
Abstract
Background:
Small, observational trials have suggested a reduction in adjacent gastric activity with ingestion of soda water in myocardial perfusion imaging (MPI). We report our findings prior to and after implementation of soda water in 467 consecutive MPI studies.
Methods:
Consecutive MPI studies performed at a high-volume facility referred for vasodilator (VD) or exercise treadmill testing (ETT) were retrospectively reviewed before and after implementation of the soda water protocol. Patients undergoing the soda water protocol received 100 ml of soda water administered 30 min prior to image acquisition and after stress. Studies were performed using a same day rest/stress protocol. Incidence of adjacent gastric activity, diaphragmatic attenuation, stress and rest perfusion defects, and major adverse cardiovascular events (MACE) outcomes defined as death, myocardial infarction, stroke, reevaluation for chest pain, and late revascularization (>90 days from MPI) were abstracted using International Classification of Diseases, Ninth Revision (ICD-9) search.
Results:
Two hundred and eighteen studies were performed prior to implementation of the soda water protocol and 249 studies were performed with the use of soda water. Baseline demographic data were equal between the groups with the exception of more patients undergoing VD stress receiving soda water (p < 0.001). Soda water was not associated with a decreased incidence of adjacent gastric activity with stress (54.7% versus 61.9% with no soda water, p = 0.129) or rest (68.6% versus 69.5% with no soda water, p = 0.919) imaging. Less adjacent gastric activity was observed with patients undergoing ETT who received soda water (42.5% versus 56.9% with no soda water, p = 0.031), but no difference was observed between the groups with VD stress (69.0% versus 68.1% with no soda water, p = 1.000).
Conclusion:
The use of soda water prior to technetium-99m MPI was associated with lower rates of adjacent gastric activity only in patients undergoing ETT stress but not rest or VD stress. This differs from previously published data.
Keywords
Background
Myocardial perfusion imaging (MPI) is one of the most powerful diagnostic and prognostic tests in the evaluation of ischemic heart disease. Technetium (Tc-99m) is a commonly used radiotracer secondary to emission of a higher energy photon (140 keV) which provides for higher resolution images and minimal scatter when compared with thallium [Wackers et al. 1989]. However, the clearance of Tc-99m primarily by the liver with eventual excretion into the biliary system can result is significant gastric and intestinal uptake, creating significant imaging artifact adjacent to the myocardium [Higley et al. 1993]. One small trial has suggested a reduction in adjacent intestinal activity with ingestion of soda water in MPI [Hara et al. 2008]. We sought to examine the incidence of gastric activity in our institution prior to and after implementation of soda water in 467 consecutive MPI studies.
Methods
Consecutive MPI studies performed at a high-volume, tertiary care facility referred for vasodilator (VD) (adenosine or regadenoson) or exercise stress testing were retrospectively reviewed before and after implementation of the soda water protocol. Studies were performed using a same day rest/stress protocol (Figure 1). All patients underwent overnight fasting prior to testing. Only the patients receiving soda water prior to imaging received oral intake prior to acquisition. Resting images were obtained following a 10–12 mCi dose of Tc-99m sestamibi. Patients were redosed with 29–32 mCi dose of Tc-99m sestamibi administered at peak stress. Patients undergoing the soda water protocol received 100 ml of soda water (Perrier, Nestlé Waters, MT, France) immediately before image acquisition (both stress and rest) and 30–60 min following Tc-99m dosing. This timing of soda water administration was chosen to evaluate whether this technique would be effective and thus potentially improve throughput. After resting images were obtained, patients underwent either an exercise treadmill test (ETT) stress or VD stress infusion with administration of either a standard adenosine 140 μg/kg/min 6 min infusion or regadenoson 0.4 mg intravenous injection.

Graphical depiction of study cohort. Patients were injected with technetium 99m (Tc-99m) 30–60 min prior to imaging (stress and rest). Soda water was given immediately prior to stress and rest imaging.
Stress testing, image acquisition, and image processing were performed in the cardiology department under the direct supervision of a cardiologist and a nuclear technician. A Siemens C-Cam dual source gamma camera (Siemens Medical Solutions USA, Inc., Hoffman Estates, IL, USA) with a low-energy, high-resolution (LEHR) collimator and iterative reconstruction was used for image acquisition. Images were acquired in a 180° rotation with the patient in a semirecumbent position using the following parameters: starting position −45; step angle 2.8°/32 directions per detector head; matrix size 128 × 128; collection time for rest images 25 s/step; collection time for stress images 35 s/step. Image processing was performed using Siemens 3D flash software (Siemens Medical Solutions USA, Inc.) and iterative reconstruction. Image interpretation was performed in a separate location by a single nuclear medicine imaging specialist at the time of initial image acquisition who was blinded to the implementation of this protocol. Perfusion defects were graded qualitatively, with mild perfusion defects defined as 50–75% radiotracer uptake, moderate perfusion defects as 25–49% radiotracer uptake, severe perfusion defects as 1–24% radiotracer uptake, and complete defects had no radiotracer uptake. Perfusion defects during rest and stress were analyzed separately using a pooled count of each defect severity within polar map groupings corresponding to inferior (segments 3, 4, 5, 9, 10, 11, and 15), anterior (segments 1, 2, 6, 7, 8, 12, and 13), lateral (segments 5, 6, 11, 12, and 16), and septal (segments 2, 3, 8, and 9) distributions. Stress-induced ischemia was defined as incremental improvement in a given perfusion defect from stress compared with rest within the given segment. Fixed perfusion defects were defined as persistence of the same degree of perfusion defect severity between stress and rest images. Reverse defects were defined as incremental improvement in a given perfusion defect from rest when compared with stress, thus likely representing the artifact. Gastric activity was present when activity within the gastric wall was indistinguishable from the myocardium [Figure 2(a, b)] on raw image review. The raw images were available for review in cine and still frame projections at any point along the 180° camera arc. Differentiation of gastric activity from the adjacent bowel or hepatic activity was at the discretion of the nuclear cardiologist during initial interpretation. No patients in this analysis were imaged using prone positioning.

Raw data tomograms of rest images demonstrating gastric wall activity (dashed circle) with (a) significant adjacent gastric activity and (b) no significant adjacent gastric activity.
Patient background data were abstracted using the Department of Defense (DOD) outpatient and inpatient electronic medical record (EMR) system. MACE outcomes defined as death, stroke or transient ischemic attack, myocardial infarction (MI), evaluation for chest pain following MPI, or late revascularization more than 90 days after MPI testing were abstracted with manual EMR abstraction. Chest pain evaluations were identified initially by searching ICD-9 codes for atypical chest pain (786.59), chest pain (786.5), and angina (413) in the inpatient and outpatient setting from the date of initial evaluation. All visits pertaining to the index MPI were excluded. ICD-9 codes for death (798.1, 798.2, 798.9, and V12.53), stroke (434.00, 434.01, 434.10, 434.11, 434.90, 434.91, 997.02, and V12.54), nonfatal MI (410.0–410.9), and late revascularization (defined as revascularization > 90 days from index MPI) with percutaneous intervention (PCI) (92980, 92981, 92982, 92995, and 92996) or coronary artery bypass grafting (33510-33514, 33516, and 33533-33536) were used for initial data extraction followed by DOD outpatient and inpatient EMR verification of events. We determined mortality using the social security death index followed by reverification using EMRs for the last visit date as well as Tricare healthcare informatics division verification. All events identified by ICD-9 code were adjudicated. Patient follow up was performed using EMRs with 100% patient capture in this cohort.
Statistical analysis was performed using IBM SPSS version 19.0 (IBM, Armonk, NY, USA). Categorical variables are presented as frequencies with percentages and contingency tests were employed to compare differences between groups. Continuous variables were reported as mean ± standard deviation or median with range as appropriate. Differences between continuous variable groups were analyzed using analysis of variance. MACE-free survival was analyzed using a Kaplan–Meier method with log-rank test. For these variables, two-tailed p values less than 0.05 were considered statistically significant. Bivariate logistic regression analysis was performed to assess parameters that may predict the presence of adjacent gastric activity with p value less than 0.05 considered statistically significant. Differences between the groups receiving soda water compared with no soda water in rest and stress images were analyzed using contingency testing (z test) with application of a Bonferroni correction with p value less than 0.0125 considered statistically significant.
Results
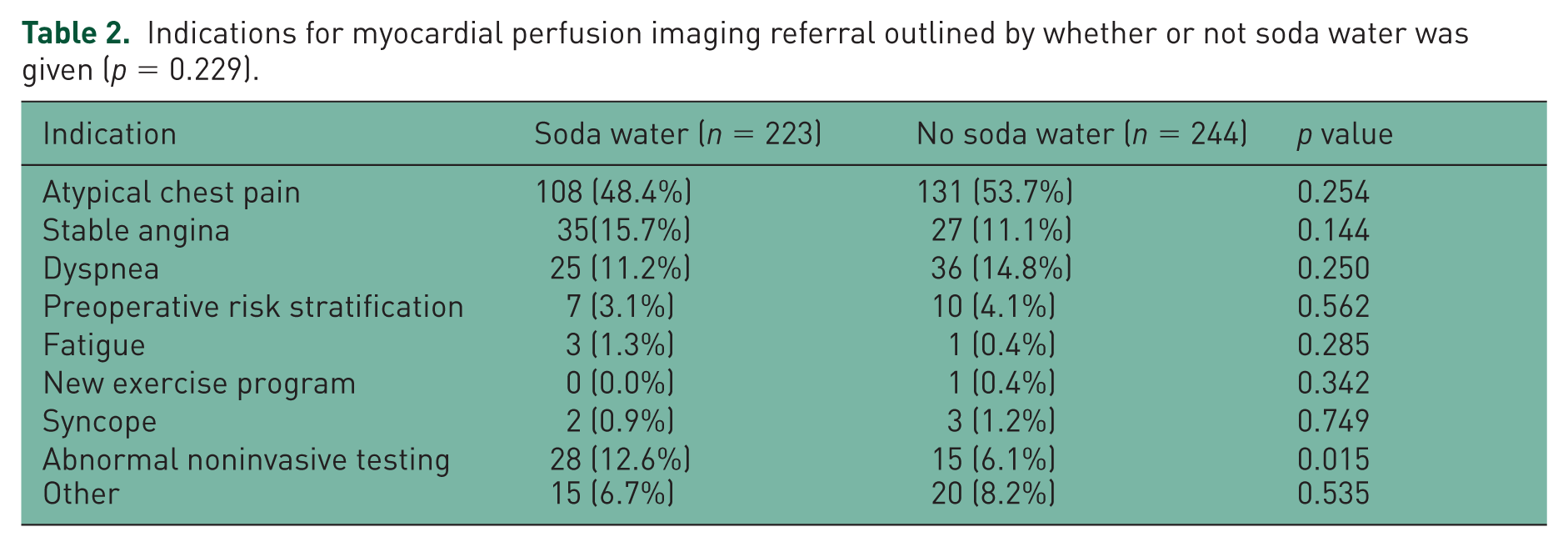
Four hundred and sixty-seven consecutive patients underwent MPI between July 2013 and February 2014. Patient demographics are outlined in Table 1. The groups are equally balanced with the exception of patients undergoing a VD stress protocol who were more likely to receive soda water (45.7% versus 35.2%, p < 0.001). In addition, there was a difference in the duration of patient follow up between the groups, with patients receiving soda water having shorter median follow up [median 111 days (IQR25–75 66–161, range 0–365 days) for the soda water group versus median 190 days (IQR25–75 124–240, range 0–365) for the no soda water group, p < 0.001]. Indications for performance of MPI in this cohort are outlined in Table 2, separated by whether or not soda water was given. There are no significant differences between the two groups with regard to the indication for testing (p = 0.229).
Patient characteristics and baseline demographics.

CABG, coronary artery bypass grafting; CAD, coronary artery disease; LBBB, left bundle branch block; CCB, calcium channel blocker; ETT, exercise treadmill test; MET, metabolic equivalent.
Indications for myocardial perfusion imaging referral outlined by whether or not soda water was given (p = 0.229).
Qualitative adjacent gastric activity during all stress was not significantly different between the group that received soda water (54.7%) compared with the no soda water group (61.9%, p = 0.129). There was significantly less adjacent gastric activity following ETT (42.5% versus 56.9%, p = 0.031), but not VD stress (69.0% versus 68.1%, p = 1.000) in patients receiving soda water compared with no soda water, respectively. VD stress testing was more common in the patients receiving soda water (45.7% versus 35.2%, p < 0.001). In addition, regadenoson stress was more common in the cohort receiving soda water (45.7% versus 17.6%, p < 0.001) whereas adenosine stress infusion was more common in the patients who did not receive soda water (17.6% versus 0%, p < 0.001). Neither the stress modality used nor administration of soda water was found predictive of the presence of adjacent gastric activity on logistic regression analysis. Table 3 summarizes the changes in attenuation and outcomes between the groups. There was no significant difference between the groups during stress imaging with respect to the presence of qualitative diaphragmatic attenuation, stress-induced ischemia, fixed defects, or reverse defects. Qualitative adjacent gastric activity during rest was also not different between the group receiving soda water and the group with no soda water (68.6% versus 69.5%, p = 0.919). Table 4 summarizes the incidence of image attenuation and perfusion defects by pooled distribution during rest imaging. There was no significant difference between the groups with respect to diaphragmatic attenuation (p = 0.547). Administration of soda water and patient demographic parameters were not found to predict the presence or absence of adjacent gastric activity during rest imaging with logistic regression analysis.
Stress myocardial perfusion imaging attenuation, artifacts, and perfusion defects.

Bonferroni correction was applied to the evaluation of the perfusion defect severity subgroups making the required p value for statistical significance = 0.0125.
VD, vasodilator; GXT, graded exercise test.
Rest myocardial perfusion imaging attenuation, artifacts, and perfusion defects.

Bonferroni correction was applied to the evaluation of the perfusion defect severity subgroups making the required p value for statistical significance = 0.0125.
Analysis of pooled perfusion defects during stress [Figure 3(a)] showed a significant overall decrease in inferior (p = 0.012), lateral (p = 0.021), and anterior (p = 0.018) defects with the administration of soda water. Analysis of individual degrees of perfusion defect severity within each pooled wall segment demonstrated no significant difference between the group receiving soda water compared with no soda water after application of Bonferroni correction for subgroup analysis. In contrast, administration of soda water during rest imaging [Figure 3(b)] was associated with significant worsening of inferior (p < 0.001), lateral (p < 0.001), anterior (p < 0.001), and septal (p < 0.001) pooled perfusion defects compared with no soda. Subgroup analysis demonstrated significantly more mild and moderate perfusion defects with administration of soda water in the inferior, lateral, and anterior wall segments at rest and mild perfusion defects in the septal wall segment compared with no soda water after Bonferroni correction.

Analysis of pooled inferior segment (segments 3, 4, 5, 9, 10, 11, and 15), lateral segment (segments 5, 6, 11, 12, and 16), anterior segment (segments 1, 2, 6, 7, 8, 12, and 13), and septal segment (segments 2, 3, 8, and 9) perfusion defects at stress (a) and rest (b).
Discussion
Various methods have been reported for the reduction in adjacent gastric radiotracer activity. The excretion of Tc-99m into the gut is thought to be 29–34% at rest and 25–37% with stress with the primary site for entry into the bowel lumen within the small intestine [Wackers et al. 1989; Higley et al. 1993]. Tc-99m-tetrofosmin gastrointestinal (GI) tract activity increases exponentially at rest (2.9 ± 2.3% injected activity at 5 min increasing to 10.7 ± 2.7% injected activity at 60 min) and in a more linear fashion with stress (2.0 ± 1.9% injected activity at 5 min increasing to 5.7 ± 3.6% injected activity at 60 min). This GI tract activity is significantly greater than that observed in the myocardium during the same time period post injection (1.2 ± 0.3% injected activity at 5 min increasing to 1.2 ± 0.4% injected activity at 60 min) at rest and with stress (1.3 ± 0.3% injected activity at 5 min increasing to 1.1±0.2% injected activity at 60 min) [Higley et al. 1993].
In the setting of cardiac single photon emission computed tomography (SPECT) imaging, higher activity in the GI tract reduces target to noise ratio needed (particularly the inferior wall) for quality nuclear imaging. Imaging artifacts can occur secondary to count normalization creating a perfusion defect or count scatter resulting in the perception of increased perfusion. Increasing gastric volume or distention is thought to improve myocardial SPECT imaging by increasing the distance between the inferior myocardial wall and the adjacent GI tract. Two small trials, to date, have examined the effect of soda water in Tc-99m sestamibi perfusion imaging. In these analyses, improving gastric motility with metoclopramide was ineffective at reducing adjacent gastric activity [Weinmann and Moretti, 1999]. In contrast, carbonated lime drink improved the myocardium to adjacent abdomen ratio with both planar and SPECT imaging in a predominantly male population of 33 consecutive patients [Malhotra et al. 2010].
Various techniques have been studied using Tc-99m imaging with tetrofosmin. Erythromycin was found to be inferior to lime water ingestion at reducing interfering extracardiac activity [Vorster et al. 2010]. Several oral agents have been used in an attempt to create gastric distention and increase the ratio of myocardial counts to adjacent GI counts. Boz and colleagues used 200 ml of milk followed by a standard sandwich and 220 ml of water prior to resting images and 200 ml of milk before stress images compared with 200 ml of milk only before stress and rest to reduce adjacent gastric activity. The patients in the sandwich group had less adjacent GI activity with improvement in the myocardium to abdominal count ratio [Boz et al. 2001]. Oral contrast mixed into 1 liter of water has been shown to reduce adjacent GI activity when compared with 1 liter of water alone and a control group in a total of 30 patients (p < 0.001). Two patients in the contrast arm did not tolerate drinking 1 liter of fluid over 30 min prior to imaging [Iqbal et al. 2004].
The use of soda water in Tc-99m MPI has been looked at previously in small patient populations. Hara and colleagues assigned a total of 95 patients in a prospective fashion to either a control group (n = 32) or a soda water group (n = 63) prior to stress imaging following adenosine VD stress. Patients were imaged 5 min following Tc-99m injection and quantitative assessment of the inferior myocardium as well as adjacent GI activity were obtained in three planar projections to arrive at an average inferior wall to abdomen (I/A) count ratio. This group was able to show a reduction in adjacent GI activity from 90.6% to 69.8% in the group receiving soda water (p = 0.038). The I/A count ratio was significantly higher in the soda water cohort (1.9 ± 0.51) compared with the control group (1.5 ± 0.35, p < 0.0001). In addition, three-dimensional computed tomography was performed in both groups and volumetric analysis of gastric distention was performed demonstrating a substantial increase in gastric volume from 55.9 to 276.6 ml with soda water administration [Hara et al. 2008].
We present the largest patient population to date examining the use of soda water prior to both stress and resting Tc-99m SPECT imaging. In contrast to previously published data, administration of soda water was only associated with a reduction in adjacent gastric activity following ETT stress imaging. In our experience, there was significantly less inferior, lateral and anterior perfusion defects with the use of soda water during stress, which was offset by significantly more inferior, lateral, anterior, and septal perfusion defects with soda water administration during rest. Previous data would suggest soda water would be most advantageous during stress imaging with VD or rest imaging. Our conclusions are complicated by the differences between the groups with respect to the VD stress agent used in that significantly more patients in the soda water cohort received regadenoson as the stressor agent whereas significantly more adenosine was used in the patients not receiving soda water. As adenosine is a nonselective G-protein-coupled receptor agonist, there is likely more effect on gastric motility than would be seen with the more selective A2A receptor agonist regadenoson. In addition, the effect of soda water use on perceived perfusion defects should be minimal and isolated to the inferior, and in rare cases, anterior walls. Given the small cohort of patients in the published literature to date, perhaps soda water administration has additional effects beyond simple gastric expansion and perhaps the optimal formulation of soda water to achieve myocardial count separation from gastric uptake has yet to be elucidated. Finally, semirecumbent patient positioning, while likely beneficial in reducing diaphragmatic artifact, may have increased the prevalence of subdiaphragmatic artifact sources such as adjacent gastric activity. Larger prospective, trials are needed to better delineate the presence and magnitude of soda water effect on Tc-99m SPECT imaging attenuation and artifacts.
Limitations
We recognize several limitations to our study. This study is single center and retrospective. While our findings represent a real-world experience following incorporation of a soda water protocol, the results are hypothesis generating and require prospective confirmation. Due to the observational nature of our analysis, patient follow up for downstream clinical events outside of our healthcare system may not have been captured. While we performed exhaustive chart review from a worldwide resource of all military electronic health care records, there remains the potential for incomplete data. Qualitative image interpretation was performed and thus subject to higher rates of inter- and intra-observer variability than semiquantitative analysis. Finally, images were obtained on a single SPECT platform and thus these results may not be generalizable to other camera configurations.
Conclusion
The use of soda water prior to Tc-99m MPI was associated with a modest reduction in adjacent gastric activity during ETT stress without significant effect during rest or VD stress imaging. While soda water significantly decreased perfusion defects in stress wall segments, this benefit was offset by a significant increase in resting wall perfusion defects.
Footnotes
Acknowledgements
The opinions in this manuscript do not constitute endorsement by San Antonio Army Medical Center, the US Army Medical Department, the US Army Office of the Surgeon General, the Department of the Army, Department of Defense, or the US Government of the information contained therein.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The authors declare that there is no conflict of interest.