
Abstract
Americans are under assault by a fierce epidemic of obesity, diabetes, and cardiovascular disease, of their own doing. Lowered death rates from heart disease and reduced rates of smoking are seriously threatened by the inexorable rise in overweight and obesity. Latest data indicate that 32% of children are overweight or obese, and fewer than 17% exercise sufficiently. Over 68% of adults are overweight, 35% are obese, nearly 40% fulfill criteria for the metabolic syndrome, 8–13% have diabetes, 34% have hypertension, 36% have prehypertension, 29% have prediabetes, 15% of the population with either diabetes, hypertension, or dyslipidemia are undiagnosed, 59% engage in no vigorous activity, and fewer than 5% of the US population qualifies for the American Heart Association (AHA) definition of ideal cardiovascular health. Health, nutrition, and exercise illiteracy is prevalent, while misinformation and unrealistic expectations are the norm. Half of American adults have at least one cardiovascular risk factor. Up to 65% do not have their conventional risk biomarkers under control. Of those patients with multiple risk factors, fewer than 10% have all of them adequately controlled. Even when patients are treated according to evidence-based protocols, about 70% of cardiac events remain unaddressed. Undertreatment is also common. Poor patient adherence, probably well below 50%, adds further difficulty in reducing cardiovascular risk. Available data indicate that only a modest fraction of the total cardiovascular risk burden in the population is actually now being eliminated. A fresh view of these issues, a change in current philosophy, leading to new and different, multimechanistic methods of prevention may be needed. Adherence to published guidelines will improve substantially outcomes in both primary and secondary prevention. Primordial prevention, which does not allow risk values to appear in a population, affords more complete protection than subsequent partial reversal of elevated risk factors or biomarkers. Current evidence supports recent calls for massive educational programs supporting primordial prevention, individual responsibility and pride in achieving population-wide ideal cardiovascular health through lifestyle modification. Environmental and social changes will be necessary, along with major supportive adjustments in the food industry and the assistance of the media. Cooperation is critical to the success of such an initiative.
Keywords
‘We Have Met the Enemy and He Is Us…’
(Walter Kelly, Pogo cartoonist, 1970)
Introduction
The goal of medicine is to prevent disease, relieve suffering, and prolong life. Traditionally, true ways to prevent illness have been both revered and preferred, but it has been suggested that this view is only intuitive, not evidence based, and cost-ineffective. In the past few years there has been considerable debate about whether prevention is worthwhile, and during this time we have ignored powerful, simple measures, leaving significant potential to avoid disease unrealized. Is, in fact, an ounce of prevention worth a pound of cure, or not? Before examining the evidence, it is appropriate to ask: what is ‘worthwhile’, what is ‘prevention’, and are we actually doing what is needed to generate the benefits of prevention?
What is worthwhile?
After analyzing the cost of quality-adjusted life-years of many preventive interventions, Cohen and colleagues concluded that general pronouncements about the cost-saving potential of prevention were unjustified [Cohen et al. 2008]. The greater significance of their findings, however, was that cost-effectiveness is a function of the particular preventive measure considered and the referenced illness. Russel recognized benefits in preventing chronic disease, but maintained that the preponderance of evidence showed that preventive measures increased healthcare costs, with only about 20% being cost-effective [Russel, 2009].
These analyses raise several issues. First, and an important one, is that the intention of preventive medicine is to delay disease and forestall anguish and disability, optimize productive functioning, and contribute to happiness, rather than the newly revised assignment of preventive measures to reduce costs. As Wilson observed, holding clinical preventive services to the standard of saving money is a uniquely stringent requirement for a medical service, which is never applied to disease care [Wilson, 2009a]. Second, these discussions focused on whether expanding healthcare to include more preventive interventions was capable of improving the healthcare budget. Intensive screening to detect more high-risk patients or lowering biomarker criteria to include larger numbers of patients for care obviously raises required resources, but may not be the best choice. Third, there are detailed, well-developed data showing considerable benefits of prevention, citing returns of 5.6 : 1 on investments [Trust for America's Health, 2008; Cohen et al. 2007]. Fourth, the commentary is based upon the symptom-reactive, disease-oriented paradigm of medical care that currently exists, wherein only 54.9% of all recommended effective treatments are routinely employed [McGlynn et al. 2003]. Woolf disparaged this double standard, that preventive care should save money, but a high price of disease care is to be expected, and he called for a clearer and more discriminating analysis [Woolf, 2009]. Currently, we underinvest in preventive care, usually representing ≤3% of the healthcare budget, which may have roots in the impersonal nature of future benefits, inertia of societal change, even individual neural functioning [Hemenway, 2010]. The unexpected and perplexing resistance to implementing proven methods of saving large numbers of lives through prevention has yet to be fully understood [Grundy, 2005].
However, it is possible to vastly improve our yield through judicious selection. Of 25 preventive services endorsed by the US Preventive Services Task Force and the Advisory Committee on Immunization Practices, emphasizing core measures with high priorities may produce much higher returns than others [Maciosek et al. 2006]. Therefore, one question to be answered is better framed: how can we identify preventive interventions that will keep cost-effectiveness attractive and facilitate grassroots improvement in public health? For example, since implantations of cardioverter defibrillators and left ventricular assist devices are costly, what can be done fundamentally, at an earlier stage in the disease, to obviate the need for such intensive and high-technology care?
Lifestyle measures are effective
In August 2007, the National Commission on Prevention Priorities found that over 100,000 lives per year could be saved through intensifying five services to 90% of the identified population. Those services were: (i) smoking cessation counseling; (ii) breast cancer screening in women over 40 years of age; (iii) screening for colorectal cancer in adults ≥50 years of age; (iv) influenza immunizations in adults ≥50 years of age; (v) the use of aspirin in high-risk cardiovascular patients [National Commission on Prevention Priorities, 2007a, 2007b]. Their report identified a number of additional specific services for which there was a substantial return on investment. The extensive review concluded that significant underuse of effective preventive care in the USA resulted in lost lives, unnecessary poor health, and inefficient use of healthcare resources.
Lifestyle changes in smoking cessation, nutrition, and physical activity typically show excellent cost-effectiveness in lowering the burden of disease, especially with respect to obesity, future diabetes, heart disease and cancer [Russel, 2009; National Institutes of Health et al. 2007]. Other than tobacco use, lifestyle and personal behavior amount to between 50% and 80% of factors that contribute to chronic disease. Lifestyle interventions, in which the patient can participate, result in more than a fivefold return when compared with most other clinical preventive measures, even when imperfect [Trust for America's Health, 2008]. In part, this is because the target conditions are costly. Hence, for lifestyle interventions and chronic degenerative diseases, much of the argument about the ‘illusion’ of economic benefits disappears. In addition, there are societal benefits that go further than the measured endpoints, beyond healthcare. The absurd proposal that its potential success with cardiovascular disease, for instance, would prolong life and raise total projected expenses during additional years of life, is socially untenable and must be dismissed. Considerable evidence suggests true prevention (see below) works better than drugs, lasts longer than percutaneous coronary intervention (PCI), and is preferable to surgery in coronary artery disease (CAD), but only if it is done early in life. The administrative aspects of implementing campaigns to encourage lifestyle changes, with advertisements, motivational materials, re-education, and, in this situation, enlisting multiple organizations and the media for support, are anticipated to require a higher fraction of resources invested. CAD, the leading cause of death and imposing public health problem worldwide, and the current obesity epidemic, which threatens to reverse recent gains, are of greatest concern [Fuster and Kelly, 2010; Koh, 2010]. There is also evidence that increases in life expectancy from reductions in smoking may also be offset by obesity [Stewart et al. 2009]. Fortunately, even relatively small increases in preventive services lead to substantial rewards in cardiovascular patients [Farley et al. 2010]. Nutritional advice is especially cost-effective, and its full potential may be greater than realized, since much of the data are from studies with older participants [Roux et al. 2008; Lindgren et al. 2003]. Increasing physical activity is an effective, safe technique for improving cardiovascular outcomes and weight management, especially so in individuals with the metabolic syndrome [Kim et al. 2010; Lee et al. 2010; Schrauwen-Hinderling et al. 2010; Stensvold et al. 2010; Haskell et al. 2007; Nelson et al. 2007; Thompson et al. 2007] and is endorsed worldwide by numerous authoritative bodies.
What is prevention?
Prevention has several meanings. When many physicians talk about prevention, they refer to screening tests, vaccinations, and prescribing medication for CAD, hypertension, and dyslipidemia to ‘prevent’ myocardial infarction and lethal cardiac events. To be sure, these measures are lifesaving. In one model, for each 10% increment in treatment of hypertension, an additional 14,000 deaths would be prevented annually in patients younger than 80 years of age [Farley et al. 2010]. The number of deaths prevented for every 10% increase in treatment of elevations of low-density lipoproteins (LDL) or using aspirin prophylaxis would be about 8000 apiece. Optimal use of all three measures could avoid up to 100,000 deaths annually. These potential returns are striking, and are based upon greater use of fewer, selected preventive services that will be effective.
Primary prevention, another common usage, refers to prevention of coronary disease before clinical heart disease is evident, a diagnosis is made, or an event has occurred, usually in patients with risk factors. Secondary prevention refers to delaying recurrence of cardiac events in patients who are already diagnosed with heart disease. When epidemiologists use the term prevention, they mean delaying the progression of disease, or postponing disease in all of its guises.
Prevention may also refer to a more fundamental, perhaps truer way to avoid disease, unrelated to prescription drugs or devices, a subject that has drawn insufficient interest from evidence-based medicine thus far. This includes what the patient can do personally to delay disease or risk factors, behavioral lifestyle measures that applied sufficiently over the anticipated incubation period of a disease can avoid the appearance of risk factors entirely. Such an approach is fruitful in CAD, since the incubation period extends over decades, begins in childhood, and results from common causes. The requirement for lifestyle change over a prolonged period also applies to secondary prevention, consistent with the slow change in the components of atherosclerotic plaques [Gonçalves et al. 2010].
In 1978, Strasser coined the term ‘primordial prevention’, referring to prevention attained through a self-directed lifestyle that did not allow risk factors to develop in a population [Strasser, 1978]. The Third International Heart Health Conference in Singapore, 1998, continued this theme, but interest has since waned. Most recently, the American Heart Association (AHA), in its synthesis of goals for 2020 to reduce the prevalence and mortality of heart disease, guided by the powerful concept of primordial prevention, highlighted ‘ideal cardiovascular health’ [Lloyd-Jones et al. 2010]. The AHA redefined ideal cardiovascular health as not only the absence of cardiovascular disease, but having a healthy lifestyle (i.e. absence of smoking, adequate exercise, defined superior diet score, and body mass index (BMI) <25 kg/m2), and ideal health factors (i.e. untreated normal values of blood cholesterol, blood pressure, and fasting glucose). Similar metrics to classify and monitor cardiovascular health in the population were also defined to facilitate a 20% improvement in heart health and simultaneous 20% reduction in cardiac and stroke deaths by year 2020.
The incubation periods of chronic degenerative diseases greatly exceed those of the acute diseases they replaced as the major causes of death over the last two centuries. Compared with acute fulminant infections, diabetes, for example, now a pediatric disease, develops over decades, with a delay of 9–12 years prior to diagnosis [Nathan and Herman, 2004]. By the time symptoms appear, patients with chronic diseases may have multiple lesions and elevations in systemic biomarkers, a relatively late stage in their natural history. This long asymptomatic period needs greater attention.
The burden of cardiovascular risk is high
Data from national surveys conducted approximately a decade apart, 1988–1994 and 1999–2002, showed no appreciable difference in the distribution of 10-year risk of developing CAD [Ajani and Ford, 2006]. Extending this period, in a review of the 18-year progress from 1988 to 2006, it was found that adherence to a healthy lifestyle actually decreased [Fryar et al. 2010]. Specifically, obesity (BMI ≥30 kg/m2) rose from 28% to 36%, physical activity frequency (12 sessions/month) dropped from 53% to 43%, consuming five or more portions of fruits and vegetables/day decreased from 42% to 26%, moderate alcohol intake rose from 40% to 51%, and smoking rates remained constant at approximately 26.5%. Overall adherence to these five health habits fell from 15% to 8%. Moreover, individuals with cardiovascular disease and diabetes were no more likely to adhere to healthy lifestyles than other respondents. In the year 2000, another analysis concluded that about 3% of American adults maintained a normal weight, consumed five portions of fruits and vegetables, engaged in regular exercise, and did not smoke [Reeves and Rafferty, 2005]. Despite exceptional effort from public agencies, vegetable consumption continues to fall. Presently it is estimated that <5%, perhaps as little as 0.5%, of the population satisfies the AHA definition of ideal cardiovascular health as described above [Lloyd-Jones et al. 2010]. Much of the data is self-reported, so the reality is likely to be worse.
Geoffrey Rose, a London physician and epidemiologist, wrote extensively comparing a high-risk strategy with a population-based strategy in reducing the burden of disease. He emphasized that the prevalence and impact of important diseases depend less upon a small number of patients at high risk, but more upon the collective behaviors and environment of society as a whole. Treating a small number of high-risk individuals intensively might be temporary, palliative, unsustainable, suffer from an inability to accurately identify risk, and ultimately not contribute greatly to the control of a disease. On the other hand, a population strategy affords only a small individual benefit, and requires a major change in the economic and political function of society [Rose, 1992, 1981].
Recently there has been renewed interested in population-wide approaches to prevention, as opposed to preventive and urgent interventions in high-risk individuals [Starfield et al. 2008]. A minority (<10%) of the population falls in the high-risk category, yet because the remaining population with average risk is huge, the majority of events will occur in the larger pool [Hingorani and Psaty, 2009; Lloyd-Jones et al. 2009]. Over 90% of cardiac events occur in patients with ≥1 risk factor, presently just under half of the population [Berger et al. 2010]. To reduce the greater number of events, lowering risk in the entire population is the more productive intervention. A fall in risk factors within the population, substantially pharmacological, accounts for 47–65% of the lowering of death rates during the past 40 years [Björck, et al. 2009; Capewell et al. 2009]. There are indications that these trends have been reversed recently due to increasing obesity and diabetes, and both observations underscore the power of risk-factor reduction in improving cardiovascular outcomes. The 2009 update on heart disease and stroke statistics provided current details on the continued high cardiovascular risk burden that Americans face [Lloyd-Jones et al. 2009]. About 34% have hypertension, 33% are overtly obese, 53% have visceral adiposity, 29% have prediabetes, 35% of men and 33% of women fulfill criteria for the metabolic syndrome, 59% admit they engage in no vigorous activity, 8% of diabetics are undiagnosed, and 32% of children (2–19 years of age) are overweight or obese. An additional analysis reported 36% with prehypertension, and 11.2% with both prediabetes and prehypertension.
The National Center for Health Statistics then released its summary, also based upon National Health and Nutrition Examination Survey (NHANES) data, noting that 45%, or 81 million American adults, have at least one of three major risk factors: hypertension, dyslipidemia or diabetes [Fryar et al. 2010]. About 13%, or 1 in 8 adults, have two of these conditions, and 3% have all three of them. This widespread risk burden was accompanied by an estimate that 8% of hypertensives, 8% of dyslipidemics, and 3% of diabetics, are undiagnosed, amounting to a total of about 15%, or 1 in 7 adults, with unrecognized but treatable diseases.
The statistic that 32% of American children and adolescents are overweight or obese is well known and, generally, a comparable situation now exists overseas [Ayer and Steinbeck, 2010; Olds et al. 2010; Stamatakis et al. 2010; Song et al. 2010; Ogden et al. 2008]. The majority of 4 year olds were found to have at least one risk factor in a recent Chilean study [Corvalán et al. 2010], while about 20% of adolescents aged 12–19 years have at least one abnormal lipid level in this country [Centers for Disease Control and Prevention, 2010a]. Approximately 17% of American high school students report engaging in less than the recommended amount of physical activity [Centers for Disease Control and Prevention, 2010b]. As with adults, excess weight is a result of a complex interaction between diet, physical activity, genetic, environmental, and social factors [Silventoinen et al. 2010]. TV watching, computer time, and video games are contributory [Wake et al. 2003], but even in adults, each hour of additional TV screen time raises the risk of death by 11%, with a clear inverse relationship between sitting time and longevity now evident [Dunstan et al. 2010]. Overweight children tend to become obese adults, and when they do, it is feared that the prevalence of diabetes and CAD will rise accordingly. Current pediatric guidelines recommend monitoring, intensive behavioral interventions, nutrition, and exercise [Whitlock et al. 2010]. A population-based, comprehensive approach to the prevention of obesity at multiple individual, environmental, and social levels has been proposed and discussed in detail [Blackburn et al. 2010; Heber, 2010; Kumanyika et al. 2008].
The Institute of Medicine (IOM) recently reported that the global burden of cardiovascular disease was also high, and constituted a major health threat in developing countries [Institute of Medicine, 2010]. Americans have the highest BMIs, but other countries are catching up [Popkin, 2010]. The World Heart Federation endorsed the recommendations from the IOM, with the Chair of the Report Committee, Valentin Fuster, MD, commenting that the goals were difficult, but attainable. Heart disease has been the leading cause of death in the UK, but in two countries with traditionally low levels of risk factors, Greece and China, stable indigenous diets and high levels of physical activity have been replaced by Western fare and sedentary lifestyles, producing a corresponding rise in obesity, diabetes, hypertension, and CAD [Moran et al. 2010; Panagiotakos et al. 2008; Gu et al. 2005]. In fact, some Chinese children now have a higher BMI than Americans at the same age [Popkin, 2010].
The evidence supporting prevention is substantial and compelling
Seventeen years ago, McGinnis and Foege, seeking the root causes of disease, reported that half the deaths in the USA were premature, and could be prevented or significantly postponed by improving 10 modifiable behaviors, habits, and factors [McGinnis and Foege, 1993]. Among them, tobacco use, diet, and lack of sufficient physical activity continue to be major determinants of chronic disease and premature death. Since their observations, a number of large studies have confirmed that improvement in just a few behaviors will result in major changes in risk factors to enhance health outcomes. Many are observational and prospective, but within subgroups of behaviors and factors, there are also some available randomized, controlled studies. In addition, they also show the remarkably small number (5–9%) of individuals that actually follow multiple healthy behaviors. The question is then, not whether lifestyle changes are effective in lowering risk for chronic disease, or benefits are sufficiently substantial, but how to have people choose health and create an environment in which improvements will be realized. The cumulative effect of these reports, with singular concordance, is so striking that it is both instructive and motivating to review a selection.
Beginning in 1986, the Health Professionals Follow-up Study at the Harvard School of Public Health monitored 42,847 men who did not smoke, maintained a BMI of <25 kg/m2, engaged in moderate-to-vigorous activity ≥30 min/day, kept alcohol consumption moderate (5–30 g/day), and followed a healthy diet scored according to a healthy eating index established by the USDA [Chiuve et al. 2006]. After 16 years, men who followed all five practices enjoyed an 87% lower risk for cardiac events, and those who adopted two or more of them experienced a 27% reduction in cardiac events. Over half of the instances of CAD among those using risk-lowering drugs could have been avoided by adding healthy habits to the medications. The results were similar to those of the earlier Nurses’ Health Study [Stampfer et al. 2000], and showed the impressive extent to which lifestyle may enhance primary and secondary prevention in middle-aged men. Only 4% of all men in the study actually followed the five healthy practices, even though they were educated health professionals.
The EPIC-Norfolk Prospective Population Study followed 20,244 men and women in the UK for an average of 11 years to assess how four simple health habits affected mortality [Khaw et al. 2008]. The habits were not smoking, participation in either recreational or occupational physical activity, drinking moderately (1–14 shots/week, or the equivalent in beer or wine), and consuming at least five servings of fruits or vegetables daily, assessed by a vitamin C level of >5 mmol/l. After adjustment for age, sex, BMI, and social class, relative risks for all-cause mortality in those who followed 1, 2, 3, or all 4 habits were 1.39, 1.95, 2.52, and 4.04, respectively. The mortality risk benefit for those who adhered to four healthy habits was equivalent to being 14 years younger in chronological age.
The results of this report were confirmed in the UK Health and Lifestyle Survey [Kvaavik et al. 2010], during which a cohort of 4886 British subjects was followed for 20 years. The four health behaviors of interest were smoking, consumption of fewer than three servings of fruits and vegetables/day, fewer than 2 h of physical activity/week, and alcohol intemperance. In this study, the mortality risk benefit associated with adherence to all four healthy habits was equivalent to 12 years of aging.
The Potsdam Study used data from 23,153 German citizens [Ford et al. 2009]. The four variables of interest were tobacco use, a BMI less than 30 kg/m2, physical activity equal to or greater than 3.5 h/week or more, and a high intake of fruits, vegetables, whole grain bread, and low meat consumption. Participants were followed for a mean period of 7.8 years for the defined endpoints of diabetes, myocardial infarction, stroke, and cancer. Those individuals with all four healthy behaviors had a 78% lower risk of developing the four diseases. Specifically, risk of diabetes fell by 93%, heart disease by 81%, stroke by 50%, and cancer by 36%. Adherence to just one healthy behavior halved the risk of chronic disease. However, if a higher intake of vitamin D and calcium was added to the variables, according to a second release, cancer risk was reduced by over 60%.
Heidemann and colleagues prospectively evaluated the relationship between dietary patterns and risk of cardiovascular disease, cancer, and all-cause mortality [Heidemann et al. 2008]. The group followed 121,700 healthy women in the Nurses’ Health Study from 1984 to 2002, with five validated quantitative food frequency questionnaires completed during that period. Two predominant patterns of eating were identified. The ‘Western’ pattern consisted of higher amounts of red and processed meat, refined carbohydrates, French fries, sweets, and desserts. The ‘prudent’ pattern consisted of higher amounts of fruits and vegetables, legumes, poultry, fish, and whole grains. After 18 years, comparing the highest with the lowest quintiles of prudent diet scores, there was a 28% lower risk of cardiovascular mortality, and 17% lower risk of all-cause mortality, in women adhering to the prudent diet pattern. Parenthetically, there was also a 16% greater cancer mortality and 31% higher noncancer mortality in those following the Western diet pattern. Although an observational study, the number of participants and simplicity of using two patterns of food consumption related to mortality rather than to biomarkers or other surrogates distinguish the results.
Using a sophisticated mathematical model called Archimedes and data from the National Health and Nutrition Education Survey IV, the possible effects of recommended prevention activities on cardiovascular morbidity and mortality in the USA were examined [Kahn et al. 2008]. Among the 11 interventions probed were some that related to primordial prevention, and others to primary and secondary prevention, including use of aspirin and reductions in LDL, glycated hemoglobin (HbA1c), fasting blood glucose levels, weight, and smoking. The model found that 78% of adults are candidates for at least one prevention activity. If everyone received all the preventive maneuvers for which they are eligible, acute myocardial infarctions (AMI) and stroke would be lowered by 63% and 31%, respectively, graded according to the extent of success for each measure. There would be about 244 million quality-adjusted life-years added to the US adult population over 30 years, amounting to an average of 3.1 years of extended life for all adults if such measures were realized. The most intriguing feature was that it would take treatment of only five individuals to prevent one MI over a period of 30 years. Essentially an extension of the current paradigm of care without primordial prevention, smoking cessation, weight control, and aspirin in high-risk patients were found to be relatively cost-effective.
The INTERHEART study [Yusuf et al. 2004] conducted a case–control study of AMI in 52 countries with 12,461 participants and 9459 controls. Investigators sought to relate smoking, history of hypertension or diabetes, waist/hip ratio, vegetable and fruit intake, physical activity, consumption of alcohol, blood apolipoproteins (Apo B/Apo A-1), and psychosocial factors to myocardial infarction.
Risk factors, odds ratios and population-attributable risks of nine determinants of acute myocardial infarctions [Yusuf et al. 2004].
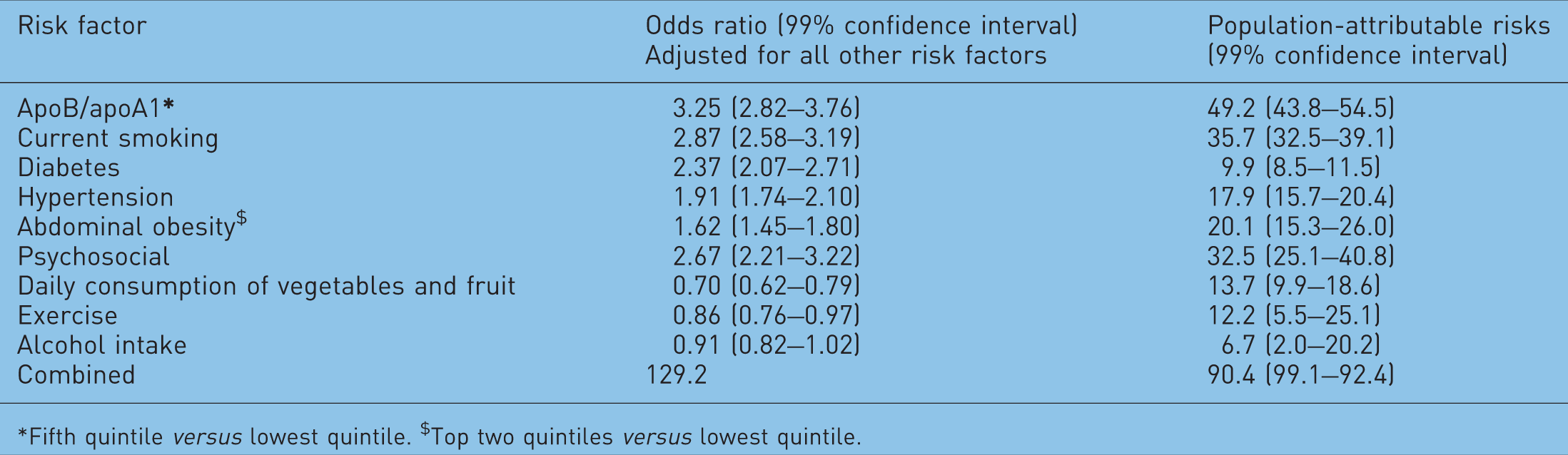
*Fifth quintile versus lowest quintile. $Top two quintiles versus lowest quintile.
Using data from the Estrogen Replacement and Atherosclerosis Study, Imamura and colleagues reported that adherence to the 2005 Dietary Guidelines for Americans reduced progression of CAD in women [Imamura et al. 2009]. These investigators devised a new method of weighing adherence to 20 key recommendations and found that close adherence to advice about intake of whole grains, lower total fat, and cholesterol management was related to changes in coronary atherosclerosis, as judged by blinded measures of quantitative coronary angiography over a 3-year period. Of interest: no woman followed all of the guidelines.
Kant and colleagues studied the association of a summary index of food consumption behaviors reflecting prevailing dietary advice and subsequent mortality [Kant et al. 2009]. Using data from the NIH-AARP cohort involving 350,886 participants, consumption of fruits and vegetables, low-fat dairy, whole grains, lean meat and poultry, and fat was found to be related to mortality from CAD, cancer, and all causes. Comparing the quintiles with the most favorable index and the most unfavorable, the former was associated with a 20–25% lower risk of mortality after 10 years of follow up.
Capewell and colleagues calculated how much CAD mortality would fall between years 2000 and 2010 if the Healthy People 2010 cardiovascular risk factors [Department of Health and Human Services, 2000] were achieved [Capewell et al. 2010]. Their unique CAD mortality model predicted that if risk factor trends continued from 2000 unchanged, 19,000 fewer deaths would have occurred. Details revealed that improvements in total cholesterol, blood pressure, smoking, and physical activity would predict 51,000 fewer deaths, but increases in obesity and diabetes would result in 32,000 additional deaths, leaving the net change less than anticipated. Their model also predicted that if the Healthy People 2010 cardiovascular risk factor goals were met, about 372,000 deaths would be prevented, nearly halving CAD death rates. Given current trends, however, Healthy People 2010 goals, as far as pediatric and adult obesity are concerned, will remain unreachable for decades to come, if at all [Kumanyika et al. 2008]. In fact, the latest interim data from Healthy People 2010 as of October 2010 show continuing lack of progress in achieving target goals in weight, physical activity, diabetes prevention, consumption of vegetables and fruits, prevalence of smoking, and (over)consumption of dietary salt, even using the older 2400 mg/day limit.
The suggested conclusion is that the ‘diabesity’ epidemic is offsetting any cumulative progress made by reducing other risk factors. Since the prevalence of obesity and diabetes is rising faster than other risk factors can be lowered by improving other lifestyle measures and using pharmaceuticals, these data create a realistic urgency about addressing and solving this dilemma.
Lifestyle changes leading to risk-factor reductions are associated with outcome improvements in cardiovascular diseases other than CAD. A cohort of 83,882 normotensive women in the Nurse’s Health Study followed for 14 years found that a healthy lifestyle may lower the incidence of hypertension by 80% [Forman et al. 2009]. The BMI was the most powerful predictor of hypertension. Data analyzed from 20,900 men in the Physicians’ Health Study followed for 22.4 years linked healthy behaviors with a significantly lower lifetime risk of health failure (HF) [Djousse et al. 2009]. For two of these risk factors, again in the Physicians’ Health Study, BMI and vigorous physical activity were strongly associated with protection against heart failure [Kenchaiah et al. 2009]. Risk of HF rose by 180% in men with BMI ≥30 (obese), and 49% in men who were overweight (BMI 25–30). For every additional 3.2 kg of weight on a man 177.8 cm tall, his risk for HF rose by 11%. Those who exercised vigorously 1–3 times a month lowered their HF risk by 18%, and those who exercised vigorously 5–7 days per week lowered their risk by 36%. Risk of HF for a sedentary obese man was 293% higher than for a man who was lean and exercising maximally.
An analysis of data from the Health Professionals Follow-up Study and the Nurses’ Health Study, involving 114,928 men and women, noted that physical activity, a prudent diet, and modest alcohol intake could lower the incidence of a first stroke up to 80%, with the reduction graded according to the level of adherence to the five healthy behaviors [Chiuve et al. 2008]. The conclusions strongly supported the American Stroke Association/AHA recommendations for the primary prevention of stroke.
The Dietary Intervention Randomized Controlled Trial (DIRECT) study randomized 140 middle-aged men and women to low-fat, Mediterranean, or low-carbohydrate diets for 2 years [Shai et al. 2010]. Some patients were taking antihypertensive and antilipidemic medications. After 2 years, carotid artery intima-media thickness and carotid vessel wall volume were assessed. The 5% of participants who exhibited carotid vessel wall volume regression also demonstrated a greater amount of weight loss, lower systolic blood pressure, and serum homocysteine levels, with higher apolipoprotein A-1 values. All three diets were equally effective in changing weight, blood pressure, and carotid measurements. Multivariate regression models showed only the lowered systolic pressure remained a predictor of carotid disease regression. The authors believed that a weight-loss-induced fall in blood pressure was primarily responsible.
A revealing recent report examined the adherence to behavioral recommendations about diet, exercise, and smoking after an acute coronary syndrome [Chow et al. 2010]. The study population comprised 18,809 patients participating in the Organization to Assess Strategies in Acute Ischemic Syndrome (OASIS 5) randomized clinical trial. At the 30-day follow-up visit, patients’ adherence to diet, exercise, and smoking were catalogued, along with conventional evidence-based management. Myocardial infarction, stroke, cardiovascular death, and all-cause mortality were documented 6 months thereafter. Quitting smoking versus continuing was associated with a decreased risk of AMI (odds ratio, 0.57). The odds ratio was 0.52 for adhering to diet and exercise versus not adhering and subsequent AMI. Patients who continued to smoke and did not follow a prudent diet or exercise had a 3.8-fold higher incidence of AMI-stroke-death, compared with those who never smoked, and followed diet and exercise recommendations. The short span of this study was, in contrast with others, a strength because it showed that the supplementation of usual pharmacological intervention with lifestyle changes effects a significant and rapid influence upon outcomes following acute coronary events. Of note: one-third of smokers refused to quit, 29% of participants ignored diet and exercise completely, but high adherence to pharmaceuticals (antiplatelet therapy, statins, and renin–angiotensin system blockers) was reported. The accompanying editorial [Patel and Balady, 2010] referred to the failure to reduce smoking and improve diet/exercise adherence as ‘a glaring demonstration of the current ineffectiveness of our healthcare system to enact these beneficial changes’.
In comparing the results of the benefits of lifestyle changes with procedures, Ornish stresses that often PCI with stenting does not prevent AMIs nor significantly prolong life in stable obstructive coronary disease [Ornish, 2009]. Indeed, it is a common misconception that PCI/drug-eluting stents lower the risk for AMI in patients with stable angina, or improve mortality, although other benefits are usually substantial [Kones 2010a, 2010b; Maron et al. 2010; Boden et al. 2007]. Intensive lifestyle changes may, however, achieve equal or better reductions in angina than revascularization procedures under certain conditions [Ornish et al. 1998, 1990; Ornish, 1998].
Residual risk remains a major concern
Particular risk factors and biomarkers treated as diseases themselves only reflect a portion of the total risk. Therefore while each risk factor is reduced during treatment, one must also be aware that unaddressed residual risk usually persists. Use of surrogates may create misleading confidence, since their response to therapy might differ from hard endpoints, such as reduction in the incidence of myocardial infarction or survival. The reduction in risk, and the extent of residual risk, may also vary with the therapeutic agent. A well-known example is the significant residual risk for cardiovascular events following guideline-directed reductions in LDL using statin drugs [Baigent et al. 2005; Libby, 2005]. In untreated Americans, the average adult LDL level is about 7 mmol/l; half the number of people in populations with LDL levels of about 6 mmol/l, considered ‘normal’ in current lipid profiles, will have atherosclerosis by the age of 50 years [Jaffer et al. 2002]. There is a well-established linear relationship between LDL-lowering and reduction in cardiac events. While traditional statins are efficacious in lowering LDL by about 30%, approximately 70% of cardiac events will unfold despite evidence-based therapy, i.e., are not prevented. Rosuvastatin in higher doses may improve both figures, but considerable residual risk is still a problem [Ridker et al. 2008]. In the PROVE-IT trial, aggressive lipid-lowering targeting LDL prevented just one in five cardiac events [Cannon et al. 2004]. Using intravascular ultrasound, it has recently been found that in about 20% of patients who achieved intensive targets, with an average LDL of 3.2 mmol/l, plaque volume still increased [Bayturan et al. 2010]. Residual risk arises in part from atherogenic lipid abnormalities other than LDL, particularly components of non-high-density lipoproteins (nonHDL), including excessive levels of very low-density lipoprotein (VLDL), chylomicron, and VLDL remnants, and sometimes lipoprotein (a). Low amounts, or poor quality, of HDL, and high triglyceride levels, also contribute to residual risk. Only a portion of this risk is captured by enhancement, using nonHDL cholesterol, apolipoprotein B, LDL particle number, or C-reactive protein (CRP) levels during evaluation. For this reason, raising HDL and/or modulating HDL function, and dual targeting of both LDL and CRP elevations, continue to attract attention as a means of closing the residual ‘risk gap’ [Alla et al. 2010; Natarajan et al. 2010; Kones, 2009; Ridker et al. 2008]. It should be noted that variations in lipid-rich particles and HDL by no means explains all of residual risk. Nonlipid factors obviously influence residual risk, giving rise to the imperative of targeting multiple risk factors. For instance, residual risk is especially high in diabetics, and recent partial failures to change cardiovascular outcomes in this disease by lowering glucose [The NAVIGATOR Study Group, 2010a], blood pressure [The NAVIGATOR Study Group, 2010b] or combination lipid therapy [Nilsson, 2010; The ACCORD Study Group, 2010], reaffirm the early, complex molecular pathology that impedes more complete protection within the timeframe of the studies conducted. Interestingly, these observations have taken us full circle, back to lifestyle, weight control and exercise as the more fundamental targets in diabetes risk management, which was found to be more effective than metformin in the Diabetes Prevention Program study [Diabetes Prevention Program Research Group, 2009]. Indeed, most antidiabetes and cholesterol-lowering drugs are clearly indicated as an adjunct to diet and exercise.
Limitations of intervention in high-risk patients
Owing to limitations in risk stratification and discrimination, many individuals who will go on to suffer cardiac events cannot be identified. Presently some are missed and misclassified by current algorithms [Berger et al. 2010; Kuller 2010; Marma et al. 2010; Cooney et al. 2009; Johnson et al. 2009; Tzoulaki et al. 2009; Wilson, 2009b; Ridker et al. 2007; Persell et al. 2006; Vasan et al. 2005]. Individuals may have a high lifetime risk of an event, yet score <10% on a 10-year risk estimate, simply because of the parameters chosen when the algorithms were devised [Berry et al. 2007; Lloyd-Jones et al. 2006]. The Framingham Risk Score (FRS), for instance, classically considered to predict accurately in 69% of a multi-ethnic population, may predict incorrectly in up to 85% of men and 33% of women, in whom risk is significantly underpredicted, for a combined prediction failure rate of 37% [Feeman, 2010]. FRS performance varies between populations and venues, leading to an overprediction by a factor of 2.87 in low-risk groups and underprediction of 0.43 in high-risk groups [Madhok and Fahey, 2006]. Since the incubation period of CAD extends over decades, using a 10-year timeframe is too short [Lloyd-Jones, 2010]. Using the 2003–2006 NHANES data, 56% of US adults have a low 10-year risk but a high lifetime risk for CAD [Marma et al. 2010]. Our inability to further refine risk prediction limits the future of the current model of identifying high-risk individuals for aggressive therapy. Add the significant residual risk that exists when patients are treated [Libby, 2005], and subtract the patients who are undiagnosed or undertreated, and the advantages of eliminating risk factors entirely through primordial prevention become more attractive. When blood glucose or LDL are lowered with drugs, neither the cause of the risk factor elevation nor the total outcome may be addressed, since the factor is only a surrogate, and not all pathogenetic pathways may be attenuated by those drugs. Individuals with cardiovascular health because of their lifestyles enjoy a higher level of ‘protection’ than patients whose risk factors are controlled pharmacologically.
In addition, an intervention such as PCI or coronary artery bypass grafts in high-risk patients may not be as successful as possible, because adherence to lifestyle changes and prescription drugs remains poor after the procedure. Unfortunately, 1 year after the initial diagnosis of CAD is made, diets in those patients remain unimproved [Ma et al. 2008]. After coronary artery bypass surgery, diets actually become even more atherogenic, despite formal counseling [Hartwell and Henry, 2003]. Enhancement of adherence in these instances will likely require a carefully designed case management system using specially trained nurses [Ciccone et al. 2010; Maron et al. 2010], or other delivery systems, such as pharmacist-managed lipid clinics [Gerrald et al. 2010; Kauffman et al. 2010].
Given the present progression of overweight, obesity, the metabolic syndrome, and cardiovascular risk, it appears questionable whether, using the present paradigm, even with improved efficiency of identifying individuals with high risk, more potent drugs, such as rosuvastatin, can be given to those who are so identified fast enough to reverse the onslaught. The recent approval for use of rosuvastatin in middle-aged patients with no clinical CAD, but with elevated CRP levels and one other risk factor, adds to the clinician’s armamentarium for primary prevention [Kones, 2009], but does not solve the fundamental cause. The enormity of the issue suggests, however, more is needed sooner, but, most assuredly, in addition to the proven traditional approach of treating high-risk individuals aggressively [Kones, 2010c, 2009].
Status of prevention performance
In all three categories, primordial prevention that does not permit risk factors to appear in healthy individuals, primary prevention focusing on lowering risk factors in patients yet to suffer a cardiovascular event, and secondary prevention to delay recurrent events, progress has been less than satisfactory. Even when pharmacological methods are used to reduce risk aggressively according to evidence-based protocols, as mentioned, around 70% of subsequent cardiac events still remain unaddressed.
Two additional practical barriers also prevent optimization of risk reduction, that is, poor patient adherence [Baroletti and Dell’Orfano, 2010; Muzzarelli et al. 2010; Ho et al. 2009; Mazzaglia et al. 2009; Osterberg and Blaschke, 2009; Jackevicius et al. 2002], and imperfect physician performance in monitoring and prescribing [Basile, 2010; Davidson et al. 2009; Gotto, 2009; Kotseva et al. 2009; McKenney et al. 2009; Sachdeva et al. 2009; Waters et al. 2009; Riesen et al. 2004], so that results in usual practice venues are not comparable to goals or to those in published studies. In clinical trials average patient adherence ranges from 43% to 78%, but data in practice reflect lower rates. Patients with CAD and stroke fail to fill their prescriptions within 1 week after discharge 23% of the time. Nonadherence is now a risk factor in itself [Cutler and Everett, 2010; Ho, 2009; McKenney et al. 2009; Ho et al. 2006; Yiannakopoulou et al. 2005; Grant et al. 2003], and may result from simple refusal, reluctance to take medications for life, lack of understanding, polypharmacy, cultural factors, or cost.
However, the patient is not the entire explanation [Sachdeva et al. 2009; Doroodchi et al. 2008; Erhardt, 2005; Hajjar and Kotchen, 2003]. In one notable report, only 29% of patients with a prior history of CAD were taking lipid-lowering drugs upon hospital admission, presumably in greater part because they were not given prescriptions [Sachdeva et al. 2009]. NHANES III data reported only 7% control in dyslipidemia patients, with 16% given lipid-lowering medication [Fryar et al. 2010]. Of those with both hypertension and dyslipidemia, fewer than 3.6% of patients achieved dual targets. The DYSlipidemia International Study (DYSIS) recently reported that 37% of all patients being treated with statins in Canada failed to reach Canadian guideline goals, including 45% of high-risk patients [Goodman et al. 2010]. Only 10–15% of patients reach aggressive LDL targets ≤4 mmol/l [Kauffman et al. 2010]. Indeed, although the numbers are improving, as many as 30–65% of all patients do not achieve evidence-based target goals in three risk factor categories, that is, blood pressure, dyslipidemia, or glucose/HbA1c. Moreover, while fewer than 50% of patients with both hypertension and dyslipidemia reach goals, the treatment gap is even more pronounced among obese patients [Bhan et al. 2010].
As office blood pressures may be inaccurate and infrequent, and with home and ambulatory recordings still underutilized, hard data about deficiencies in reaching blood pressure targets are sparse. There have been indications of only 27% net control [Hyman and Pavlik, 2002], whereas with adequate monitoring and titration 69% may achieve goals [Cooper-DeHoff et al. 2004; Hajjar and Kotchen, 2003], leaving perhaps 20–30% of hypertension patients classified as resistant [Calhoun et al. 2008]. Use of questionnaires and surveys based upon recall are unreliable and may produce misleading data [Miller et al. 2010]. A recent analysis of partial data from 2007–2008 NHANES found that, while rates of hypertension rose from 23.9% in 1988–1994 to 28.5% in 1999–2000, they remained steady at 29% between 1999–2000 and 2007–2008. In addition, these investigators reported an improvement in hypertension control from around 35% in the NHANES data from 1999–2004 to 50.1% in the 2007–2008 update [Egan et al. 2010]. This encouraging improvement, however, still leaves half of known hypertensives uncontrolled. Several limitations in the study were also evident. Blood pressures less than 140/90 in diabetics were considered normal, and even though they were not being treated for hypertension, they were still counted as ‘controlled’. Similarly, even if fasting blood glucose was well over 7 mmol/l, individuals were not classified as diabetics, because ‘diabetes’ was defined by a history of treatment or having been told of the diagnosis. In addition, the startling rise in overweight and obese citizens from the 1999–2004 NHANES data to the present time has produced a corresponding rise in hypertension noted elsewhere, the same period during which hypertension control is reported to have improved 20%. The close relationship among the variables of age, BMI, visceral adiposity, insulin resistance, blood pressure, and even aldosterone secretion is well established [Garg et al. 2010; Schneider et al. 2010; Zalesin et al. 2008; Mufunda, 2007]. Since health habits, including departure from Dietary Approach to Stop Hypertension (DASH)-like diets and salt consumption, have significantly worsened during this same period, lifestyle improvements are an unlikely explanation for any improvement in blood pressure control. This leaves a precipitous rise in the number of medications dispensed to explain the reported rise in control, which could not be assessed because of lack of available data. An accompanying editorial cautioned that these results need confirmation, particularly whether hypertension prevalence has not changed since the 1999–2004 survey [Chobanian, 2010]. Resolution with other reports, and a most recent one discussing the disparity of more uncontrolled hypertension despite improved therapy, awaits further clarification [Fryar et al. 2010; Lloyd-Jones et al. 2010; Chobanian, 2009]. By all measures thus far, hypertension, a major risk factor for premature cardiovascular morbidity and mortality, remains poorly controlled in North America, the UK, and the EU [Leenen and Schiffrin, 2010].
Sometimes not included in risk factor discussions because its deleterious effects are largely, although not exclusively, mediated through blood pressure, dyslipidemia, and diabetes, the attainment of weight targets lags even further behind. Disparity between performance and goals, or the ‘quality chasm’, is sometimes attributed to delays in translation of prevention research, but the figures above refer to well-established guidelines [Zapka, 2008]. One might also compare this performance to guideline adherence in related areas, such as warfarin use at discharge for atrial fibrillation complicating acute coronary syndromes, with only 13.5% of patients so treated [Lopes et al. 2010]. When all of these shortfalls are considered together, there is a vast amount of incipient and ongoing cardiovascular pathology in the population that is currently unrecognized and undertreated.
Considering limitations in identifying high-risk individuals, appreciable levels of unaddressed residual risk, the significant fraction of patients not aggressively managed through ‘clinical inertia’, and disappointing adherence, it appears that presently, total risk during primary and secondary prevention is being reduced by a surprisingly small percentage.
Risk factors in EUROASPIRE I, II, and III.

In mmHg systolic/mmHg diastolic.
FBS, fasting serum glucose; TC, total serum cholesterol.
In EuroASPIRE III, about one third of patients with CAD had diabetes, and in those using pharmacological agents for control, only 10% had fasting glucose values ≤6.1 mmol/l; only two out of five reached targets for HbA1c in the primary prevention group. Among approximately 9000 patients, of those with hypertension taking drugs, only 44% were controlled, meaning nearly three out of five patients under active care did not reach goals. Since the number of prescriptions for all classes of agents increased significantly, the authors believed that the rising proportions of overweight and obese patients contributed to the dismal results, along with lack of uptitration of doses and poor adherence. Targets for total cholesterol were reached in only 55% of patients, but this number had risen consistently from study to study, which was attributed to the use of more potent statins. About 89% of patients were prescribed hypolipidemic drugs, and 97% were using antihypertensive medication in the latest survey, yet results remained substandard. About a fifth of patients with CAD continued to smoke cigarettes, but there was a rise in smoking in men and in numbers of women smoking, especially young women. The numbers of patients that were overweight or obese had gone up steadily from 1999. To place these results in perspective, one comprehensive lifestyle management system has achieved better percentages of reaching target goals without any medication in 3 months, achieving reductions in systolic pressure of 64%, diastolic pressure of 67%, LDL cholesterol of 21%, and fasting blood glucose of 39%, with somewhat different entry qualifications [Gordon et al. 2002].
A critical editorial particularly decried the gap between EuroASPIRE III results and current guidelines, commenting that one would expect physicians to be able to do a better job of reaching evidence-based targets in secondary prevention, compared with patients trying to adhere to lifestyle changes in primary prevention [Brekke and Gjelsvik, 2009]. Possibilities explaining the disparity included ongoing reluctance of physicians to intensify treatment with potential side effects and expense simply to compensate for persisting lifestyle deficiencies. Although targets should be reached, focus should continue on lifestyle issues, the editorial continued, adding that pharmacological secondary prevention was not enough, and political action was needed to reverse trends in obesity and lack of physical activity.
In a survey of primary care practitioners, only 33% considered evidence-based practice guidelines important in achieving optimum patient management [Hajjar and Kotchen, 2003]. One half indicated their knowledge of nutrition was a significant barrier in giving dietary advice, and over one third did not recommend lowering trans fatty acid intake in patients [Mosca et al. 2005]. Yet, dietary intervention is the foundation and the first step in the management of lipid disorders and coronary risk factors [Anderson, 2003; ATP Final Report, 2002]. In the EU, 10% of physicians are unaware of the guidelines, another 10% say there are too many, and many believe they are following the guidelines when they are not [ATP Final Report, 2002]. Compared with the FRS, physicians significantly underestimate risk [Hobbs and Erhardt, 2002]; 13% of primary care physicians routinely use a risk score, 43% do sometimes, and 43% rarely or never use one [Backlund et al. 2004]. While the FRS and/or SCORE may not be perfect, they are a considerable improvement over individual practitioner judgment. Hence, for both physicians and patients alike, perception and reality remain far apart as far as risk burden, adherence, and outcomes are concerned [Erhardt, 2005; Erhardt and Hobbs, 2002].
The use of a ‘polypill’ containing ramipril, simvastatin, and aspirin, or a ‘polycap’, containing additional atenolol and a thiazide, has been the subject of much debate [Wald and Wald, 2010; Cannon, 2009; Fuster, 2009; Robinson, 2009; Yusuf et al. 2009; Fuster and Sanz, 2007]. Given to large portions of the population, such a pill is expected to lower ischemic heart disease burdens by over 80%, roughly equivalent to the results of a stringent lifestyle and closely followed risk factor reduction program. Worldwide, several clinical trials using polypills are in progress or poised to begin. This approach, although an embarrassing social commentary, is supported by many authorities who consider the poor rate of primordial prevention (0.5–5%), low adherence to prescribed therapies (<50%), poor compliance with lifestyle prescriptions (<15%), and disappointing control of multiple risk factors in the same patient (5–10%) essentially unchangeable.
Conclusion
CAD begins in childhood, has an incubation period extending over decades, and is a diffuse, systemic disease that results from multiple common factors. While the present paradigm of care has decreased deaths from heart disease and is effective, the obesity epidemic threatens to reverse recent gains.
Despite current screening, preventive measures, and therapies, a surprisingly high amount of cardiovascular risk remains uncharacterized and untreated in the general population. Obesity, diabetes, and cardiovascular disease are eminently preventable, and lifestyle optimization has the advantage of reducing several risk factors simultaneously. As a result, primordial prevention to prevent risk factors from appearing in the first place is a concept with much potential, and could complement primary and secondary prevention, as well as specific intensive treatment in high-risk individuals.
Such an approach would involve motivational reorientation of the public, emphasizing personal responsibility and pride in achieving goals. Re-education might revolve around a message that ideal cardiovascular health is much more than crisis intervention, and beneficial habits must begin early and continue throughout life, in addition to other therapies, including revascularization. Unfortunately, the continuing trend has been to shift individual responsibility for unhealthy habits entirely to the medical profession, rather than accept personal ownership. As a result, preventive cardiologists are under increasing pressure to optimize risk reduction strategies pharmacologically. Likewise, even poor adherence performance is now considered a failure of the medical system rather than a conscious patient choice. In contrast, behavioral health data suggest that indifferent and unreceptive patients will prevent the success of otherwise meritorious health management programs (Adams, 2010).
A population-wide effort of unparalleled proportions, major alterations in food industry practices, and significant social and environmental adjustments will be necessary to stem the current epidemics of obesity, diabetes, and CAD [Doroodchi et al. 2008]. The importance of including our youth in efforts to re-educate cannot be overemphasized, since risk factors are present in children as young as 4 years of age [Corvalán et al. 2010; Fuster, 2010].
Across the continents, evidence mounts emphasizing the perils of rising risk, while recent reports continue to reflect urgency. Therefore, in the face of overwhelming data that prevention trumps treatment in all respects, continued inattention and inaction appear unwise and potentially disastrous.
Is an ounce of prevention worth a pound of cure? The evidence says the answer is yes, if one selects the prevention, targets the cure and does what needs to be done.
Footnotes
Acknowledgement
The author wishes to thank Michelle Delaney for her astuteness, computer skills, untiring assistance, and valuable suggestions in the preparation of this manuscript.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
None declared.