
Abstract
Background:
The aim of this study was to compare the two different directions of tumescent solution delivery (from distal to proximal knee to the saphenofemoral junction [SFJ] or proximal to distal SFJ to the knee) in terms of differences in tumescent volume, number of punctures, and pain and comfort scores of patients.
Methods:
A total of 100 patients were treated with endovenous laser ablation (EVLA) under local anesthesia between August 2013 and October 2013. These 100 patients were divided into two groups. In group 1, tumescent solution was delivered in a proximal to distal direction. In group 2, the tumescent solution was delivered in a distal to proximal direction. In each group, the great saphenous vein (GSV) diameter, delivered total energy, treated GSV length, delivered tumescent volume, number of punctures, and pain and comfort scores were recorded for each patient.
Results:
All patients were treated unilaterally. EVLA was performed with 100% technical success in all patients. There was no difference statistically between group 1 and group 2 according to GSV diameter, delivered total energy, and treated GSV length. Average tumescent volume, number of punctures, and pain scores in group 2 were lower than in group 1 (p = 0.0001; p < 0.05). Also, the average comfort score was higher in group 2 than in group 1 (p = 0.0001; p < 0.05).
Conclusions:
We believe that delivering the tumescent solution in a distal to proximal direction increases the comfort of both patient and surgeon with lower tumescent volume during the EVLA of the GSV.
Introduction
Chronic venous disorder is a very common medical condition affecting the adult population with a prevalence between 5% and 30% although reports have ranged from less than 1% to greater than 70% [Raffetto and Eberhardt, 2010; Beebe-Dimmer et al. 2005]. For more than a century, the classic treatment for saphenous vein insufficiency has been surgical ligation and stripping [Teruya and Ballard, 2004]. Over the last 10 years endovenous thermal ablation of the incompetent vein by laser energy has gradually become the treatment of choice [Min and Khilnani, 2005]. This laser energy leads to intimal damage, which results in permanent occlusion with subsequent fibrosis of the vein [Bergen et al. 2002]. Tumescent solution delivery is one of the most important steps in endovenous laser ablation (EVLA) [Altin et al. 2013]. It is required for the patient’s safety and the effectiveness of the procedure. Usually, a laser fiber is advanced from knee level up to 2 cm before the saphenofemoral junction (SFJ) and tumescent anesthesia is delivered along the perivenous space homogeneously.
Recent studies have described the different tumescent delivery systems in EVLA [Altin et al. 2013]. Most of the reports have claimed the superiority of tumescent anesthesia when compared with general or spinal anesthesia [Altin et al. 2013; Memetoglu et al. 2010]. Other reports have mentioned that the patient can feel pain and discomfort during the EVLA procedure if the tumescent anesthesia is inadequate [Altin et al. 2013; Memetoglu et al. 2010]. Therefore, different techniques and combination options for tumescent anesthesia have been studied many times [Altin et al. 2013; Memetoglu et al. 2010]. However, according to our knowledge, the literature does not include sufficient information regarding the difference in tumescent delivery direction between distal to proximal (knee to SFJ) or proximal to distal (SFJ to knee) delivery techniques.
In our experience, tumescent solution can be delivered in two ways, either distal to proximal (knee to SFJ) or proximal to distal (SFJ to knee). In this study, we compared these ways of delivery in terms of differences in tumescent volume, number of punctures, and pain and comfort scores of the patients. The aim of this study was to determine which way of delivery increases the comfort of both surgeon and patient during the procedure.
Patients and methods
Between August 2013 and October 2013, a prospective and nonrandomized study was performed including EVLA in a total of 100 patients. Patients were divided into two equal groups (n = 50 for each group). All patients had a unilateral treatment.
In all patients, the potential risks and benefits of EVLA were explained, and informed written consent was obtained. In addition, throughout the study, the principles of the Helsinki Declaration were strictly followed and the study was approved by the hospital’s ethical committee. Clinical, etiological, anatomical, pathological (CEAP) classification and venous clinical severity score were used for the documentation of the varicosities and symptoms. In the outpatients clinic duplex ultrasonography (DUS) was performed by a radiologist using a GE LOGIQ 7 (GE Healthcare, Milwaukee, WI, USA) with a high-resolution 5–13 MHz linear probe while the patient was standing to quantify the great saphenous vein (GSV) reflux.
Patients having GSV reflux over 1 s were included in the study. Exclusion criteria included one of the following: a nonpalpable pedal pulse, deep vein thrombosis (DVT), inability to ambulate, generally poor health, pregnancy, nursing, hypercoagulability, and extremely tortuous veins.
The 100 patients were divided equally into two groups. In group 1, tumescent solution was delivered in a proximal to distal direction. In group 2, tumescent solution was delivered in a distal to proximal direction. All patients were treated with a radial laser fiber (Limit Medical, Ankara, Turkey) and 1470 nm diode laser (Diotech, Busan, South Korea). We recorded GSV diameter, delivered total energy, treated GSV length, delivered tumescent volume, number of punctures, and pain and comfort scores during the procedure for each patient. The pain scores were recorded on a scale between 0 (no pain) and 10 (worst pain imaginable), and the patient was asked to give a number for his/her pain during tumescent delivery. In the same way, comfort scores between 0 (no comfort) and 10 (most comfortable) were also recorded.
Technique
All the operations were performed by two vascular surgeons for uniformity of application. One of the surgeons performed the DUS and the other carried out the procedure. All patients were treated under local anesthesia. The patient was positioned in a supine, anti-Trendelenburg position with the leg slightly abducted. The leg was disinfected with betadine and covered with sterile clothes. We performed the DUS examination using a MicroMaxx® (Sonosite, Inc, Bothell, WA, USA) with a high-resolution HFL 38/13–6 ultrasound transducer (Sonosite, Inc). The transducer of the DUS machine was disinfected with betadine and the nonsterile parts of the tranducer were placed under a sterile camera cover. Under ultrasound control, the best point for the puncture was selected and the GSV diameter was measured at the selected point. The vein was punctured using the Seldinger technique with a 19-gauge needle (Argon Medical Devices, Plano, TX, USA) and a 0.035 inch J- tipped 45 cm guide wire was introduced into the vein. A stab incision with a blade 11 knife was made at the entry point of the guide wire then a 6F introducer sheath (Argon Medical Devices) was inserted over it. A laser fiber was then inserted into the sheath, advanced up to the SFJ and the tip of the laser fiber was placed approximately 2 cm distal to the superficial epigastric vein (Figures 1(a) and 2(a)). Then patient was placed in a Trendelenburg position for tumescent delivery and laser ablation. Tumescent solution was delivered through a 20 ml syringe manually into the perivenous space under ultrasound guidance using a 19G needle (Figures 1(b) and 2(b)). The solution included 500 ml saline, 100 mg 0.5% bupivacaine, 10 ml 8.4% sodium bicarbonate, and 1 ml adrenaline. After we had ensured that the tumescent solution was delivered uniformly around the vessel, we started firing the laser. We used an intermitant mode (5 s duration, 1 s pause) and delivered 10–15 watt power in accordance with the vein diameter during ablation. Closure of the GSV was confirmed by ultrasound after ablation of the vein.

Ultrasound images of the perivenous space (PVS) at the saphenofemoral junction level before (a) and after (b) delivery of 40 ml tumescent solution.
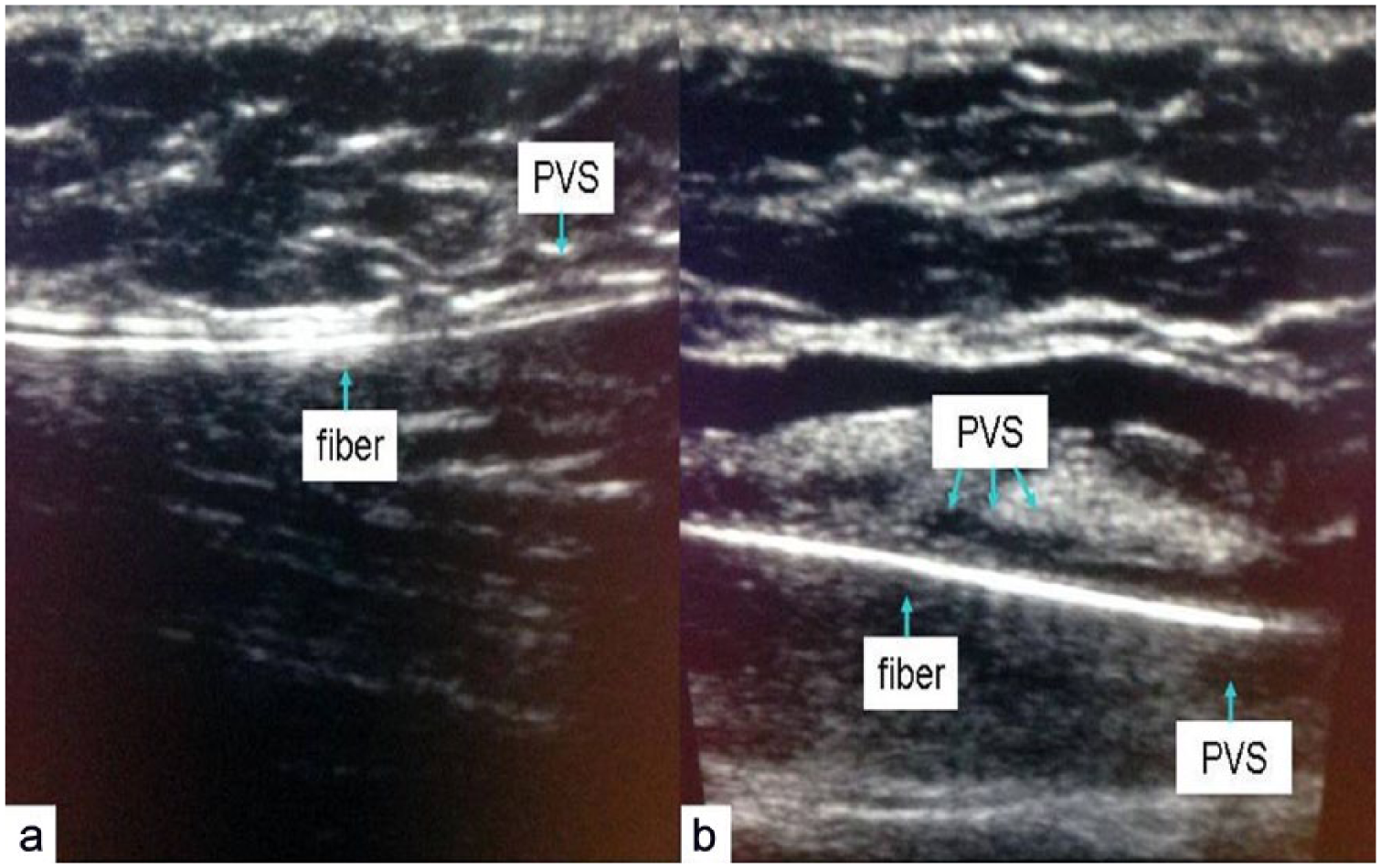
Ultrasound images of the perivenous space (PVS) at knee level before (a) and after (b) delivery of 40 ml tumescent solution.
Patients with varicosities underwent concomitant miniphelebectomies (MPs). Compression pads were applied over the course of the treated vein with an elastic bandage on it for the first 24 h after the operation. Then patients wore full-thigh compression stockings (20–30 mmHg) for a month. Patients were given a nonsteroidal anti-inflammatory drug for a week. They were also advised to walk for at least 1 h/day, but to avoid intense exercise, high temperatures, and standing for a long period of time.
Follow-up examinations
Patients were evaluated using DUS at the first week and first month after the operation. Noncompressibility of the treated veins with no blood flow within the ablated GSV was used to define successful treatment. The presence of recanalization in the previously ablated vein, bruising, thrombophlebitis, cellulitis, paresthesia, skin burns, and DVT were recorded as complications.
Statistical analysis
Number Cruncher Statistical System (NCSS) 2007 Statistical Software (Kaysville, UT, USA) was used for statistical analysis in this study. In the process evaluating the data, as well as descriptive statistical methods (i.e. mean, standard deviation, median and interquartile ranges), independent Student’s t-test for comparing normally distributed variables in binary groups and the Mann–Whitney U test for comparing not normally distributed variables in binary groups were used. Pearson’s chi-squared test was used to compare qualitative data. Significance were evaluated at p < 0.05 level.
Results
EVLA was successfully performed in all patients. Preoperative patient demographic details are shown in Table 1. There was no statistically significant difference between the groups. Concomitant MPs were performed in all patients after completing the laser ablation. Pain and comfort scores during tumescent delivery were evaluated. Operational data are summarized in Table 2.
Preoperative patients’ demographics.
Operative data.

There is no difference statistically between group 1 and group 2 according to GSV diameter, delivered total energy, and treated GSV length. Moreover, the average of the delivered tumescent volume in group 2 is lower than in group 1 (p = 0.0001). In addition, we needed fewer punctures in group 2 than we did in group 1 (p = 0.0001). There are significant differences statistically between the two groups in regard to the pain and comfort scores. Furthermore, the average pain score in group 2 is lower than in group 1 (p = 0.0001). Also, the patients in group 2 said that they had had a more comfortable operation than the patients in group 1 (average comfort score was higher in group 2, p = 0.0001; p < 0.05).
After the EVLA, no major complications such as DVT and skin burns occurred. There were some minor complications including bruising over the course of the ablated vein (16%), paresthesia (6%), cellulitis (4%), and thrombophlebitis (3%). There were no statistically significant differences between groups. None of the patients had recanalization in the ablated vein at the 1 week and 1 month follow ups by DUS.
Discussion
According to our results proximal tumescent delivery provided lower tumescent volume than distal application. In addition, fewer punctures were detected in the proximal tumescent delivery method, and also, better comfort and pain scores were obtained with proximal tumescent delivery. There was no difference between the proximal and distal tumescent delivery routes with regard to complications. This is a unique study that compares the proximal and distal tumescent delivery routes in EVLA.
EVLA was introduced as an alternative to conventional surgery by Navarro and colleagues in 2001 [Navarro et al. 2001], and has rapidly become the treatment of choice for treating saphenous vein insufficiency. Tumescent anesthesia delivery is an important stage in EVLA. It provides local anesthesia to make the procedure painless for the patient [Yilmaz et al. 2007]. In addition, it provides isolation of the GSV from surrounding tissues [Yilmaz et al. 2007]. Therefore, it prevents heat damage to the skin and accompanying nerves and decreases the risk of complications, such as skin burn and paresthesia [Min and Khilnani, 2003]. Tumescent anesthesia compresses the vein by bringing the vein wall into close contact with the laser fiber. This makes the ablation more efficient and improves the long-term outcome of EVLA [Min and Khilnani, 2003, 2005; Proebstle et al. 2006; Timperman et al. 2004]. The tumescent solution should be delivered homogeneously into the perivenous space in order to obtain the benefits.
We found that inserting the needle for the first time into the perivenous space at the distal point is difficult because the space between the vein wall and the fascia is tight (Figures 1(a) and 2(a)). However, once we had entered the space it became easier to deliver the tumescent solution homogeneously (Figures 1(b) and 2(b)) with fewer punctures. Performing fewer punctures made the patients more comfortable during tumescent delivery. These patients (in group 2) also felt less pain during the procedure. Another advantage of delivering the tumescent solution in a distal to proximal direction is that it needs a smaller tumescent volume for the same efficacy. On the contrary, filling the perivenous space in a proximal to distal direction requires more punctures and greater tumescent volume. As there are shorter intervals between punctures along the vein, patients feel more pain and less comfortable during tumescent delivery in a proximal to distal direction.
Endovenous ablation procedures are performed easily under local anesthesia by experienced surgeons [Durai et al. 2010]. When we considered the whole procedure, we observed that patients felt pain mostly during tumescent delivery because of the needle puncturing and the burning effect of the local anesthetic agent. In our opinion, other parts of the procedure, especially during laser firing, seem relatively painless if the tumescent solution is delivered uniformly around the perivenous space. We believe that if the patient is comfortable during the tumescent delivery stage, the whole procedure is comfortable. Therefore, it also affects the comfort of the surgeon.
In conclusion, delivering the tumescent solution in a distal to proximal direction might be the most effective way to increase the comfort of both the patient and surgeon during EVLA of the GSV.
Footnotes
Conflict of interest statement
All the named authors have seen and approved the submitted manuscript, affirming their contribution and responsibility for the work without any conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.