes than patients with stable angina. In addition, since morbidity-related MACEs are higher with standard therapy, this model likely underestimated the total impact of patient-level, health-status improvements made possible by the OAS technology because it does not capture the negative impact that these events have on a patient’s quality of life. Finally, the assumption about survival impact might be questioned because of the lack of a direct comparison. ORBIT II may have been underpowered to measure this single component of the composite MACE measure.
Conclusion
Relying on comparison of a single-arm trial to historical data, the FDA approved the OAS technology in October 2013 to improve outcomes in difficult-to-treat PCI patients with severely calcified coronary lesions. For this population, this economic modeling analysis suggests that using OAS technology is likely to result in lower inpatient costs, particularly for the initial procedure and during the immediate 30-day follow-up period. Based on economic modeling from the pivotal ORBIT II trial as well as indirect comparisons with other trial and Medicare data, the OAS device likely represents both significant clinical and highly cost-effective improvements in the care of patients with severely calcified lesions undergoing PCI.
Footnotes
Appendix
Baseline characteristics of the ORBIT II and HORIZONS-AMI/ ACUITY pooled study populations.

| Parameter | ORBIT II population |
HORIZONS-AMI/ACUITY population |
|---|---|---|
| 71 | 61 | |
|
|
65 | 73 |
|
|
||
|
|
36 | 24 |
|
|
92 | 62 |
|
|
22 | 23 |
|
|
15 | 13 |
|
|
Chronic kidney disease excluded, acute kidney injury N/A | 17 |
|
|
9 | 6 |
|
|
92 | 62 |
HORIZONS-AMI/ACUITY, Harmonizing Outcomes with Revascularization and Stents in Acute Myocardial Infarction/Acute Catheterization and Urgent Intervention Triage Strategy trials; ORBIT II, Evaluate the Safety and Efficacy of OAS in Treating Severely Calcified Coronary Lesions trial.
Funding
The ORBIT II trial was funded by Cardiovascular Systems, Inc. St. Paul, MN, USA.
Conflict of interest statement
The authors received financial support from Cardiovascular Systems, Inc.