
Abstract
Despite remarkable advances in identifying and managing coronary heart disease, the global burden of cardiovascular (CV) risk and levels of undetected, subclinical heart disease remain enormous. Substantial numbers of patients do not reach their therapeutic goals, others are unable to tolerate the treatments, half may fail to adhere to their programs, and in those who do attain their targets, major cardiovascular events may continue. Well-known risk factors, such as obesity and diabetes, have now gained the upper hand, with no evidence-based remedy capable of reversing this trend. All told, less than 1% of American adults and adolescents qualify for ideal CV health; world-wide, the growing prevalence of CV risk factors in children is imposing. A number of novel emerging drug therapies are in development, some recently approved for use in patients with familial hypercholesterolemia.
Hopefully, they will contribute significantly to the current therapeutic armamentarium. However, for meaningful improvement in total and residual CV risk, an optimal mix of all available modalities will likely be necessary, including earlier and more effective prevention, aggressive medical care, revascularization and device implantation, judicious use of novel agents, and reengineering of the environment.
Keywords
Introduction
Cardiovascular (CV) disease remains the leading cause of mortality in the USA and worldwide, and is largely prevented and partly controlled through the elimination of risk factors, with dyslipidemia being of major importance [Fuster et al. 2011]. Data reporting persistent lipid abnormalities reflect the now-different and evolving nature of CV risk and cardiovascular disease (CVD) epidemics that are blanketing the world. In France, at least one dyslipidemia persisted in 50.8% of all patients and in 71.1% of high-risk patients [Laforest et al. 2012]. Further, among those with high CV risk, abnormal levels of high-density lipoprotein (HDL-C) and/or triglycerides (TGs) were as prevalent as high values of low-density lipoprotein (LDL-C). In the USA, persisting low HDL-C levels are found in 67% of patients treated with statins for coronary heart disease (CHD) or risk equivalents [Roger et al. 2012]. In France, as in the EU and North America, only a portion of remaining abnormal lipid values is due to poor management [Ferrieres et al. 2004], but pharmacological control is currently challenging. These reports confirm observations from other venues about how dyslipidemia has changed over the past decades, and underscore the importance of addressing residual risk in managing patients with heart disease. Considering LDL-C is the primary treatment target in current guidelines, persistence of lipid abnormalities suggests that addition of agents targeting low HDL-C and/or high TG values might be warranted. In this communication, the origins of residual risk are viewed in a broader sense, looking at solutions that are in development, drug therapies that are in current use but are not sufficiently implemented, and lifestyle improvement, the ‘Rodney Dangerfield’ of interventions, which receives little respect, but is nonetheless imperative for the success of any comprehensive program.
In spite of remarkable progress in pharmacological, invasive, and surgical management of heart disease, as reflected in lowered incidence of myocardial infarction (MI) and CHD mortality, the prevalence of CV risk factors remains unacceptably high [Roger et al. 2012; NCHS, 2012]. For several reasons, detection of the volume of background risk in the population is difficult, and may be inapparent at points of contact using current techniques and thresholds, but may be captured by lifetime risk [Berry et al. 2012]. Lower mortality combined with high risk, in the setting of pandemics of obesity and diabetes in both adults and adolescents, paints a bleak picture of expanded morbidity over extended years of life, which may be followed by decreasing longevity, depending upon the interplay of variables. Fundamentally, most of these changes are due to Westernization of traditionally healthy indigent diets, the ageing of the population, urbanization within developing countries accompanied by more smoking, weight gain, and hypertension, and alarming decreases in physical activity, as sitting time replaces field time. In the USA, when high-risk adolescents grow older, and additional segments of the population are added to the health system, a perfect storm of CVD may be in the offing, with an unprecedented number of patients with multiple risk factors leading to high rates of disability and mortality.
Many molecular explanations, behavioral hypotheses, and mathematical models have been proposed to account for these phenomena, but fundamentally two still stand out: eating excessively, especially too much sugar, calories, salt, and processed foods devoid of fiber, all of which are absent from hunter-gatherer fare; and lack of adequate exercise, which was formerly an inherent part of most work details and recreation. Pathologically, sedentary lifestyles coincided with the beginning of the obesity epidemic. All told, in the USA the level of CV health in the population is abysmal, with < 1% achieving ideal CV health, and the rest of the world is not too far behind.
Reducing ‘residual risk’ is now a popular topic in publications of major cardiology journals, seminars, editorials, and reviews. Residual risk, as some would define it, is the risk for major CV events (MCVE) that remains after patients are treated to evidence-based LDL-C targets with statin drugs. However, residual risk in a broader sense exists with almost all drugs or interventions, because few completely eliminate either the substrate/pathology that led to the illness or the possibility of recurrence. With drug therapy, device implantation, or surgical treatment, there are always inherent limitations. Or some patients in whom, for genetic, constitutional, behavioral, or ill-understood reasons, a given treatment is not effective. Since CHD is common worldwide, statin drugs are among the most prescribed drugs globally. However, statin therapy, even when titrated aggressively to LDL-C targets < 1.8 mmol/L, still leaves around 70% of unwanted MCVE to unfold. It is sobering to reflect that after using the very drug that has changed cardiology so strikingly for the better, the total risk that remains after treatment is still greater than the risk that is eliminated in a majority of patients, even when the medication is taken as prescribed. For this reason, there is much work to be done.
The modern: molecular manipulation in order to raise HDL-C and lower LDL-C
Current therapies
The increasingly frequent finding of low HDL-C and TG levels in patients, and three decades of strong epidemiological associations of low HDL-C values with poor CV outcomes, has fueled significant effort to raise HDL pharmacologically [Sarwar et al. 2007; Barter et al. 2007b; Miller et al. 2008; Carey et al. 2010]. Indeed, the HDL Atherosclerosis Treatment Study (HATS) [Brown et al. 2001; deGoma et al. 2008] and the Arterial Biology for the Investigation of the Treatment Effects of Reducing Cholesterol 6-HDL and LDL Treatment Strategies in Atherosclerosis (ARBITER-6-HALTS) trial [Villines et al. 2010] impressed many practitioners with the clinical advantages of using niacin, which is capable of raising HDL-C by 15–35%. In the Emerging Risk Factors Collaboration [Di Angelantonio et al. 2009], HDL-C and non-HDL-C were largely independent from each other, and from TG levels and other risk factors; concentrations of non-HDL-C and HDL-C were each strongly associated with CHD risk, though in opposite directions. Practitioners quoted the adage that for each 0.02586 mmol/L rise in HDL-C, CHD risk fell by 2–3%, and mortality decreased by about 4–5% [Cardenas et al. 2008]. In patients with acute coronary syndrome (ACS) receiving stents, those with low HDL-C levels had 2.6 times the risk of death at 1 year of follow up than those without low HDL-C concentrations [Wolfram et al. 2006].
The recent Atherothrombosis Intervention in Metabolic Syndrome with Low HDL/High Triglycerides: Impact on Global Health Outcomes (AIM-HIGH) trial randomized CVD patients with atherogenic dyslipidemia to either extended-release niacin (1.0–2.0 g/day) and simvastatin, or placebo and simvastatin [Boden et al. 2011]. After 32 months, the study was stopped for futility, having found no benefit in the niacin group. Despite several methodological difficulties (e.g. inadequate design and control, underpowering, confounding) that were later debated, AIM-HIGH cast a palpable shadow on prescribing niacin. The larger, ongoing Treatment of HDL to Reduce the Incidence of Vascular Events (HPS2-THRIVE) study is examining the effects of statin monotherapy versus extended-release niacin/laropiprant with statins, and its report next year is expected to permit more definitive conclusions about the future of niacin therapy [HPS2-THRIVE. 2012]. Since low HDL-C concentrations are believed to increase CV risk by about 40%, if HPS2-THRIVE results fail to reflect such a relationship, the HDL hypothesis itself will be in question, or have to be modified.
HDL is a complex molecule which, in addition to its lipid actions, has antioxidant, antiatherogenic, anti-inflammatory, antithrombotic, and antiapoptotic properties, as well as further roles in the innate immune system and upon endothelial repair, mediated in part by endothelial progenitor cells [Kones, 2011, 2010]. Healthy HDL3 can efflux cholesterol from lipid-laden cells rapidly [Sankaranarayanan et al. 2010], and raising levels of apolipoprotein A-1 (apo A-1) is capable of lesion regression independently of high amounts of LDL-C in preclinical studies [Feig et al. 2011]. Although it is believed to exert its major effect through reverse cholesterol transport (RCT), the relative importance of the other cardioprotective functions of HDL, particularly preserving endothelial function and protection against oxidation of LDL, may change according to HDL composition. The functional capability of HDL depends upon its protein and lipid cargo, upon coexisting disease, and perhaps even upon the pathway taken to achieve a given state. At the present time, details about how HDL function changes during the various interventions of clinical interest are largely unknown.
Several recent scholarly reviews, however, summarize current information about HDL biology [Khera et al. 2011; Navab et al. 2011; Besler et al. 2011], and the important role it plays in macrophage cholesterol efflux within the general topic of RCT [Khera et al. 2011; Rosenson et al. 2012; Prosser et al. 2012; Brewer, 2011; Besler et al. 2012]. Basically, due to anatomic and functional heterogeneity, global HDL-C levels may not be a good surrogate for individual properties of the HDL molecule, particularly the crucial process of macrophage cholesterol efflux.
A major way in which pharmacologists have attempted to raise HDL-C is through inhibition of cholesteryl ester transfer protein (CETP). This glycoprotein facilitates the exchange of neutral lipids, cholesteryl esters in HDL particles, for TGs in apo B-containing lipoproteins, that is, with very-low-density lipoprotein (VLDL) or LDL, through a molecular tunnel. Interruption of this transfer by CETP inhibition is accompanied by a rise in HDL-C, and with some agents, a fall in LDL-C [Shinkai, 2012]. It is important to note the elevation in HDL-C observed is in concentration, since CETP inhibition actually produces an increase in large HDL, which is not as efficient in RCT as small HDL. As a result, there was considerable speculation about whether the HDL associated with CETP inhibition would be functional, an issue yet to be resolved.
Four CETP inhibitors have been investigated: torcetrapib, dalcetrapib, anacetrapib, and evacetrapib. In the ILLUMINATE study [Barter et al. 2007a], torcetrapib was found to elevate HDL-C levels by about 75%, impair endothelial function, and significantly raise CV events and mortality. Subsequent analysis revealed that hypertension and hypokalemia were related to hypersecretion of aldosterone and cortisol. In May 2012, the development of dalcetrapib was also discontinued, not because of similar off-target phenomena, but due to lack of efficacy. Specifically, dal-OUTCOMES, a large, randomized, double-blind, placebo-controlled phase III trial in stable patients following ACS, failed to show sufficient success in the primary outcome – the time to first occurrence of a composite (death due to CHD, major nonfatal coronary event or stroke) [Miller, 2012]. In addition, the degree of improvements in endothelial function, plaque volume, and inability to lower LDL-C and C-reactive protein were disappointing.
Anacetrapib was shown to raise HDL-C by 138%, lower LDL-C by 40%, reduce TG levels by 7%, and also lower lipoprotein(a) by 36% in relation to placebo [Yvan-Charvet et al. 2010; Cannon et al. 2010]. No changes in blood pressure or serum electrolytes were observed. In view of these remarkable results, Merck is proceeding with the Randomized EValuation of the Effects of Anacetrapib Through Lipid-modification (REVEAL) study, a large randomized, double-blind study in secondary prevention patients, which will examine the effects of anacetrapib versus placebo upon coronary death, MI, or a coronary revascularization procedure [REVEAL, 2012].
Evacetrapib, the last of the CETP inhibitors being discussed, has been found to be safe and well tolerated either as monotherapy or in combination with statins in patients with either high LDL-C or low HDL-C [Nicholls et al. 2011]. The drug was considered efficacious, raising HDL-C by up to 129%, lowering LDL-C by as much as 36%, and reducing TGs by up to 11%. As a result, a large phase III clinical trial is being planned by Eli Lilly in the near future.
Finally, it should be mentioned that not all CETP inhibitors share the same mechanism of action, properties in CETP binding, time dependence, potency, ability to transfer neutral lipids between HDL and apo B-containing lipoproteins, and final products [Ranalletta et al. 2010; Niesor et al. 2010]. Hence, while dalcetrapib was ‘weaker’ than torcetrapib or anacetrapib, actually more of a CETP ‘modulator’ than a CETP inhibitor, it was hoped that selective preservation of pre-β-HDL particles would result in greater antiatherogenicity than predicted from the comparatively modest rise in HDL-C associated with the former. Despite this disappointment, binding characteristics of CETP-mediated lipid exchange suggest that design of novel agents may be possible in the future [Koivuniemi et al. 2012].
Emerging drug therapies
Additional approaches to HDL treatments include use of apo A-1 upregulators (such as RVX-208), delipidated pre-β-HDL [Waksman et al. 2010], reconstituted apo A-1/HDL [Tardif et al. 2007], and apo A-1 mimetic peptides [Bloedon et al. 2008]. Infusion of CSL-112, human apo A-1 reconstituted with phosphatidylcholine to resemble HDL, and a successor to the prior molecule CSL-111 [Bloedon et al. 2008], robustly promotes cholesterol efflux from macrophages when added to serum of volunteers. CSL-112 leads to raised levels of pre-β1-HDL, with efflux mediated by ATP-binding cassette (ABC) ABCA1, and is in phase II development in ACS patients [Khera et al. 2011]. CER-001 (Cerenis Therapeutics, Labège, France), the first pre-β-HDL mimetic, is in a phase II trial: Can HDL Infusions Significantly Quicken Atherosclerosis Regression (CHI-SQUARE) in 500 ACS patients, with preliminary results due later this year.
Among hypolipidemic agents, mipomersen (ISIS Pharmaceuticals, Carlsbad, CA, USA/Genzyme, Cambridge, MA, USA) is an apo B 20-mer antisense oligonucleotide targeting apo B-100. The sequence of nucleotides in mipomersen is complementary to the sequence in the coding region of apo B mRNA. Binding to the drug causes degradation of the nascent mRNA complex, lower hepatic synthesis of apo B, and a reduction in the amounts of VLDL and LDL released into the circulation [Ricotta and Frishman, 2012; Parhofer, 2012]. The drug is given by injection, and there are now four phase III trials in patients with homozygous familial hypercholesterolemia (FH), or severe hypercholesterolemia, and a phase II study in high-risk patients intolerant to statins [Visser et al. 2012]. In one phase III trial recently reported [Stein et al. 2012a], mipomersen was able to reduce mean LDL-C by 28%, apo B 26.3%, total cholesterol 19.4%, and lipoprotein(a) 21.1% in patients with heterozygous FH and CHD beyond values achieved with traditional therapies. Hepatic fat retention and elevations in alanine aminotransferases have caused concern about the possibility of irreversible liver damage or cirrhosis long term.
Lomitapide (Aegerion Pharmaceuticals, Cambridge, MA, USA) is an oral inhibitor of the microsomal TG transfer protein, an enzyme necessary for the production and secretion of VLDL and LDL in the liver and chylomicrons in the intestine, which has just completed a phase III trial in homozygous FH patients. The drug lowers LDL-C by about 40% accompanied by reductions in TGs and other apo B-containing lipoproteins, including lipoprotein(a). Intestinal side effects, elevations in hepatic enzymes, deficiencies in fat-soluble vitamins, and hepatic steatosis have been reported. It is likely that special certification for physicians and pharmacies will be required to prescribe and dispense the drug only to appropriate patients in the USA.
Monoclonal antibodies to proprotein convertase subtilisin/kexin 9 (PCSK9), an enzyme controlling degradation of LDL receptors, have generated considerable interest. One of these, REGN727 (Sanofi, Paris, France/Regeneron Pharmaceuticals, Inc., Tarrytown, NY, USA), given subcutaneously, completed a phase II trial in patients with heterozygous FH taking atorvastatin and ezetimibe [Stein et al. 2012b]. Significant reductions in LDL-C, apo B, non-HDL-C, and lipoprotein(a) were reported. An antisense oligonucleotide, ALN-PCS (Alnylam, Cambridge, MA) targeted to silence PCSK9 mRNA, has also completed a phase I study in patients with severe hypercholesterolemia not being treated with statins. Such agents, now being explored as add-on therapy to statins, may eventually have considerable success if adverse effects are not limiting.
Other future targets being considered, some mentioned at the 80th Congress of the European Atherosclerosis Society in Milan, were RNA-based therapeutics targeting apo C-III in hypertriglyceridemic patients, targeting remnant lipoproteins in diabetics, novel manipulations of ABC transporters, inhibition of endothelial protein kinase C-βII to protect endothelial function, altering vascular smooth muscle phenotype using endothelial microRNAs, targeting specific macrophage subsets to reduce inflammation, supporting regulatory T (Treg)-cell function (Foxp3+ Treg cells) to inhibit atherogenesis, and modulation of endothelial progenitor cell populations to improve endothelial repair.
The old-fashioned: controlling risk through better performance and adherence
In the original Treating to New Targets (TNT) study, some 9200 patients with CHD and LDL-C < 3.3 mmol/L received either atorvastatin 10 mg or 80 mg/day, and were observed for an initial MCVE. In the high-dose group who attained their target, an LDL-C between 1.8 mmol/L and 2.6 mmol/L (mean = 2.0 mmol/L), 8.7% developed a major event within the 5-year follow-up period [Barter et al. 2007b]. An inverse relationship existed between HDL-C levels and MCVE, suggesting HDL-C was an independent risk factor for CVD. Even though the study was retrospective, together with epidemiological and other preclinical data, the residual risk observed was attributed to low levels of HDL-C. A recent re-analysis of those data [Mora et al. 2012], however, revealed that the relationship between low HDL-C and poor prognosis disappeared when adjustments were made for baseline apolipoproteins. In addition, the significant remaining determinants of residual risk after those adjustments included elevated body mass index (BMI), smoking, hypertension, and diabetes. According to the authors’ new, more comprehensive multivariable model, a multifactorial approach to management was advised, since when LDL-C is within targets, control of other factors may become more important.
In this regard, it is appropriate to recall data reported by the Justification for the Use of Statins in Prevention: an Intervention Trial Evaluating Rosuvastatin (JUPITER) study group [Ridker et al, 2010]. Using the JUPITER trial cohort, these investigators found no relationship between HDL-C levels and CV risk in patients treated with rosuvastatin 20 mg (with a median on-treatment LDL-C level of 1.42 mmol/L; interquartile range 1.14–1.86). They concluded that in patients who attained low values of LDL-C, HDL-C concentrations were no longer predictive of additional CV risk. Many clinical examples of a dissociation between HDL-C concentrations and CV risk are known, and are supported by preclinical evidence indicating that only 3–5% of the total HDL-C mass is derived from tissue macrophages, with the majority originating in the liver and intestine [Haghpassand et al. 2001].
Turning attention to these nonlipid factors found to predict residual risk, performance in achieving goals and targets can be improved considerably. After smoking, maintaining a healthy body weight is a second suitable target, because it is closely associated with hypertension, the atherogenic triad, diabetes, and ischemic heart disease. In the USA, more than two thirds of the population is overweight, and half of those, about one third, are obese. When dual-energy X-ray absorptiometry is used to gauge obesity instead of BMI, 48% of women and 25% of men are reclassified upward as obese [Shah and Braverman, 2012]. The frequency of false-negative BMIs indicates that the prevalence of obesity, as imposing as it appears, is currently being significantly underestimated. Even so, a recent study clearly showed that for every 4 kg/m2 rise in BMI, there is a 26% increase in CHD [Nordestgaard et al. 2012]. When genes known to be associated with obesity are incorporated in the analysis, for each 4 kg/m2 rise in BMI, there is a 52% increase in CHD. In addition, for each rise of 1 mmol/L in nonfasting glucose, there is a > 24% increase in CHD. The crushing burden of rising overweight and obesity has no end in sight, has not been given sufficient priority, and is often obfuscated by discussion of details that may be relevant, but distract to undermine effectiveness. Tragically, the only measure that has succeeded in reversing obesity to some extent, but with caveats, is bariatric surgery. Other than this, there is no evidence-based, long-term medical treatment for serious weight gain being used in the population. The evidence linking higher amounts of moderate-to-vigorous physical activity with lower prevalence of diabetes, the metabolic syndrome, and CHD is strong, and cardiorespiratory fitness predicts a reduced lifetime risk for CVD at all ages, suggesting that a new urgency to discourage sedentary behaviors at a young age is in order [Berry et al. 2011]. From 1984 to the present, attempts to promote exercise in the USA have been unsuccessful, although they have been repackaged several times.
Control of elevations in LDL-C is reported at about 48% in the EU [Gitt et al. 2012], 53% in the UK [Kotseva et al. 2012], but was decidedly improved at approximately 73% for all patients in the Lipid Treatment Assessment Project 2 (L-TAP-2) [Waters et al. 2009]. In high-risk patients, however, target attainment was lower at 67%, and only 35% of patients with two or more risk factors achieved optional goals of LDL-C < 1.8 mmol/L. Control of hypertension has risen to around 48%, and control of HbA1c in diabetes surged from 27% to about 50–57% [George et al. 2001; Malik et al. 2007; Cheung et al. 2009]. While performance today is nearly double what it once was, there is still an appreciable shortfall. In addition, current figures may not reflect the many patients that remain undiagnosed. If all risk factors are addressed impeccably, a substantial difference can be made, but achieving control of three or more risk factors is uncommon, averaging about 12% in diabetics [Cheung et al. 2009]. When inadequate patient adherence is factored in, generally averaging below 50%, the amount of risk that is unaddressed, but potentially reversible, becomes large. Poor adherence to medications is an immense obstacle to treatment, and every opportunity to motivate compliance through patient education should be utilized.
There is little debate that in patients with CHD, beta blockers, angiotensin-converting-enzyme (ACE) inhibitors, statins, and antiplatelet agents are of value in secondary prevention. In patients with stroke, treating hypertension with diuretics, beta blockers, ACE inhibitors, or angiotensin-receptor blockers, and the use of antiplatelet drugs and statins is also recommended. The Prospective Urban Rural Epidemiology (PURE) study examined the rates of CHD and stroke, and the use of these evidence-based drugs that are readily available and inexpensive [Yusuf et al. 2011]. Conducted in adults from urban and rural areas in countries divided into four groups according to income, about half of all patients received none of the drugs. In high-income countries, use was a little over 50%, in medium-income countries about 25–50% received the treatments, and in low-income countries fewer than 10% of patients received these therapies, but individual preferences contributed to these numbers. Hence, not only physician and patient behaviors influence risk, but social, economic, and policy priorities as well.
The novel and unique: the polypill and environmental modification
The polypill
One strategy to improve distribution, use, and adherence to preventive CV medications is the use of the ‘polypill’, a capsule or pill containing four or more active ingredients in a fixed-dose combination. Simplicity, intuitiveness, and low cost have made this approach attractive, particularly for underserved populations in developing nations. As originally envisioned [Wald and Law, 2003], the rationale behind this approach is the monotone relationship between the levels of risk factors and outcomes within the physiological range of interest. Since critical low-end thresholds usually do not exist, lowering blood pressure and cholesterol will benefit the preponderance of recipients [Wald and Wald, 2010]. Therefore, selection of patients is made on the basis of overall CV risk, usually using age as a surrogate with a common cutoff of 50–55 years, rather than the values of the risk factors. The basis for using polypills is drawn from recent advances in population-based prevention, the continuum of global risk over time rather than the artificial division into primary and secondary prevention, the increasing reliance upon total CV risk for treatment decisions rather than absolute values in, for example, LDL-C, and treating to targets [Kones, 2011]. A polypill with three antihypertensives and a statin would prevent most heart disease, with aspirin administered electively for secondary prevention. One third of people taking this pill from 55 years of age were expected to benefit, extending life by an average of 11 years, free from a MCVE.
The Indian Polycap Study (TIPS) employed a capsule containing hydrochlorothiazide (12·5 mg), atenolol (50 mg), ramipril (5 mg), simvastatin (20 mg), and aspirin (100 mg) given to 2053 Indian subjects without CVD, but with at least one risk factor [Yusuf et al. 2009]. Extrapolating the results of this 12-week study would result in a 62% and 48% reduction in relative risk for CHD and stroke respectively, well short of the 80% and 88% predicted. While the treatment was well tolerated, acceptance and adherence were still barriers, with approximately 15% of participants discontinuing the pill.
The Program to Improve Life and Longevity (PILL) study reported similar findings in 378 individuals with no indication for any component of the polypill, and an estimated 5-year Framingham Risk Score (FRS) of > 7.5%, randomized to a polypill containing aspirin 75 mg, lisinopril 10 mg, hydrochlorothiazide 12.5 mg, and simvastatin 20 mg or placebo for 12 weeks [PILL Collaborative Group 2011]. Primary care patients in the polypill group enjoyed a fall of 0.8 mmol/L in LDL-C, and 9 mmHg in systolic pressure, translating to a 60% long-term reduction in risk for both CHD and ischemic stroke. Adverse effects were noted in 58% of the treated group (versus 42% in the placebo group), and a 23% discontinuance rate in the polypill arm (18%, placebo).
With additional demonstration of feasibility and patient acceptance of the polypill concept in primary [Soliman et al. 2011], and secondary prevention patients [Fuster and Sanz, 2007; Fuster, 2009; Robinson, 2009; Sanz, 2011], use of the polypill evolved into one part of a global strategy to lower the inordinate burden of CVD in developing countries, so critically needed in view of the striking underuse of proven preventative drugs [Lonn et al. 2010], found by the PURE investigators, mentioned above.
In The Second Indian Polycap Study (TIPS-2), a ‘full’ dose of the polycap used in the TIPS study, consisting of two capsules, each containing hydrochlorothiazide (12·5 mg), atenolol (50 mg), ramipril (5 mg), simvastatin (20 mg), and aspirin (100 mg), were found to lower blood pressure and LDL-C modestly further than the ‘single’ lower dose, with no increase in adverse effects [Yusuf et al. 2012].
A randomized, double-blind crossover study of 84 primary care patients over 50 years of age was conducted using a polypill composed of amlodipine 2.5 mg, losartan 25 mg, hydrochlorothiazide 12.5 mg, and simvastatin 40 mg for 12 weeks [Wald et al. 2012]. There was a 12/11% reduction in systolic/diastolic blood pressures (mean systolic, -17.9 mmHg, diastolic, -9.8 mmHg) and a 38% fall in LDL-C (-1.1 mmol/L). About 29% suffered adverse effects, and 11% reported myalgias. Projecting these admittedly short-term data would result in a reduction of 72% and 64% in event rates for CHD and stroke, respectively. When used long term after age 50, about 28% of users could avoid or delay such events in their lifetime, the equivalent of adding 11 event-free years to their life.
Use of polypills remains a controversial and highly debated topic among physicians and researchers, and the enthusiasm driven by the need for an effective, inexpensive, and population-based agent may not be matched by evidence. In addition to the open questions concerning the extent of risk reduction achieved, underestimated adverse effects of several agents administered widely in combination, cost-effectiveness, adherence, physician acceptability, under- and overtreatment, uncertainty about the ideal or gender- and disease-specific components, dose, types of polypills suitable for subpopulations, and consequences of lack of monitoring, there are also major philosophical and ethical issues. First, pharmaceutical control of risk factors has not been successful in abating the tsunami of CV risk, which is driven by obesity, physical inactivity, and poor nutrition. The mathematical estimation of a reduction in MCVE by polypills may therefore be ‘fool’s gold’. Second, the fundamental belief that a disease should be managed through specific diagnosis, evaluation of the extent of disease, and individualized risk assessment, treatment, and monitoring is being replaced with an unproven shotgun approach. Third, the use of polypills conveys the wrong message to the public, that there is a magic bullet to prevent heart disease, and may dissuade individuals from making fundamental changes in lifestyle, which are more effective than a polypill, and will probably be necessary even in spite of a polypill program. In fact, physical activity itself has been called the ideal polypill, which is now shamefully neglected, and the ideal ‘polymeal’ in the form of the Mediterranean diet has been eclipsed by harmful Western fare. Fourth, the interest in polypills arises from two phenomena: (a) frustration and desperation of physicians and health officials that the poor rate of primordial prevention (5%), low adherence to prescribed therapies (< 50%), poor compliance with lifestyle prescriptions (< 15%), and disappointing control of multiple risk factors in the same patient (5–10%) continues; and (b) financial interests, both in savings for health programs, and in pharmaceutical profits [Cannon 2009; Malekzadeh et al. 2010; Sanz, 2011; Viera, 2011; Dabhadkar et al. 2011; Franklin et al. 2004].
There are also specific objections to overtreating patients for conditions they do not have, and undertreating others whose risk requires more than the fixed doses provided, or different agents. Interests of such subpopulations, that is, undertreated, inappropriately treated, or with adverse effects, some to unneeded constituents, would basically be dismissed in favor of the greater good. While statistically acceptable to the health planner at a computer, it would not be acceptable to the patient who develops adverse gastrointestinal or intracerebral hemorrhage from aspirin.
Compared to lifestyle improvement through behavior modification, the use of a polypill does not depend heavily upon personal responsibility, since instructions are simple. Unfortunately, assuming that traditional beliefs confer an undisputed advantage may be incorrect. For example, adherence to medications in secondary prevention remained abysmal even after they were provided without copays in the Post-Myocardial Infarction Free Rx Event and Economic Evaluation (MI FREEE) trial [Choudhry et al. 2011]. Adherence to harmful diets and inactivity may be greater than adherence to polypills, and the protection afforded by the polypill, although convenient, remains incomplete. Although current evidence suggests use of polypills succeeds in lowering CV risk, long-term improvement in outcomes in large, randomized trials remains to be seen.
On the other hand, polypill use offers advantages that include a partial solution to poor access to care, budget constraints, adherence, some medication errors, and administration does not require a physician in attendance. The polypill approach has received the attention of the Wellcome Trust and World Health Organization, and is endorsed by the World Heart Federation and other authorities concerned about the inordinate burden of CHD and human cost [Grabowski et al. 2012; Sanz and Fuster, 2011]. Use of polypills has immense potential, few side effects, supportive evidence is strong, and comparable alternatives are sparse. The expense of large-scale randomized trials would likely be impractical in view of the current need to implement such programs immediately. In populated areas of lesser developed nations with limited resources, the polypill may ultimately provide better protection than expensive, sophisticated care [Braunwald, 2012; Kovacic 2012; Lonn et al. 2010].
The Use of a Multidrug Pill In Reducing cardiovascular Events (UMPIRE) study, with results soon to be presented at the American Heart Association Sessions, Fixed Dose Combination Drug for Secondary prevention (FOCUS) [Sanz et al. 2011], Guidelines Adherence with the Polypill (GAP) study, Improving Adherence Using Combination Therapy (IMPACT) trial, and the 5-year Heart Outcomes Prevention Evaluation (HOPE)-3 studies are ongoing and may help to answer some of the open questions and reservations concerning the use of polypills. Food and Drug Administration approval for a polypill is anticipated in the USA within a year, and within a similar timeframe elsewhere.
Ecological (environmental) control
Among the population approaches to optimize lifestyle habits, particularly to improve nutrition, physical activity, and discourage smoking, environmental restructuring has received considerable recent attention. One common strategy has been to divide active living into domains, such as health policy; behavior, regarding settings and access; behavior, regarding recreation, transport, occupation, and household; perceived environment; and intrapersonal. Within each category, modifiable variables that relate to health risk are candidates to be used in promoting healthy default behaviors. An illustration of such an approach for obesity appears in Figure 1 [NHLBI, 2004]. The goal is to identify those influences that will affect behaviors positively and improve health outcomes. Although analysis of such ecological systems is complex, finding pathways to tangible results is possible [Huang et al. 2009].
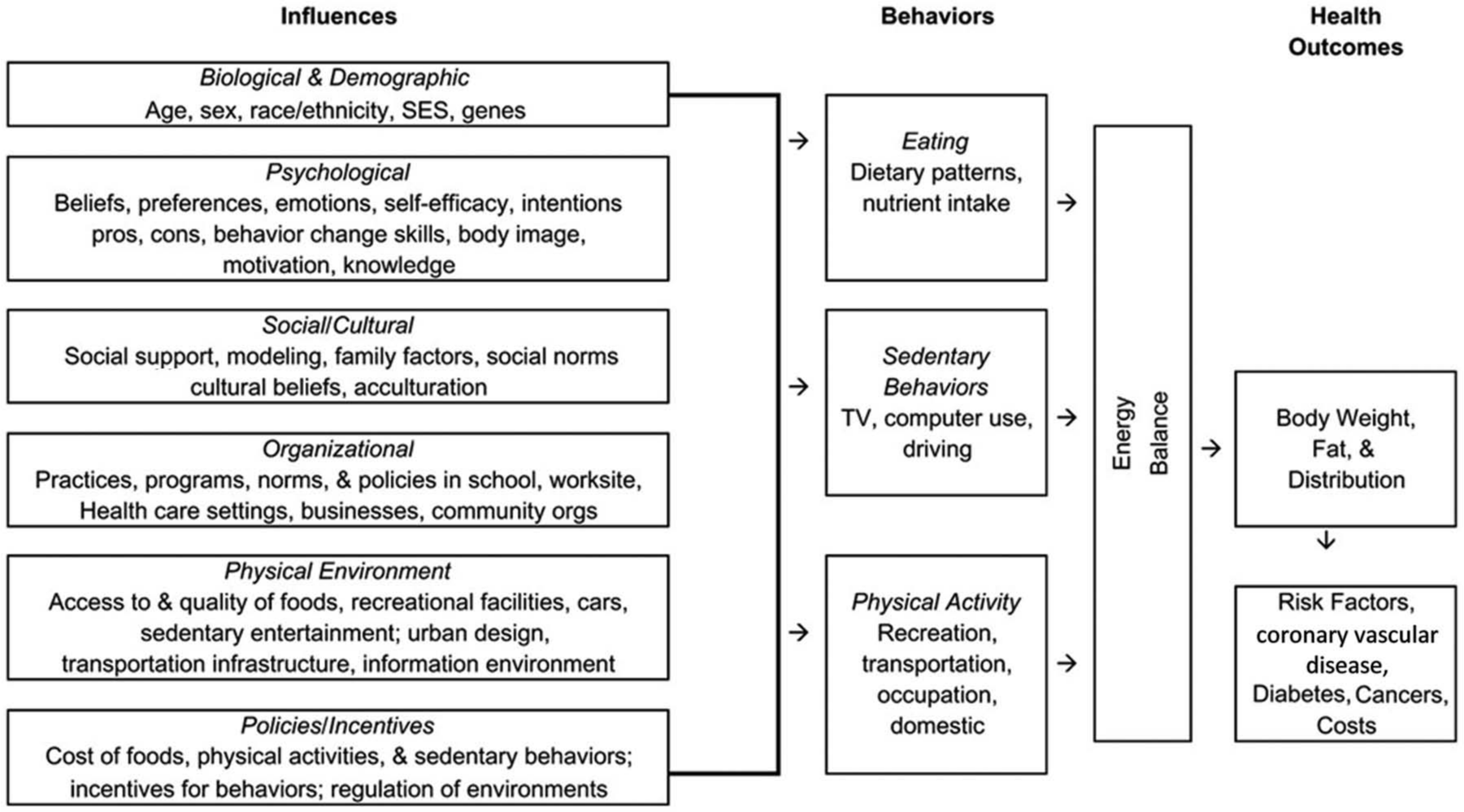
The ecological theory of obesity and cardiovascular risk. Biological, social, environmental, and health policy factors may influence individual behaviors to alter energy balance. As a result, body weight rises, predisposing to disease. (Reproduced from the National Heart, Lung and Blood Institute, National Institutes of Health, Workshop on Predictors of Obesity, Weight Gain, Diet, and Physical Activity, held 4–5 August 2004, Bethesda, MD, USA. Reproduced under authority of US 17 U.S.C. § 105 as noncopyright material in the public domain.)
Considering many population strategies to improve diet, physical activity, and smoking cessation, the American Heart Association issued a scientific statement summarizing currently available data [Mozaffarian et al. 2012]. Strategies were considered in six broad domains: (a) media and educational campaigns; (b) labeling and consumer information; (c) taxation, subsidies, and other economic incentives; (d) school and workplace approaches; (e) local environmental changes; and (f) direct restrictions and mandates. The document identified and graded evidence in terms of weight and consistency (strong, conflicting, favorable, weak, or ineffective), as well as the strength of the respective sources (randomized trials, single trial, or nonrandomized multiple, or consensus, expert opinion, or standard of care). This extensive systematic review provided an evidence-based framework for further study, evaluation, and development of future policy changes. Since the details are extensive and largely nonmedical, the reader is referred directly to that document for further information.
Conclusion
Residual risk is common, and arises not only from incompletely addressed lipoprotein factors, but by other variables, many of which may be eliminated with current therapies. Additional, novel, evidence-based molecules are needed to close the residual risk gap, and although disappointments are evident, a number of potentially rewarding agents are under investigation. As research fills in further steps involved in the pathogenesis of atherosclerosis, undoubtedly additional targets for therapy will present themselves. One example is the recently described interruption of endothelial activation/vascular inflammatory response by inhibition of NF-κB transcription factors [Sun et al. 2012]. At the moment, it would be premature to declare HDL-based approaches unworthy.
However, in the interim, attention to primordial, primary, and secondary prevention remains of utmost initial importance, since this approach will have greater impact in the here and now. Lifestyle improvement is the most fundamental and essential of all interventions, is evidence-based, and should be a priority, yet it is largely ignored in today’s world. This wide chasm in prioritization and the commitment that follows impairs public health, and specifically, CV outcomes. Together with more effective use of the drugs now available, much low-lying fruit is within our reach, and the opportunity should not be lost. Unless basic changes are made, and all effective resources are partnered wisely, the current trajectory in managing CVD will be unsustainable. Combining intensive primordial and primary prevention, wider use of current medications with known benefit, and judicious choice of newer agents will hopefully reduce the burden of CV risk and improve patient outcomes.
Footnotes
Acknowledgements
The author wishes to thank Michelle Delaney for her astuteness, computer skills, untiring assistance, and valuable suggestions in the preparation of this manuscript.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The author reports no conflict of interest in this work.