
Abstract
Background:
Nephrosclerosis progresses slowly to end-stage renal disease (ESRD) in only a small percentage of patients. However, because hypertension and nephrosclerosis are normally found simultaneously, nephrosclerosis is a risk factor for cardiovascular disease (CVD). In turn, the onset of CVD may progress to further renal impairment.
Aim:
To evaluate clinical outcomes and the association between nephrosclerosis and CVD in the long term.
Design:
Prospective study
Methods:
We prospectively assessed 35 patients (male/female: 19/16) with nephrosclerosis aged >30 years at disease onset, attending the Kidney Disease Center, Saitama Medical University, in a single teaching hospital center between 1995 and 2014. Nephrosclerosis was diagnosed in accordance with the criteria outlined in the World Health Organization (WHO) monograph of renal diseases. All patients were followed by means of registries for 10 years to record subsequent events, if any.
Outcomes:
The primary study outcome was correlating the occurrence of CVD, defined as a composite of cardiovascular deaths, nonfatal and fatal myocardial infarction, and stroke, with the development of ESRD or death.
Results:
The mean age of patients at the time of biopsy was 54.8 ± 12.7 years (range 33–72 years). Of these patients, seven were affected by nonfatal CVD and two died due to CVD. Only one patient developed ESRD during the follow-up period. Using Kaplan–Meier analysis, risk factors for the primary study outcome were estimated to include an estimated glomerular filtration rate (eGFR) < 60 ml/min/1.73 m2, systolic blood pressure > 130 mmHg and proteinuria > 1 g/g creatinine. Univariate analysis was used for the assessment of the relative risk for the primary study endpoint of several covariates: age, systolic blood pressure, eGFR and proteinuria at time of renal biopsy. eGFR was found to be the strongest factor determining an event-free period [relative risk (RR) =1.931, p = 0.014].
Conclusions:
Patients with nephrosclerosis are at high risk of CVD when they have moderately advanced renal impairment.
Introduction
Nephrosclerosis progresses to end-stage renal disease (ESRD) in only a small percentage of patients and is known to closely associate with cardiovascular disease (CVD). The relationship between mild to moderate hypertension and either nephrosclerosis or ESRD remains circumstantial, although these syndromes have long been linked according to the medical literature [Ronco, 2010; Ronco and Di Lullo, 2014].
Both an epidemiological study on Atherosclerosis Risk in Communities (ARIC) (Bash et al. 2009; Hui et al. 2013] and a large scale clinical study on Heart Outcomes and Prevention Evaluation (HOPE) [Mann et al. 2001] clearly demonstrated that mild renal insufficiency was the largest risk factor for total mortality and CVD. In both studies, the causes of mild renal insufficiency were uncertain because renal biopsy data were unavailable. It was suspected that renal impairment of studied patients was related to hypertension and aging. As previously known, renal disease associated with hypertension and aging is classified as hypertension or benign nephrosclerosis [Hill, 2008; Meyrier, 2014].
A diagnosis of nephrosclerosis is arbitrarily assigned to people who have a long-term history of hypertension and present with mild renal insufficiency and/or mild proteinuria. A renal biopsy is a necessary requirement to confirm such a diagnosis. However, in clinical practice, a renal biopsy is rarely performed and a diagnosis of nephrosclerosis is made by exclusion of other diseases on clinical grounds [Freedman et al. 1995]. When hypertensive patients are suspected to have nephrosclerosis, evidence of other chronic kidney diseases, such as glomerulonephritis, renovascular disease and interstitial nephritis, should be excluded by renal biopsy [Fogo et al. 1997; Wehrmann and Bohle 1998]. Indeed, in 136 patients diagnosed as having ‘benign nephrosclerosis’, Zucchelli and Zuccala performed a thorough diagnostic workup, including kidney biopsies, and found cholesterol emboli in 29.4%, renovascular disease in 26.5% and true nephrosclerosis in only 44.1% of patients [Zucchelli and Zuccala, 1993]. Recently, in Norway 102 biopsy-proven nephrosclerosis cases were followed for the long term, from which it was concluded that nephrosclerosis was a common condition in ESRD and CVD [Vikse et al. 2003].
In Japan, as far as we know, reports discussing the prognosis of Japanese patients with nephrosclerosis in the long term are lacking. Moreover, recent advances in genetics provide convincing evidence that there are a variety of factors, including environmental factors, aging, obesity, chronic inflammation and essential hypertension, which contribute to nephrosclerosis in different populations. In the present study, we prospectively followed 35 biopsy-proven nephrosclerosis patients and describe their characteristics and prognosis during the years 1995–2014 at a single center in Japan.
Subjects and methods
Patients
This was a prospective, observational, single-center cohort study conducted in accordance with the Declaration of Helsinki. Approval for the study was obtained from Saitama Medical University Hospital Ethics Committee and written informed consent was obtained from each participant at the time of renal biopsy.
Patients were selected from patient histories containing both clinical and histopathological data at the time of renal biopsy.
In general, indications for renal biopsy in our institute include proteinuria > 1.0 g/24 hours, or a serum creatinine < 1.5 mg/dl if a renal parenchymal cause is suspected. We studied patients biopsied from April 1995 to December 2003 and followed for 10 years. During this period, the registry received a total of 1024 biopsies, including those from 35 patients diagnosed with nephrosclerosis. All cases were reviewed by two experienced nephron pathologists from the Department of Pathology at Saitama Medical University Hospital, who used the diagnostic criteria described below. Consequently, consistent diagnostic criteria were used in all cases. The patients were treated and followed at the Kidney Disease Center of Saitama Medical University Hospital, Saitama, Japan.
In the present analysis, the primary study outcome was a composite endpoint of: ESRD, defined as chronic renal failure necessitating chronic dialysis treatment or renal transplantation; fatal and nonfatal CVD, where myocardial infarction (MI) is defined by clinical symptoms combined with the new appearance of Q waves and elevation of the ST segment on at least two electrocardiograms obtained on separate occasions and/or elevation of creatinine phosphokinase MB (CKMB) of more than 250 U/l and troponin of more than 0.25 ng/ml; and stroke, defined by clinical symptoms combined with evidence from computed tomography (CT) and/or perfusion magnetic resonance imaging (MRI) data.
Histopathological diagnosis
Standard methods of processing and staining of biopsy tissues were used. All specimens were examined by light microscopy and immunohistochemistry – staining for immunoglobulin (Ig) G, IgA, IgM, C3 and C1q). When considered necessary, electron microscopy was applied to exclude other types of renal disease. Nephrosclerosis was diagnosed in accordance with the criteria given in the World Health Organization (WHO) monograph of renal disease [Churg and Sobin, 1982]. Light microscopy observation of hyaline arteriolosclerosis, especially of the afferent arteriole, is characteristic of nephrosclerosis: The arteriolar wall is thickened by homogeneous eosinophilic material that narrows the lumen. Arteries may show medial hypertrophy, subsequent intimal sclerosis and reduplication of elastic laminae. There is a variable degree of glomerular capillary collapse and glomerular sclerosis associated with focal tubular atrophy with interstitial fibrosis. Areas with clusters of sclerotic glomeruli and tubulointerstitial scarring become more extensive with the progression of disease. Cases complicated by other kidney diseases, such as glomerulonephritis, malignant hypertension and interstitial nephritis, were excluded from the study.
Clinical and laboratory investigations
The study baseline was defined as the time of biopsy, when standard clinical and laboratory tests were performed. In this paper, we focused on the following baseline variables: age, sex, serum creatinine, urinary protein, blood pressure, serum albumin, uric acid and total cholesterol.
According to the CKD Guidelines of the Japanese Society of Nephrology, estimated glomerular filtration rate (eGFR) was calculated by the following Modification of Diet in Renal Disease (MDRD) equation for the Japanese: eGFR = 194 × Cr(-1.094) × Age(-0.287) (× 0.739, if female) [Matsuo et al. 2009].
Exclusion criteria
Exclusion criteria included diabetes mellitus, atrial fibrillation, known left ventricular dysfunction (ejection fraction <55%), signs and symptoms of congestive heart failure, pregnancy or lactation, significant valvular or coronary heart disease, cardiac arrhythmia or conduction defects, systemic diseases, and use of sedative, hypnotic drugs or any other drugs potentially affecting blood pressure during ambulatory monitoring (e.g. corticosteroids).
Follow-up methods
During the study, target home blood pressure was 130/80 mmHg or lower, and home blood pressure measurements were encouraged [Suzuki et al. 2002]. The selection of an antihypertensive agent depended on the physicians’ preference but would have included renin–angiotensin inhibitors [Suzuki, 2004]. All patients were followed up every month until the primary study endpoint. At each clinic visit, serum creatinine, electrolyte concentrations, complete blood counts and other serum chemistries (uric acid, glucose, albumin, cholesterol and liver enzymes) were measured. Lipid lowering drugs, primarily statin derivatives, were administered if serum cholesterol levels exceeded 240 mg/dl [Suzuki et al. 2013].
Statistical analysis
Statistical analyses were performed using JMP software, version 9 (SAS, Cary, NC, USA). Data are presented as mean
Patient event-free curves were calculated by the Kaplan–Meier life table analysis method and differences between the groups were evaluated by the log-rank test.
The Cox proportional hazard regression model was used to evaluate the effects of the individual baseline variables on the primary study outcomes. The following variables were entered into the Cox model: continuous values of age, proteinuria, serum albumin, systolic and pulse blood pressure, and eGFR.
Results
Baseline characteristics
Baseline characteristics of the 35 subjects with nephrosclerosis are listed in Table 1. Of the 35 patients, 19 (54%) were male and 16 (46%) female. The mean age of patients at the time of biopsy was 54.8 ± 12.7 years (range 33–72 years).
Patient characteristics.

Values are mean ± SEM.
LV, left ventricular; SEM, standard error of the mean.
Blood pressure
A total of 13 patients (37.4%) who were diagnosed as having nephrosclerosis received antihypertensive treatment at the time of biopsy. After the start of the study, all patients were treated with antihypertensive agents, including renin–angiotensin system inhibitors. The risk of development of the primary study outcome was similar, whether patients received blood pressure treatment or not, at the time of renal biopsy.
Reasons for a renal biopsy
A total of 18 patients received antihypertensive therapy and 10 patients were diagnosed as having hypertension, if the blood pressure level cutoff for hypertension was set at 130 mmHg/80 mmHg. All patients not receiving antihypertensive therapy had hypertension as well as renal disease. All patients had urinary abnormalities (proteinuria and/or hematuria) at renal biopsy; 14 (40%) had moderate or severe proteinuria (> 1 g/24 hours). Microscopic hematuria was reported in 17 (48%). Renal function was impaired (eGFR < 60 ml/min/1.73 m2) in 15 (42%) of patients.
Outcomes
Of the 35 patients with nephrosclerosis, 7 patients were affected by nonfatal CVD (4 patients had cerebrovascular disease and 3 patients had a MI) and 2 patients died due to CVD (1 patient had cerebrovascular disease and 1 patient had a MI). Only one patient progressed to ESRD during the follow-up period.
Comparison between patients with and without events
Of the variables, age and serum creatinine levels were significantly higher and, conversely, eGFR was significantly lower, in patients with events compared with those without events (Table 2; all p < 0.05). As shown in Table 2, there were no significant differences between the two groups in regards to proteinuria, systolic and diastolic blood pressures, and pulse pressure.
Comparison of patients’ characteristics without or with events.
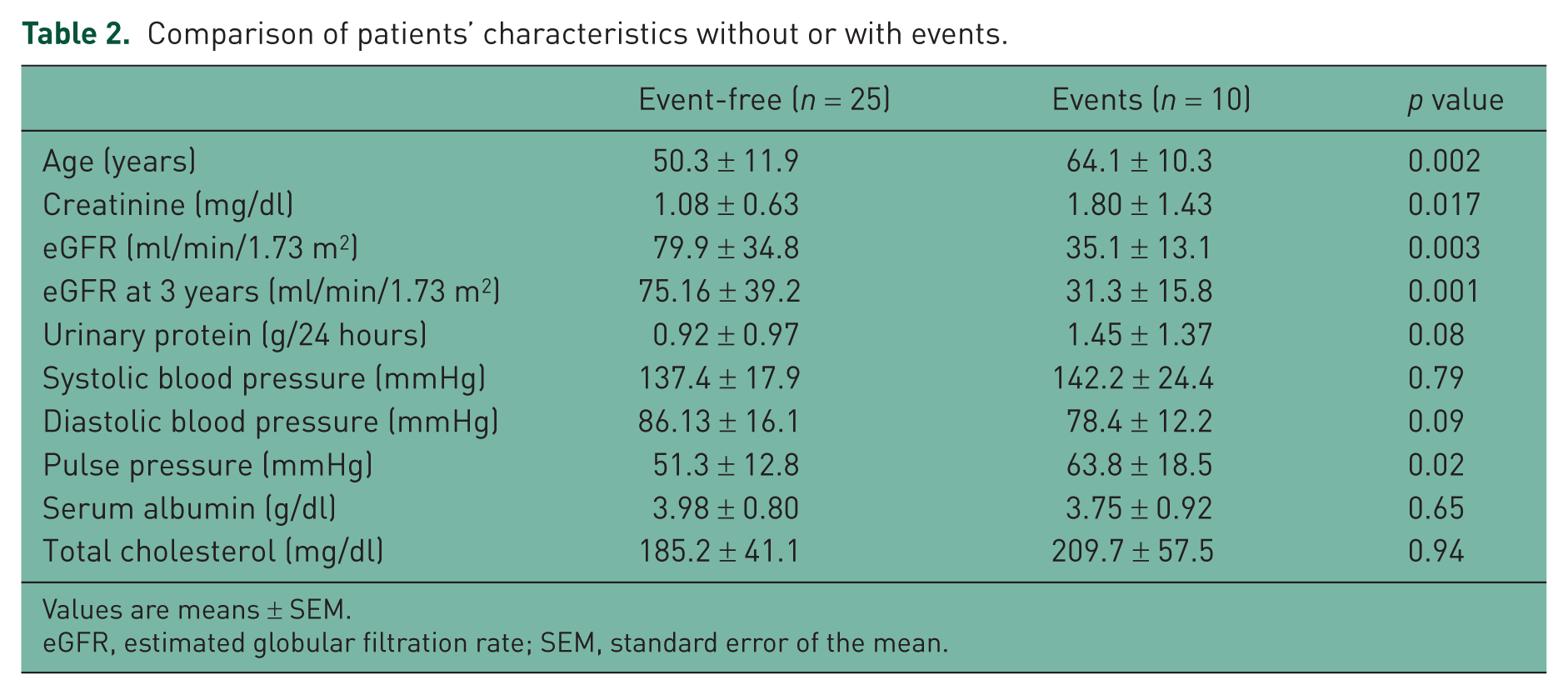
Values are means ± SEM.
eGFR, estimated globular filtration rate; SEM, standard error of the mean.
Risk factors for the primary study outcome
The cumulative probabilities of the primary study outcome are given in Figures 1 to 4. Patients with higher levels of systolic blood pressure and pulse pressure, increased urinary excretion of protein and decreased eGFR had a significantly higher risk of progression to the primary study outcome during the entire follow-up period.
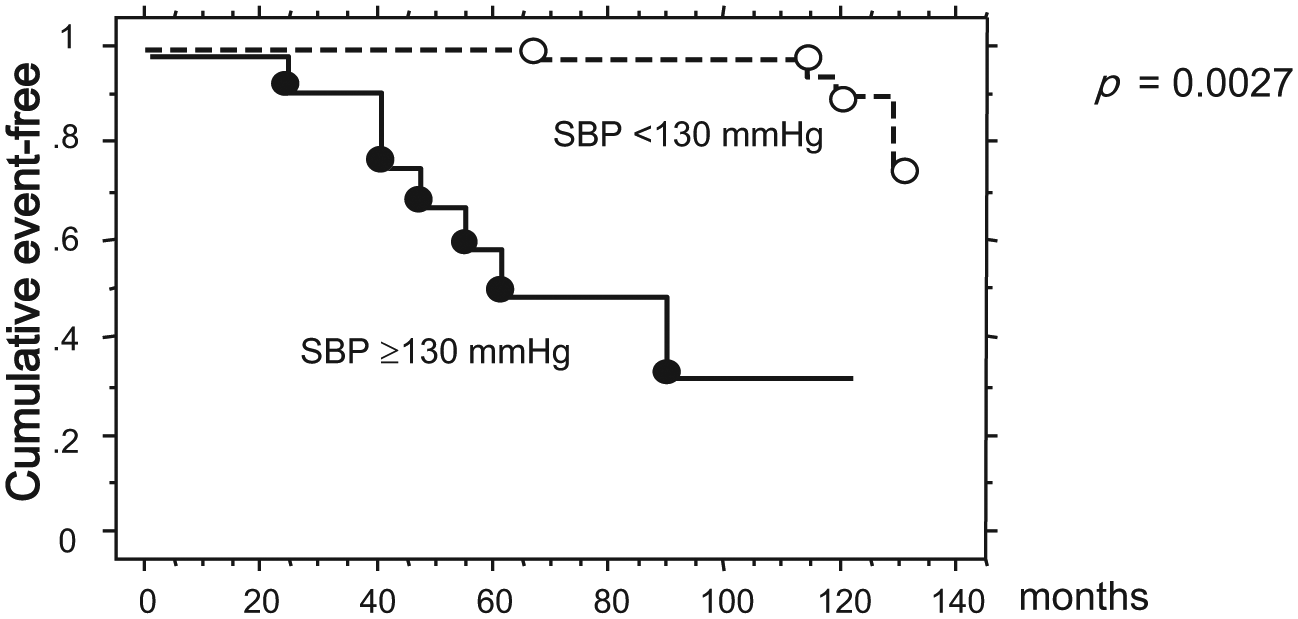
Kaplan–Meier analysis showing the cumulative, event-free probability for all patients with nephrosclerosis according to SBP.

Kaplan–Meier analysis showing the cumulative, event-free probability in patients with nephrosclerosis according to PP.

Kaplan–Meier analysis showing the cumulative, event-free probability for all patients with nephrosclerosis according to proteinuria.

Kaplan–Meier analysis showing the cumulative event-free probability for all patients with nephrosclerosis according to eGRF.
Systolic blood pressure
In patients with systolic blood pressure ⩾130 mmHg, regardless of antihypertensive therapy, just over 30% were event-free at 10 years versus 78% of patients with systolic blood pressure <130 mmHg (Figure 1; p = 0.0027).
Pulse pressure
In patients with pulse pressure >65 mmHg, just over 20% were event-free at 10 years versus 54% of patients with a pulse pressure <65 mmHg (Figure 2; p = 0.0128).
Proteinuria
In proteinuric patients (
eGFR
An eGFR < 60 ml/min/1.73 m2 was a strong prognostic marker for an event: 100% experienced an event by 10 years versus 20% of patients with an eGFR > 60 ml/min/1.73 m2 (Figure 4; p = 0.0041).
Changes in eGFR in patients without events
The eGFR in patients without events did not show changes during a 10 year follow-up period (Figure 5).

Changes in eGFR during 10 years in event-free patients.
Prediction of the primary study outcome by univariate analysis
We used univariate analysis to assess the relative risk (RR) for the primary study outcome of a composite end point including CVD, ESRD or death; and as covariates: age, eGFR and urinary excretion of protein at onset, hypertension at onset (Table 3). Moderate or severe proteinuria during follow up was the strongest predictor of composite endpoint (RR: 1.931, p = 0.014), followed by systolic blood pressure (RR: 1.651, p = 0.041) and urinary protein (RR: 1.532, p = 0.038). The small numbers of patients in this study precluded multivariate analysis.
Cox regression for event-free.
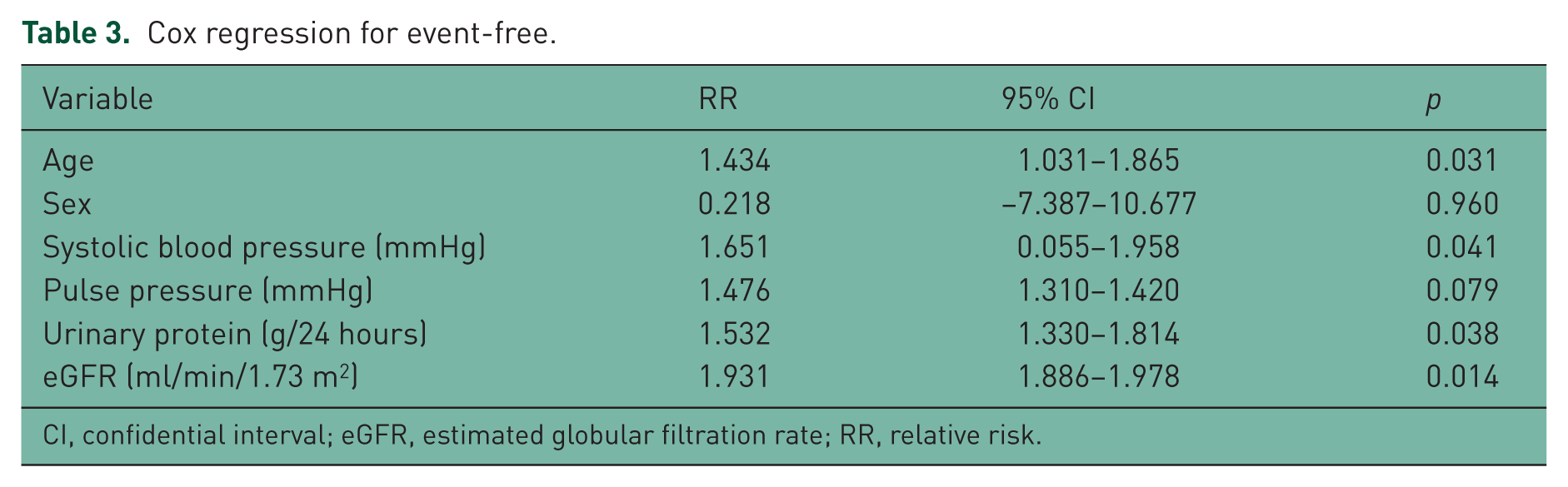
CI, confidential interval; eGFR, estimated globular filtration rate; RR, relative risk.
Discussion
This study describes the long-term follow up of patients with nephrosclerosis in a single kidney disease center in Japan. From the present study, the following conclusions were reached. Firstly, patients with nephrosclerosis who had a lower eGFR and higher systolic blood pressure and pulse pressure were likely to suffer a CVD event. Secondly, CVD events may not be preventable after nephrosclerosis is found, even though intensive antihypertensive therapy with renin–angiotensin inhibitors is performed. Thirdly, the early detections of low eGFR levels, high blood pressure and proteinuria are of the utmost importance, because of their possible contribution to CVD in nephrosclerosis patients before a diagnosis by renal biopsy.
It is well known that cardiovascular events occur more frequently in patients with CKD or vascular disease; they typically take place in the final stage of a pathophysiologic process of progressive vascular damage [Garcia-Donaire and Ruilope, 2010]. Renal disease and CVD share similar etiopathogenic risk factors, including hypertension, dyslipidemia, glucose metabolism disturbances, cigarette smoking, obesity and physical inactivity. This cardiorenal continuum illustrates the sequential occurrence of the atherosclerotic process from the initial stage, in which cardiovascular risk factors are detected. In the present study, an eGFR < 60 ml/min/1.73 m2 was a strong risk factor for progression to CVD events. It has previously been demonstrated that a reduction in renal function is an important risk factor for CVD [Mann et al. 2003]. The HOPE study reported that the impact of early renal insufficiency on CVD in primary and secondary outcomes was not affected by the presence of either diabetes or hypertension. However, the causes of mild renal insufficiency were not determined and it was uncertain what proportion of the studied population exhibited nephrosclerosis in the HOPE study. Since the selection criterion used was described as vascular disease, it is likely some proportion of participants were affected by nephrosclerosis. Combining these data with our present findings, a combination of hypertension and mild renal insufficiency is a strong predictor for a future CVD event.
Previously, serum creatinine was used for the evaluation of renal insufficiency. However, more recently, monitoring levels of serum creatinine has been replaced by measuring eGFR, which is a more accurate indicator of renal function. In line with this notion, our findings strongly support the use of eGFR in elderly hypertensive patients with impaired renal function. However, unresolved issues remain, since intensive blood pressure controls used in this study did not produce a favorable outcome. After a post hoc analysis of HOPE, the authors proposed that an individual with mild renal insufficiency be treated with angiotensin converting enzyme (ACE) inhibitors [Yusuf et al. 2000]. Additionally, it is recommended that renin–angiotensin system inhibitors be used in hypertensive patients with CKD to prevent progression to ESRD [Casas et al. 2005]. However, Onuigbo has proposed that renin–angiotensin system inhibitors are not always effective for the prevention of progression of renal dysfunction [Onuigbo, 2011]. Similar findings were reported by the African American Study of Kidney Disease and Hypertension (AASK), demonstrating that even with excellent blood pressure control and the use of a renin–angiotensin system inhibitor, the progression of underlying CKD is relentless [Appel et al. 2010]. In this regard, further investigations will be needed to prevent CVD events in hypertensive patients with nephrosclerosis.
Some 15 years ago, Wehrmann and colleagues demonstrated that in 170 patients diagnosed with decompensated benign nephrosclerosis, more than one third progressed to ESRD [Wehrmann et al. 1989]. This finding contrasts with the recent popular notion that nephrosclerosis slowly progresses to ESRD in only a small proportion of patients, indicating that such decompensated, benign nephrosclerosis differs from the nephrosclerosis cases we dealt with.
More recently, Vikse and colleagues reported that benign nephrosclerosis short-term predictors of ESRD differ from long-term predictors [Vikse et al. 2003]. Benign nephrosclerosis is associated with high mortality and morbidity, and the vascular changes seen are markers of generalized disease in these patients. In their study, Viske and colleagues found a larger proportion of patients progressed to ESRD, without CVD events; this appears to contrast with our present findings, where a large proportion of patients suffered from CVD before progression to ESRD. This difference may be explained by differences in renal function at the start of the study, with average values of serum creatinine being recorded by us at less than 1.3 mg/dl, compared with those of Viske and colleagues at 2.0 mg/dl, indicating that the latter’s patients more readily developed ESRD. Another possible reason for the observed difference in studies is found in a recent review [Meyrier, 2014], where the development of nephrosclerosis in patients, even proven by biopsy, has a heterogeneous etiology, including populations, obesity, duration of hypertension, or modality of antihypertensive therapy. As was the case in the AASK study, it is quite possible that many cases have underlying primary kidney disease due to genetic variation [Kopp, 2013].
Although during nephrology trials the doubling of serum creatinine and consequent renal death is a frequently used endpoint, in the present study we used instead a composite endpoint, consisting of CVD, progression to ESRD and death. A doubling of serum creatinine was mostly observed in patients with relatively higher entry serum creatinine levels of between 1.5 and 2.0 mg/dl [Bakris et al. 2010]. This indicates that the sensitivity of detection of absolute changes in GFR is higher as serum creatinine rises. Thus, the doubling of serum creatinine may be an appropriate endpoint in trials recruiting patients with higher serum creatinine levels (e.g. >1.5 mg/dl), but may be less useful in trials where the serum creatinine entry levels are lower; in this regard, in the present study, we did not use such an endpoint.
Study limitations
There are potential limitations to our study. Although prospective, it was observational and cross-sectional in design and therefore subject to potential residual confounding effects. Secondly, our study was limited by the small number of patients analyzed. Thirdly, this study was performed at a single renal center and thus, the application of findings to other populations, including other sites, is unknown; however, this may have consequently avoided the variability generally produced by using multiple centers. Finally, as the pathological diagnosis of nephrosclerosis does not mean hypertension induced nephropathy, a direct connection between nephrosclerosis and hypertension should be discussed cautiously. In the present study, the authors would like to emphasis that patients with biopsy-proven nephrosclerosis should be carefully followed up with a focus on blood pressure.
In spite of these various limitations, this study was carried out in a single center. Moreover, an overwhelming strength of the present paper is a well-characterized cohort of patients who participated in a rigorously performed and carefully followed-up study.
Conclusion
Patients with nephrosclerosis are at high risk of CVD when they have moderately advanced renal impairment. It seems reasonable to recommend close clinical follow ups of patients with high blood pressure, particularly if these patients also show one or more of the risk factors demonstrated in this study, such as decreased eGFR, increased systolic blood pressure and pulse pressure, increased urinary protein and old age.
Footnotes
Conflict of interest statement
The authors declare no conflicts of interest in preparing this article.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.