
Abstract
Objective:
Bicuspid aortic valve (BAV) is associated with aortic abnormalities. The ascending aorta tends to dilate and its elasticity deteriorates. The morphology of the BAV and the elasticity of the proximal ascending aorta seem to influence the outcome. This study aimed to determine the distensibility of the ascending aorta with normal diameter in BAV patients and its relation to its morphology.
Methods:
This is a cross-sectional study. In the patients with BAV referred for echocardiography, the phenotype was defined as anteroposterior (AP) or mediolateral (ML) leaflet orientations. The aortic distensibility at 5–10 mm above the sinotubular junction was assessed using transthoracic echocardiography in 50 BAV patients, and 50 healthy controls with tricuspid aortic valve (TAV) matched by gender and age.
Results:
The ascending aorta in BAV patients had less distensibility compared with that in the control subjects (0.00298 ± 0.0023 versus 0.00805 ± 0.0028 cm2 dynes−1 × 10−6, respectively, p < 0.001). The ML phenotype of BAVs was more frequent. However, the reduced distensibility was not related to gender and morphology of the valve.
Conclusions:
Regardless of the valve morphology and also in the absence of aortic dilation, aortic distensibility is impaired in BAV subjects compared with TAV subjects. This finding supports the idea of an intrinsic aortic wall anomalies underlying the impaired elasticity of the aorta in BAV patients.
Introduction
Bicuspid aortic valve (BAV) is the most common congenital heart anomaly with a male predominance affecting 0.5–2% of the population [Cedars and Braverman, 2012]. It is associated with aortic root or ascending aortic dilation with increased risk of dissection or rupture [Tadros et al. 2009]. Studies have shown reduced elastic properties of the proximal aorta in BAV patients [Biner et al. 2009]. Abnormal aortic elasticity has been shown to be a risk factor for aortic dilatation in patients with Marfan syndrome [Schaefer et al. 2007].
BAV includes different morphological phenotypes. Mediolateral (ML) and anteroposterior (AP) leaflet orientations are the most frequent BAV morphology [Schaefer et al. 2007]. Leaflet orientation may be a predictive factor in BAV disease progression and aortic dilatation [Fernandes et al. 2007]. Schaefer and colleagues demonstrated differences in aortic elasticity among different BAV phenotypes so that AP leaflet orientation had a higher stiffness index and lower distensibility in the aorta [Nemes et al. 2011]. However, all studies have not found this association [Jackson et al. 2011; Demir, 2013].
On the one hand, it has been stated that aortic dilation is predictive of worse outcomes [Holmes et al. 2007; Mordi and Tzemos, 2012]. So, serial evaluation of the aortic diameter, due to increased circumferential stress with increased aortic diameter, was supported [Okamoto et al. 2003]. On the other hand, some studies suggest that impaired elasticity is independent from aortic size and may be related to intrinsic aortic wall anomalies [Oulego-Erroz et al. 2013; Santarpia et al. 2012]. Due to contradictory results, this study was conducted to determine whether aortic distensibility is reduced in BAV patients with normal aortic size and whether this is related to valve leaflet orientation, gender and age.
Methods
A total of 50 asymptomatic BAV patients and 50 healthy control subjects with normal tricuspid aortic valve (TAV) matched by age and sex were recruited. The study was approved by Shiraz University ethics committee and informed consent was obtained from the participants.
BAV was diagnosed when two valve cusps were clearly identified at systole and diastole with a clear fish-mouth appearance in systole [Oulego-Erroz et al. 2013]. BAV phenotype was defined as AP and ML orientations.
To calculate aortic distensibility, a previously described formula was used [Stefanadis et al. 1990]:

Systolic and diastolic aortic internal diameters were measured on m-mode imaging of ascending aorta in parasternal long axis view at 5–10 mm above sinotubular junction and averaged from five consecutive beats by using a GE VIVID 7 echocardiography machine (Figure 1). Blood pressure was measured and averaged 5 min before echocardiography or simultaneously during an echocardiographic investigation by an experienced nurse blind about the study purpose.

Measurement of systolic and diastolic aortic diameters shown on the M-Mode image.
Exclusion criteria
Exclusion criteria were arterial hypertension (>140/90 mmHg), greater than mild aortic stenosis (peak velocity >3 m/s, mean gradient >20 mmHg), Marfan syndrome and aortic diameter more than 4 cm.
Statistical analysis
All analyses were performed using the statistical software program SPSS, version 16.0 (SPSS Inc., Chicago, IL). Continuous data were presented as mean ± standard deviation (SD). Categorical data were presented as an absolute number or percentages. Chi-squared and one-way analysis of variance (ANOVA) tests were used to compare categorical and quantitative data, respectively. The significance level was set at p < 0.05.
Results
The patients’ age range was 16–56 years (median = 30). As shown in Table 1, there were no significant differences in baseline characteristics as well as systolic blood pressure and diastolic blood pressure between the study groups.
The baseline characteristics of BAV and control subjects.
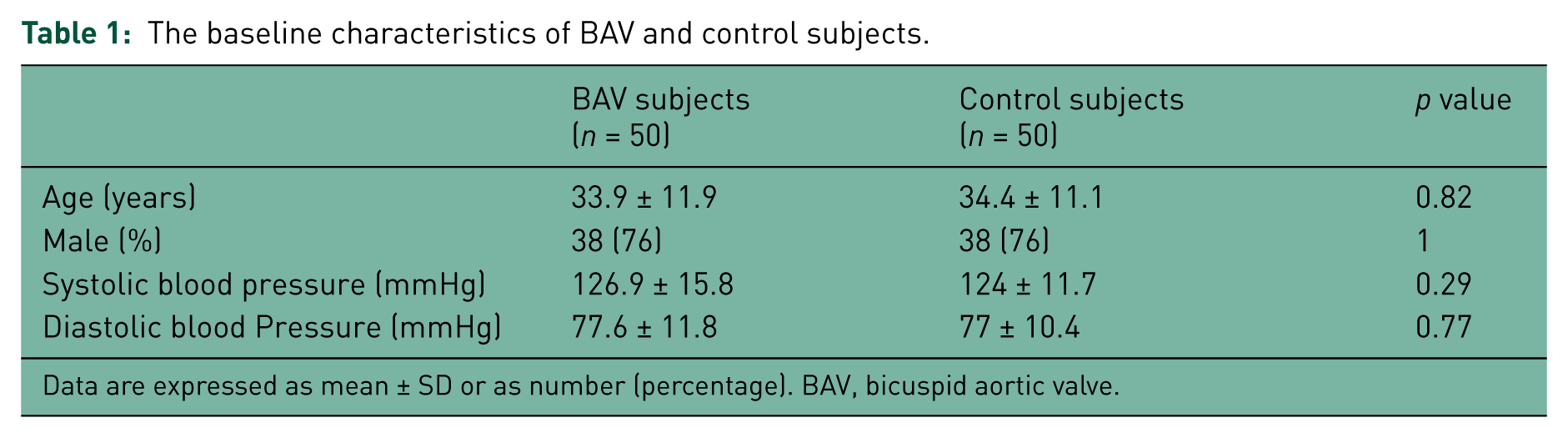
Data are expressed as mean ± SD or as number (percentage). BAV, bicuspid aortic valve.
Distensibility of the aorta
As shown in Figure 2, the BAV groups had significantly reduced proximal aortic distensibility compared with the control group (0.00298 ± 0.0023 and 0.00805 ± 0.0028 cm2 dynes−1 × 10−6, respectively, p < 0.001). Of 50 BAV patients, 19 (38%) had AP and 31 (62%) had ML phenotype of their aortic valve. The aortic distensibility in AP (0.0028 ± 0.0024 cm2 dynes−1 × 10−6) and ML (0.0030 ± 0.0023 cm2 dynes−1 × 10−6) morphology was not significantly different (p = 0.70). The reduced distensibility showed no gender differences (p = 0.07). However, a significant decrease in the distensibility property with increasing age was noted (p = 0.03).

Comparison of aortic distensibility between groups. *p < 0.001 versus control group. AP, anteroposterior leaflet orientation; ML, mediolateral leaflet orientation; BAV, bicuspid aortic valve.
Discussion
This study shows that aortic distensibility is impaired in BAV patients with normal aortic size compared with healthy subjects with TAV. The predominant BAV morphology in our study group was ML phenotype (62%). The comparison of aortic distensibility between the BAV phenotypes revealed no significant difference. The prevalence of BAV was higher in men (76%). Nevertheless, male gender did not show a significant effect on the BAV morphology or aortic distensibility. Aortic distensibility was related to age; namely, there is a significant decrease in the distensibility property with aging.
The investigation of aortic distensibility in BAV patients by transthoracic echocardiography may be useful with the purpose of cardiovascular risk prevention and may serve as a clinical indicator of aortic wall deterioration [Oulego-Erroz et al. 2013]. Reduced aortic distensibility in BAV patients is in line with other studies [Nistri et al. 2002; Biner et al. 2009]. The aortic distensibility in our BAV patients was 0.00298 ± 0.0023 versus 0.00471 ± 0.00367 in the study by Nistri and colleagues [Nistri et al. 2008] and 0.00657 ±0.00 283 cm2 dynes−1×10−6 in the study by Pees and Michel-Behnke [Pees and Michel-Behnke, 2012]. Grotenhuis and colleagues, using an MRI technique, found that reduced aortic distensibility in patients with BAV increased leaflet stress and thus predisposed the patient to valve dysfunction including aortic regurgitation [Grotenhuis et al. 2007].
In childhood, the predominant BAV morphology is the AP phenotype [Fernandes et al. 2004; Mahle et al. 2010]. In adulthood, the phenotype distribution is less clear. The equal prevalence of AP and ML phenotype was reported by Ward [Ward, 2000] and a more prevalence of the AP morphology as great as 82% was described by Schaefer and colleagues [Schaefer et al. 2007]. In contrast, in this study the ML phenotype was the predominant BAV morphology at 62%. Moreover, no difference in aortic distensibility was observed between both BAV phenotypes. This finding is consistent with the results of Huang and colleagues who declared: ‘aortic elasticity had no correlation with different BAV phenotypes’ [Huang and Le Tan, 2014]. However, Pees and Michel-Behnke expressed that BAV morphology had a major role in the outcome of BAV disease so that the AP subtype is more prone to impaired aortic elasticity and the ML subtype is more likely to develop aortic valve dysfunction [Pees and Michel-Behnke, 2012]. Schaefer and colleagues also reported that BAV phenotype was an important predictor in the elastic properties and size of the aorta. This means that AP morphology is associated with a higher stiffer index, lower distensibility and larger diameter in the aorta [Schaefer et al. 2007]. It has been shown that a more severe degree of aortic wall degeneration occurs in patients with ML morphology [Russo et al. 2008]. Differences in the results of investigations might be due to the difference in inclusion criteria of patients. So, it is recommended that larger studies be performed on BAV patients with various conditions.
The gender distribution of our BAV patients was the same as that of other studies [Fernandes et al. 2004; Mahle et al. 2010], with 76% male patients. Likewise, consistent with the finding of Pees and Michel-Behnke’s study [Pees and Michel-Behnke, 2012], male gender does not have any significant effect on aortic distensibility.
In our study, aortic distensibility was related to age which seems to be in accordance with previous studies [Chue et al. 2013; Pees and Michel-Behnke, 2012]. Decreased arterial elasticity (including aortic) occurs with aging and ongoing atherosclerosis [Nistri et al. 2008; Santarpia et al. 2012].
Conclusions
Aortic distensibility assessed by transthoracic echocardiography is impaired in BAV patients with normal aortic diameter compared with healthy subjects with TAV. This means that reduced aortic elasticity is independent from aortic dilation and valve orientations. Large and prospective studies should define the precise role of aortic elasticity impairment in the incidence of aortic complications in BAV disease.
Footnotes
Acknowledgements
The present article was extracted from the thesis written by Dr Khavanin.
Funding
The research in this work was supported by Shiraz University of Medical Sciences with grant No 3076.
Conflict of interest statement
The authors have no conflicts of interest to declare.