
Abstract
Objective:
The prognostic value of the Global Registry of Acute Coronary Events (GRACE) risk score (GRS) and the Thrombolysis in Myocardial Infarction (TIMI) risk index (TRI) have been reported in patients with coronary artery disease (CAD). In this study, we sought to evaluate the association between TRI and the extent and severity of CAD evaluated by SYNTAX score (SS) and Gensini score in patients with ST elevation myocardial infarction (STEMI).
Methods:
A total of 290 patients with STEMI were included in the study. GRS and TRI were calculated on admission using specified variables. The extent and severity of CAD were evaluated using the SS and Gensini scores. The patients were divided into low (TRI ⩽19), intermediate (TRI 19–30), and high (TRI ⩾30) risk groups. A Pearson correlation analysis was used for the relationship between TRI, GRS, Gensini score and SS.
Results:
There were significant differences in the mean age (p < 0.001), admission heart rate (p < 0.001), admission systolic blood pressure (p = 0.009), SS (p < 0.001), GRS (p < 0.001) and in-hospital major adverse cardiac events (MACE) in all patients between the low, intermediate and high TRI risk groups. There was a positive significant correlation between TRI and SS (r = 0.24, p < 0.001), Gensini score (r = 0.18, p = 0.002), GRS (r = 0.74, p = 0.001) and in-hospital MACE (r = 0.29, p < 0.001).
Conclusion:
TRI is significantly related to SS and Gensini score in predicting the extent and severity of CAD in patients with STEMI.
Introduction
Coronary artery disease (CAD) and acute myocardial infarction (MI) are a major cause of death and morbidity worldwide. Atherosclerosis is a major cause of cardiovascular disease (CVD) [Lopez et al. 2001]. Coronary atherosclerosis is the main cause of ST elevation acute myocardial infarction (STEMI). Recently, cardiologists have begun studying risk stratification in patients with acute coronary syndrome (ACS) to identify the severity and complexity of CAD. For this intention, a large number of scoring systems and laboratory parameters have been used in clinical practice. The SYNTAX score (SS) is one of these scoring systems, used to determine the extent and severity of CAD [Serruys et al. 2009; Wykrzykowska et al. 2010; Girasis et al. 2011; Acet et al. 2014a].
Although these scoring systems have many advantages, they require an invasive method such as coronary angiography to perform the scoring. Therefore, those interested in cardiovascular medicine still need an easily accessible, cost-effective and noninvasive method to carry out risk stratification to determine the extent and severity of CAD of ACS patients. In order to identify high-risk patients with ACS, various risk classification systems and scoring systems are used [Braunwald et al. 2002; GUSTO IV-ACS Investigators, 2001; Boersma et al. 2000; de Araújo Gonçalves et al. 2005; Granger et al. 2003]. Prediction of early and late mortality using the in-hospital death Global Registry of Acute Coronary Events (GRACE) risk score (GRS) and the Thrombolysis in Myocardial Infarction (TIMI) risk score (TRS) has been shown by testing in populations of hundreds of thousands of patients [de Araújo Gonçalves et al. 2005; Granger et al. 2003]. Recently, the TIMI risk index (TRI) has been proven to be useful in many studies due to its ability to predict mortality, and the ease of assessment and scoring with fewer parameters (age, blood pressure, heart rate, etc.) in patients with non ST-elevation ACS (NSTE-ACS) and patients with STEMI [Wiviott et al. 2004; Bradshaw et al. 2007].
But although many studies have investigated the relationship between GRS, TRI and Non-STEMI [Santos et al. 2013; Garcia et al. 2004], none have addressed the association between TRI and severity of CAD using SS and Gensini score in patients with STEMI. Thus, the aim of the current study is to investigate whether high TRI is associated with the extent and severity of CAD in patients with STEMI with SS and Gensini score.
Methods
Study population
This study was conducted retrospectively. A total of 590 patients that presented with STEMIs and underwent primary percutaneous coronary intervention (p-PCI) within 12 hours of symptom onset between January 2012 and October 2013 were included in the study. STEMI was defined based on criteria created by the American College of Cardiology and the European Society of Cardiology and included: an increase in troponin I > 1 ng/ml; a new ST elevation as measured from the J-point in two or more contiguous leads with leads V1, V2 and V3 measuring at least 0.2 mV or at least 0.1 mV in the remaining leads; and measurement during the first 12 hours after symptom onset or new developed left bundle branch block (LBBB) pattern [European Society of Cardiology and American College of Cardiology, 2000].
Patients with severe liver disease, autoimmune diseases, cancer, hematological disorders, severe valvular disease, inflammatory or infectious diseases, and a history of bleeding diathesis were excluded from the study. Patients on the following medications were also excluded from the study: corticosteroids, cytotoxic drugs, thrombolytic therapy, glycoprotein IIb/IIIa inhibitors and diuretics. Patients were also excluded if during the study the patient was not treated with primary PCI and did not follow up for blood work. After accounting for all of these exclusion criteria, a total of 290 patients remained in the study sample. All patients received a complete physical examination and assessment of coronary risk factors; medical histories and presenting clinical symptoms were also recorded. Patients were evaluated for heart failure prognosis according to Killip clinical examination guidelines [Killip and Kimball, 1967].
Demographic data and variables determined TRS points. A total score of 0–14 was possible according to the following characteristics: age, diabetes mellitus (DM)/hypertension (HT) or angina, heart rate < 100 beats per minute (bpm), systolic blood pressure (SBP) < 100 mmHg, Killip class II–IV, weight < 67 kg, anterior MI or LBBB presentation, and latency > 4 hours [David et al. 2000]. Calculation of the TRS was performed using a computer program. GRS points (including age, creatinine, heart rate, SBP, Killip class, cardiac arrest at admission, elevated cardiac markers and ST-segment deviation) were recorded [Granger et al. 2003] and calculation of the GRS was performed using a computer program. The TRI of patients was calculated using the formula: ‘Heart rate × (Age ÷ 10)2 ÷ SBP’.
Monitoring for major adverse cardiac events (MACEs) was performed during the in-hospital follow-up period. Examples of MACEs were cardiogenic shock, new advanced heart failure, pulmonary edema, complete atrioventricular block (AVB) requiring a temporary pacemaker, severe ventricular arrhythmia, and in-hospital mortality during the post-PCI follow-up period. An in-hospital mortality was only considered a MACE if the death was due to myocardial infarction, cardiac arrest or some other cardiac-related cause. Cardiogenic shock was defined as marked and persistent hypotension lasting more than 30 minutes with a systolic arterial pressure less than 80 mmHg with signs of hypoperfusion due to left ventricular dysfunction, right ventricular infarction or cardiac mechanical complications. New-onset advanced heart failure was diagnosed if the patient qualified for a New York Heart Association functional classification of III or greater. In order for a severe ventricular arrhythmia to be considered a MACE, it needed to occur within 48 hours of admission and the rhythm must have been ventricular fibrillation, ventricular tachycardia or asystole.
Blood works analysis
Venous blood samples were collected when the patient initially presented to the emergency department or intensive coronary care unit (ICCU) before p-PCI. Hematologic indices were measured using an automated hematology analyzer system (Abbott Cell-Dyn 3700; Abbott Laboratory, Abbott Park, IL, USA). Absolute cell counts were used to perform subsequent analyses. Total cholesterol, high-density lipoprotein (HDL), low-density lipoprotein (LDL), triglycerides, glucose and creatinine levels were measured using the Abbott Architect C 16000 autoanalyzer (Abbott Laboratory).
Angiographic analysis and syntax score
All patients underwent selective coronary angiography using the Judkins technique. Coronary lesions leading to ⩾50% diameter stenosis in vessels ⩾1.5 mm was scored separately and added together to provide the cumulative SS, which was prospectively calculated using the SS algorithm on the baseline diagnostic angiogram [Sianos et al. 2005]. The online latest updated version was used for the calculation of the SS (http://www.SYNTAXscore.com). Two experienced interventional cardiologists analyzed the SS; the opinion of a third analyst was obtained and the final judgment was made by consensus in cases of disagreement. The final score was calculated from the individual lesion scores by analysts who were blinded to procedural data and clinical outcome. The Gensini scoring system was used to determine the severity of CAD [Gensini et al. 1983].
Statistical analysis
All analyses were performed using SPSS for Windows version 18.0 (SPSS Inc. Chicago, Illinois, USA). Continuous variables were expressed as the mean ± 1 standard deviation (SD) and categorical variables were expressed as percentages. Comparisons between categorical variables between the TRI groups were performed using the χ2 or Fischer’s exact test. Analysis of variance (ANOVA) was used in the analysis of continuous variables. A stratified analysis of clinical and laboratory variables was performed according to the tertiles of the TRI. The correlation between TRI and score parameters was assessed by the Pearson correlation test. Statistical significance was defined as a p value < 0.05. The cutoff points for sensitivity and specificity of TRI in predicting SS was estimated by performing a receiver operator characteristic (ROC) curve analysis. The study protocol was reviewed and approved by the Ethics Committee in accordance with the Declaration of Helsinki.
Results
A total of 290 patients [216 male (74.5 %), mean age 61.5 ± 14.0 years] were enrolled in the study. The TRI tertiles are TRI low ⩽ 19 (n =96), TRI mid > 19 and < 30 (n =94), and TRI high ⩾ 30 (n =106). The baseline characteristics of the three groups are summarized in Table 1. The mean age of the TRI high group was higher than that of the TRI low and TRI mid groups (p < 0.001 for all). Frequency of hypertension, smoking, positive family history and Killip class III–IV were more common in the TRI high group. Admission heart rate and admission SBP were high in TRI high group patients (p < 0.001, p = 0.009, respectively, for all).
Demographic characteristics of patients in TIMI Risk Index groups.

ANOVA test and χ2 test;
Fischer Exact test
ACE, ANOVA, analysis of variance; bpm, beats per minute; CAD, coronary artery disease; SBP, systolic blood pressure; TIMI, Thrombolysis in myocardial infarction; TRI, TIMI Risk Index.
Initial laboratory findings of patient groups are compared in Table 2. The admission level of creatinine in the TRI high group was significantly higher than that in with TRI low and mid groups (p = 0.006 for all). The levels of hemoglobin (p < 0.001 for all), triglycerides (p = 0.001 for all) and red blood cell (RBC) (p < 0.001 for all) were significantly lower in the TRI high group compared with the TRI low and mid groups. Gensini score (p = 0.007 for all), SS (p < 0.001 for all), TRS (p < 0.001 for all) and GRS (p < .001 for all) were significantly higher in the high risk patients compared with the low risk patients (Table 2).
A comparison of initial laboratory values and risk scores of patients in TIMI Risk Index groups.

Values are mean ± SD or n (%), ANOVA test;
ANOVA, analysis of variance; HDL, high-density lipoprotein; LDL, low-density lipoprotein; RBC, red blood cell count; SD, standard deviation; TIMI, thrombolysis in myocardial infarction.
The in-hospital adverse outcomes are listed in Table 3. The in-hospital death rate was greater in the high TRI group than in the other groups (p = 0.005 for all). MACEs were more frequent in the high TRI group than in the other groups (p < 0.001 for all). Similarly, occurrences of in-hospital advanced pulmonary edema (p = 0.005 for all), in-hospital cardiogenic shock (p = 0.008 for all) and severe ventricular arrhythmia (p = 0.002 for all) were higher in the high TRI group than in the other patient groups.
A comparison of in-hospital major adverse cardiovascular events of patients in TIMI Risk Index groups.
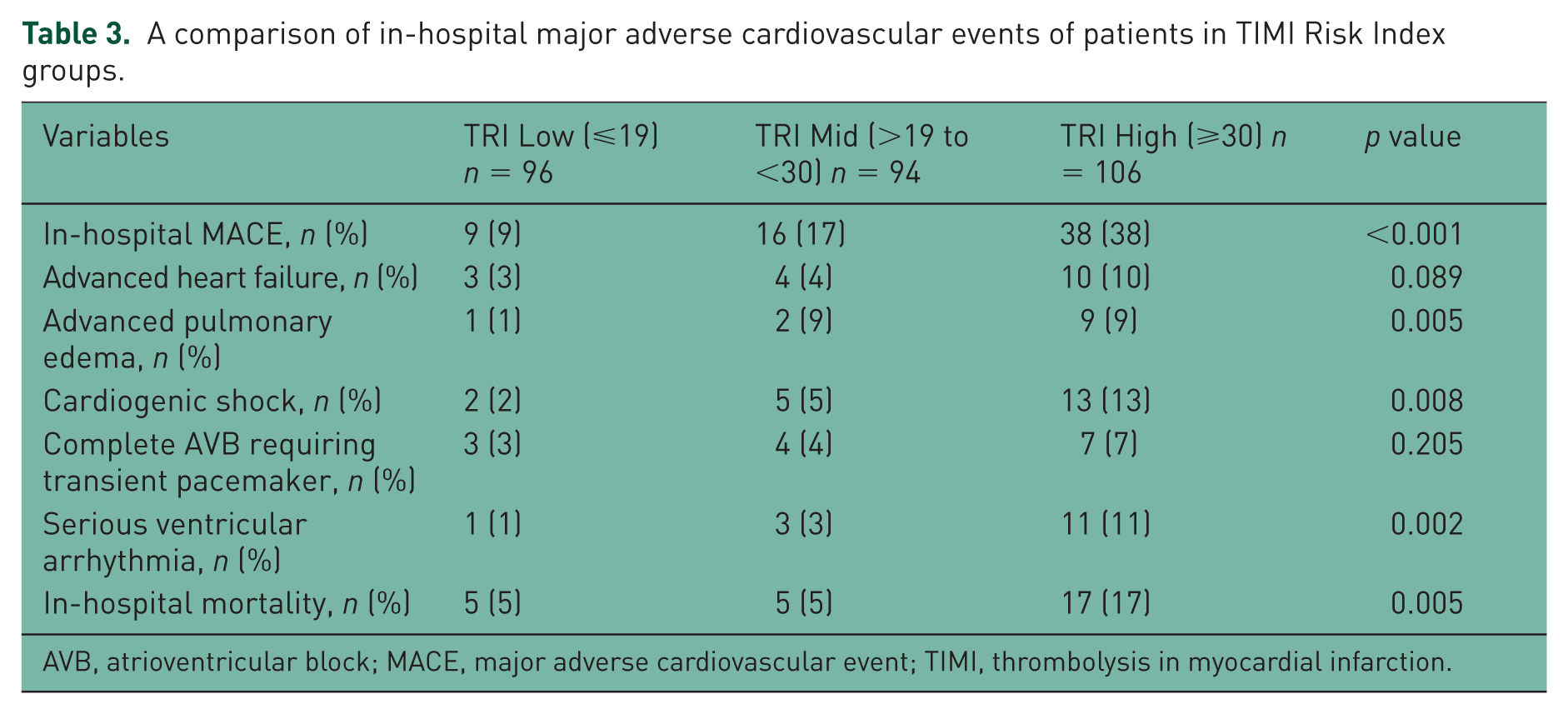
AVB, atrioventricular block; MACE, major adverse cardiovascular event; TIMI, thrombolysis in myocardial infarction.
Pearson’s correlation analysis revealed significant associations between a high TRI and Gensini score (r = 0.18, p = 0.002), SS (r = 0.24, p < 0.001) TRS (r = 0.65, p < 0.001), GRS (r = 0.74, p = 0.001), in-hospital MACE (r = 0.29, p < 0.001) and in-hospital mortality (r = 0.17, p = 0.004) (Table 4).
Pearson correlations of patients in TIMI Risk Index.

MACE, major adverse cardiovascular event; TIMI, thrombolysis in myocardial infarction.
The relationship between TRI and SS in patients with STEMI is demonstrated in Figure 1. In ROC analysis, a cutoff point of >14.25 TRI predicted SS (sensitivity 75.0%, specificity 42.0%, and an area under curve (AUC) of 0.625 [95% confidence interval (CI) 0.558–0.693; p < 0.001] (Figure 2).

Scatter dot presentation comparison of SYNTAX score and TIMI Risk Index.

Receiver operator characteristic curve analysis of high TIMI Risk Index in predicting SYNTAX score.
Discussion
We showed that TRI was significantly associated with GRS, SS and Gensini score, which are quantitative indicators of the extent and severity of CAD in patients with STEMI. Also, we showed that, on admission, Killip class, creatinine, triglycerides, RBC, hemoglobin, in-hospital mortality and in-hospital MACE were significantly associated with TRI in STEMI patients. Moreover, TRI was significantly correlated with GRS, TRS, Gensini score, SS, in-hospital mortality and in-hospital MACEs. A TRI of > 14 was the cutoff point for predicting higher SS, with a sensitivity of 75% and a specificity of 42%.
SS and Gensini score are scoring systems used to determine the extent and severity of CAD. Although these scoring systems are advantageous, the disadvantage is the requirement of an invasive method such as coronary angiography for the scoring CAD [Serruys et al. 2009; Wykrzykowska et al. 2010; Girasis et al. 2011; Acet et al. 2014a; Gensini et al. 1983; Neeland et al. 2012]. Thus, there is a need for an easily accessible, cost-effective and noninvasive method of risk stratification to determine the extent and severity of CAD in patients with ACS.
The GRS has been recognized as a validated predictor of adverse CAD events in CVD patients [Tang et al. 2007; Acet et al. 2014b]. The GRS includes variables such as hemodynamic status, Killip class and cardiac markers, but does not include the properties of coronary lesion including complexity and morphology, and is not used to determine the extent and severity of CAD.
One of the important scoring systems used in risk stratification in patients with ACS is TRS, because it has been shown to be useful and helpful in many studies with large patient populations. TRS for STEMI was calculated as the sum of independent predictors of mortality and ischemic events [David et al. 2000] and derived from STEMI patients in the Intravenous NPA for the Treatment of Infarcting Myocardium Early (InTIME-II) randomized controlled trial [InTIME-II Investigators, 2000]. The TRS for STEMI serves as a prognostic calculator that discriminates high-risk patients with the combination of baseline variables that are part of the routine medical evaluation [David et al. 2000]. TIMI scoring has been shown to be predictor of MACEs in patients with STEMI [Acet et al .2014c] and is frequently used in clinical practice.
In addition, the relationship between TRS and the severity of CAD has been shown in several studies. For example, when comparing TIMI score with the results of coronary angiography in 683 patients with NSTE-ACS, three-vessel disease or left main coronary disease have been shown to be more frequent in each increased risk category [Santos et al. 2013]. In the PRISM-PLUS study, in 1491 patients with ACS, it was shown that there were more severe coronary lesions and left main coronary lesions in patients with high TRS compared with those with low TRS [Mega et al. 2005]. These results were confirmed with the retrospective study of Salem et al. [Ben Salem et al. 2011].
As a result of these studies conducted with the GRS and TRS, SBP, heart rate and age were found to be the three most important parameters predicting mortality. Thus, Morrow and colleagues demonstrated that TRI, an index consisting of these three parameters, can be used in risk assessment of patients with ACS [Morrow et al. 2001]. In another study Truong and colleagues demonstrated that TRI predicts long-term mortality and heart failure in patients with STEMI [Truong et al. 2009]. It has also been demonstrated that TRI predicts short and long-term mortality in patients with ACS [Ilkhanoff et al. 2005; Bradshaw et al. 2007].
TRI, calculated using the formula, heart rate × (age/10)2/SBP, was derived from observed risk relations among 13,253 patients enrolled in the InTIME-II randomized trial of lanoteplase versus alteplase as reperfusion therapy for STEMI [InTIME-II Investigators, 2000]. The prognostic discriminatory capacity of this index was expressed [Hanley and McNeil, 1982]. TRI was a strong and independent predictor of mortality at 24 hours. It was validated in an external data set of STEMI patients from the TIMI-9 trials that showed both a high discriminatory capacity and concordance between the observed 30-day mortality and the predictions based on the InTIME-II data [Morrow et al. 2001]. Rathore and colleagues focused on this point after evaluating the discrimination and calibration performance of the TRI in a community-based cohort of elderly patients taken from the Cooperative Cardiovascular Project and found the index performed poorly [Rathore et al. 2003]. The TIMI investigators would appear to have responded successfully to this criticism. They demonstrated that this apparent absence of discriminatory power of the TRI, when applied to the less homogeneous general population and a select population of the elderly as well, is resolved when TRI is used as a continuous variable.
Just as the simple but useful risk assessment tool, the Killip classification, was instrumental in persuading the establishment to undertake an expensive departure from the time-honored convention of open-ward hospital care, so too should TRI be used to extend evidence-based care from the hospital coronary care unit to the field. Our study demonstrated that on admission, Killip class was significantly related to TRI with STEMI patients. We applied the TRI for STEMI in a group of patients who underwent p-PCI and showed that an increase in TRI is associated with increased frequency of in-hospital death. TRI was developed to predict mortality.
An important clinical implication of this study is that it identified a group of high-risk patients who not only have a mortality rate higher than the low-risk group, but also have an increased frequency of in-hospital adverse events such as heart failure, development of cardiogenic shock, ventricular arrhythmias and advanced pulmonary edema. However, angiographic findings are not TRI parameters; scoring systems that predict prognosis and the prevalence and severity of CAD, such as SS, have therefore started to be used in the clinic to determine risk stratification. SS is a comprehensive anatomic scoring system based on the coronary angiogram [Sianos et al. 2005]. SS quantifies the properties of lesion including complexity, morphology and location in the coronary tree and predicts outcome after PCI in patients with CAD who are undergoing revascularization [Serruys et al. 2009; Wykrzykowska et al. 2010] Also, SS reflects the pattern of atheroma and the technical difficulty of PCI [Wykrzykowska et al. 2010] It is able to aid revascularization decisions, and predicts mortality and morbidity in patients with CAD [Serruys et al. 2009; Wykrzykowska et al. 2010].
To our knowledge, the relationship between the TRI and SS for STEMI has not previously been investigated. Our results demonstrate for the first time the predictive value of TRI and SS in patients with STEMI. We found that high TRI was significant and correlated with increased SS. Our study is important because it is the first study in the literature in which TRI and its relationship with SS were evaluated in the same patient population. In this study, with the help of calculated TRI of patients admitted to the emergency department with ACS, information about in-hospital mortality of patients and severity and extent of CAD may be obtained.
Study limitations
Our study has some limitations. First, this was a retrospective study based on a relatively small number of patients and the study population was from a single center. Second, the method of measurement of SBP, which is one of the TRI parameters, presented a limitation. Because measured arterial blood pressure is not invasive, evaluation of interobserver variability is important for accurate and clear results. But this evaluation could not be completed in our study because our study was retrospective. Third, because there was a male dominance in patients in our study, the results may not be applicable in groups with female dominance.
Conclusion
TRI is significantly related to SS and Gensini score in predicting the extent and severity of the CAD in patients with STEMI. Moreover TRI significantly related to in-hospital MACEs and in-hospital mortality. TRI uses simple and inexpensive methods for evaluating patients with STEMI. In addition, high TRI may be helpful in identifying high-risk patients and determining appropriate treatment strategies. TRI can be readily calculated at point of care, thereby facilitating short- and long-term risk prediction for STEMI patients, even prior to revascularization.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The authors declare no conflicts of interest in preparing this article.