
Abstract
Background
With the emergence of the coronavirus 2019 (COVID-19) pandemic, it was essential to determine the impact of this disease on pregnant women and neonatal outcomes. In this study, we present a series of nine cases of pregnant women with COVID-19 disease requiring intensive care unit (ICU) admission.
Methods
We retrospectively collected clinical data of pregnant women with COVID-19 disease admitted to ICU between September 2020 and September 2021.
Results
Most common presenting symptom was cough. Two patients had no respiratory symptoms at presentation. Five of the nine patients required invasive mechanical ventilation. Seven patients required caesarean section, four of whom delivered preterm. There were no maternal or neonatal deaths.
Conclusions
Although maternal and neonatal outcomes reported in our study are encouraging, it is imperative to emphasize the importance of an individualized, multidisciplinary approach, and good healthcare infrastructure for optimal management of this group of patients.
Keywords
Introduction
Towards the end of the year 2019, the world witnessed the beginning of the pandemic of COVID-19, first reported in Wuhan, China.1,2 Pregnant women were believed to be at a higher risk of developing a complex clinical course of the disease owing to the altered immunity of pregnancy. This concern stemmed from pregnant women's vulnerability to developing a severe infection from influenza and the associated poor neonatal outcomes. 3 Also, the outcomes of Middle East respiratory syndrome (MERS)-CoV and severe acute respiratory syndrome (SARS)-CoV infection in pregnant women were not encouraging albeit the data is scanty.4,5 Early reports from China and other places suggested an encouraging clinical course and prognosis for COVID-19 in pregnancy, however, some reports suggested otherwise.6–13 The U.S. Centers for Disease Control and prevention reported, in the early part of the pandemic, that pregnant women were at a higher risk for intensive care unit (ICU) admission and mechanical ventilation. This was further reiterated in their updated report, in addition to stating that they are at an increased risk for requiring extracorporeal membrane oxygenation and mortality.14,15 Subsequently multiple meta-analyses and systematic reviews found an increased incidence of preterm delivery, caesarean section (CS), and maternal mortality.10,16–18
Pregnancy-induced physiological changes elevate the risk of developing hypoxemia with SARS-CoV-2 infection in these patients. Although the changes in the immune system during pregnancy can alter the response to an infection, the outcomes may not be generalized. 19 This case series of nine pregnant women admitted to the ICU of our quaternary care centre in South India highlights the diverse presentation of COVID-19 infection complicating pregnancy and related disorders with other medical and surgical conditions, necessitating a tailored approach towards management for better outcomes.
Methods
This is a retrospective case series of pregnant women with COVID-19 requiring ICU admission, from a single quaternary care centre between September 2020 and September 2021. All patients tested positive for COVID-19 pneumonia by reverse transcription-polymerase chain reaction (RT-PCR). After obtaining informed written consent, we reviewed the characteristics of these patients from our electronic database and telephone follow-up post-discharge, including symptoms, clinical course, laboratory parameters, comorbidities, length of ICU and hospital stay, and maternal and neonatal outcomes. Ethics committee waived approval.
Results
During the study period, a total of nine pregnant women with COVID-19 infection required ICU admission. This study period had India witness both the first and the second COVID-19 waves during which the predominant variants were B.1.36 (pango lineage) and B.1.617.2 (Delta) variants, respectively. 20 The mean maternal age was 33.8 (range 21–42) years. The most common presenting symptom was cough followed by fever and breathlessness. Two patients who were hospitalized did not have symptoms of COVID-19 (Table 1). One of them was diagnosed to have HELLP and underwent emergency CS for the same while the other patient was admitted with subacute intestinal obstruction which was managed conservatively. The latter initially tested negative for COVID-19, but eventually acquired the infection a week later requiring invasive mechanical ventilation (IMV) and emergency CS. Seven of the nine patients underwent CS, five of which were performed after admission to our institute. Four of these patients delivered preterm with their neonates requiring ICU care and one among them delivered a twin. Five patients required IMV for acute respiratory distress syndrome (ARDS) using lung protective strategy with low tidal volume and high respiratory rate with positive end expiratory pressure and fractional inspired oxygen (FiO2) titrated to prevent hypoxia and atelectasis. Three of these patients required prone ventilation. As per our institution policy at the time, based on the clinical assessment by the multidisciplinary team consisting of intensivist, neonatologist, obstetrician and anaesthesiologist, pregnant women of more than 28 weeks’ gestation with P/F (arterial oxygen partial pressure to fraction of inspired oxygen) ratio less than 150 requiring prone ventilation were considered for CS while rest of the treatment strategy remained same as for non-pregnant. Two patients developed cardiomyopathy, of whom one had peripartum cardiomyopathy while the other developed likely COVID-19-related cardiomyopathy, and both showed clinical resolution at discharge. The former was discharged on hospital day (HD) 8 while the latter was discharged on HD 11. Four patients developed secondary sepsis which responded to treatment. There were no maternal or neonatal deaths (Table 2).
Characteristics of the population and laboratory investigations.
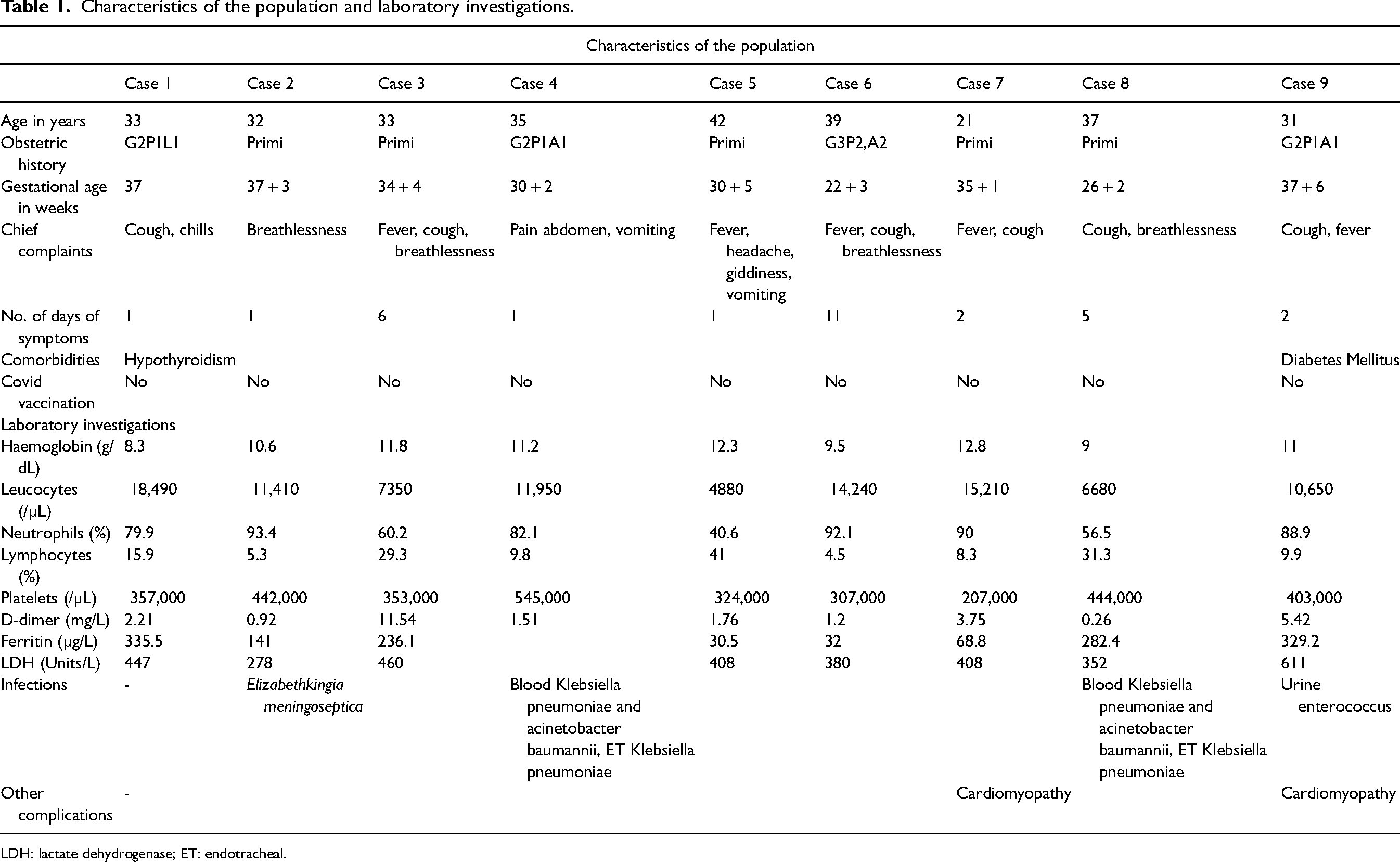
LDH: lactate dehydrogenase; ET: endotracheal.
Treatment and outcome.
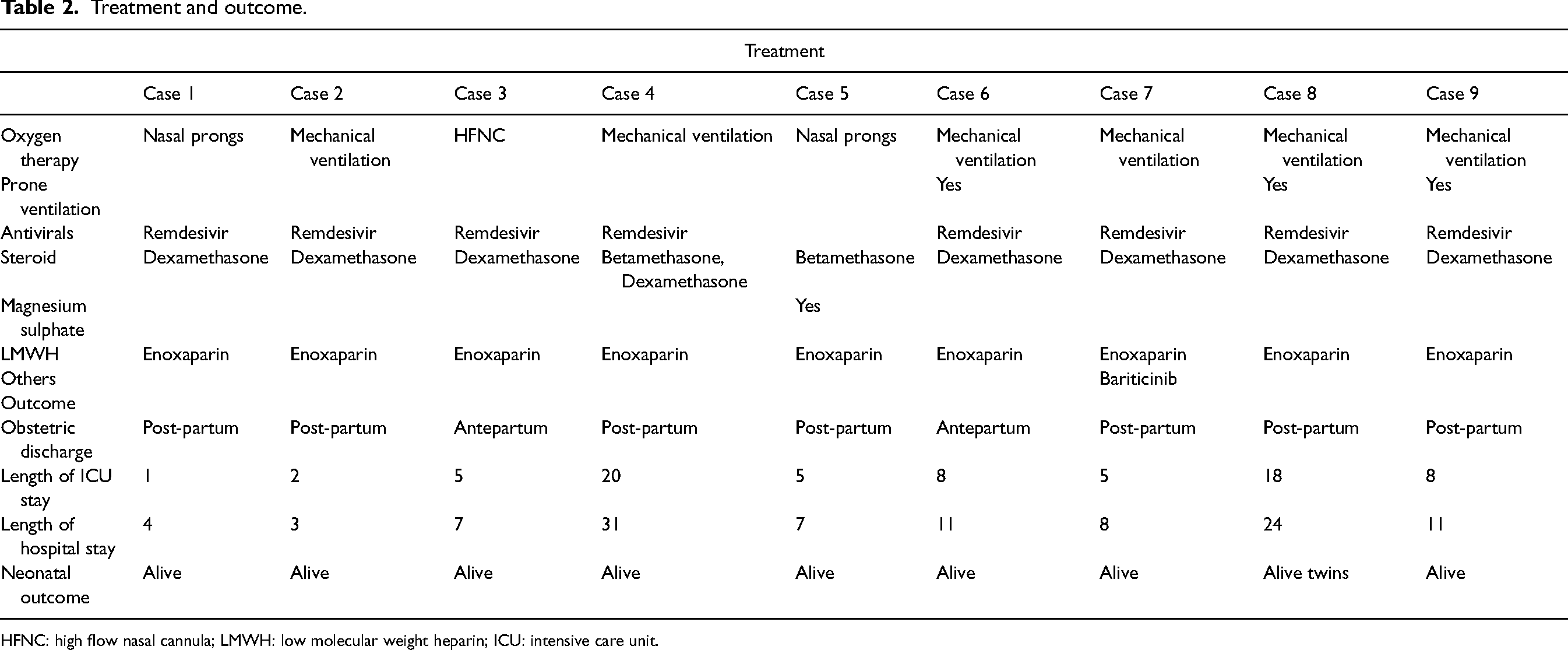
HFNC: high flow nasal cannula; LMWH: low molecular weight heparin; ICU: intensive care unit.
Case 1
A 33-year-old woman in her third pregnancy, had a history of hypothyroidism and presented at 37 weeks of gestation with cough and chills for 1 day. At presentation, she was mildly tachypneic with an oxygen saturation (SpO2) of 96% on room air (RA) requiring oxygen supplementation via nasal prongs. Lab investigation revealed an elevated leukocyte count. Inflammatory markers were mildly elevated. She underwent CS on the same evening as the gestation reached term and in anticipation of the progression of COVID-19 disease. She delivered a healthy male baby. Following CS, she was initiated on remdesivir, empirical antibiotics, dexamethasone, enoxaparin, and minimal oxygen supplementation. After a day in the ICU, she was transferred to the ward and discharged home on HD-4.
Case 2
A 32-year-old woman, who underwent CS 10 days earlier at 37 weeks and 3 days of gestation, tested positive for COVID-19 three days following CS when she presented with a history of breathlessness for 1 day. At presentation, she was in respiratory distress requiring IMV. Her worst P/F ratio was 212. She was initiated on empirical antibiotics, dexamethasone, remdesivir, and anticoagulants. Chest X-ray revealed bilateral diffuse infiltrates. Blood investigation was remarkable for elevated inflammatory markers. Antibiotics were rationalized based on the blood culture which grew Elizabethkingia meningoseptica. She was liberated from the ventilator after 24 h. She was transferred out of ICU on HD-2 and discharged home on HD-3 with down-trending inflammatory markers and clinical stability. On follow-up, we learned that the female baby was healthy while the mother succumbed to myocardial infarction 4 months later.
Case 3
A 33-year-old woman in her first pregnancy presented at weeks and 4 days of gestation with a history of fever and cough for 6 days and worsening breathlessness for 3 days. At presentation, she was tachypneic and hypoxic (SpO2 89% on RA) requiring oxygen supplementation via non-rebreathing mask (NRBM). Within 24 h, hypoxia worsened requiring high-flow nasal cannulae (HFNC). She received remdesivir, anticoagulant, and dexamethasone for fetal lung maturity in anticipation of emergency CS with worsening maternal oxygenation. Her inflammatory markers were mildly elevated. On day 3 of ICU, she developed itching with an elevation of bile acids. A diagnosis of intrahepatic cholestasis of pregnancy was made. She responded to treatment with ursodeoxycholic acid. With stability in her respiratory parameters, she was weaned off oxygen and transferred out of ICU on HD 5. She was discharged home on HD 7. She continued her regular outpatient reviews and delivered a female baby weeks later.
Case 4
A 35-year-old woman in her first ongoing pregnancy presented at 30 weeks and 2 days of gestation with a history of abdominal pain and vomiting for 1 day. She was initially evaluated in another hospital where abdominal ultrasound revealed moderate ascites and pleural effusion. She was transferred to our hospital on the same day for further management. On arrival, she was found to be hypotensive, tachycardic, and tachypneic with blood gas demonstrating a metabolic acidosis with hyperlactatemia. She was fluid resuscitated and initiated on vasopressors and broad-spectrum antibiotics. She tested negative for COVID-19. Magnetic resonance imaging of abdomen and pelvis revealed features suggestive of subacute intestinal obstruction. After consultation with general surgeon, she was managed conservatively. Betamethasone was administered for fetal lung maturity. Over the next 24 h, she improved symptomatically, opened her bowels, and became hemodynamically stable. She was then transferred to the ward after 3 days in the ICU.
On HD-8, she developed respiratory distress with hypoxia (SpO2 89% on RA) requiring oxygen supplementation. Deep vein thrombosis was ruled out. Repeat RT-PCR for COVID-19 returned positive. She was moved to the ICU and initiated oxygen supplementation, dexamethasone (COVID-19 dose), and anticoagulants. Her oxygenation worsened requiring HFNC and eventually IMV. She underwent emergency CS, in view of maternal hypoxemia (P/F 151.6) and delivered a live female baby. She was then initiated on remdesivir. Over the next 24–48 h, her oxygenation improved, sedation and paralytics were stopped, and weaning attempts were made.
On HD-16, her chest X-ray revealed pneumomediastinum for which bilateral intercostal drain (ICD) was inserted. Her hemodynamics worsened over the next 48 h warranting antibiotic escalation. Repeated blood culture grew Acinetobacter baumanii and endotracheal aspirate culture grew Klebsiella pneumoniae. Contrast-enhanced computed tomography (CT) abdomen revealed nothing contributory. Her clinical condition gradually improved and on HD-21, she underwent tracheostomy in view of difficult weaning. Both the ICDs were removed and she was weaned off the ventilator over the next 72 h. She was transferred out of the ICU on HD-24. She was decannulated after ten days following tracheostomy. She remained clinically stable and was discharged home on HD-31.
Case 5
A 42-year-old woman in her first pregnancy presented at 30 weeks and 5 days of gestation with a history of headache, giddiness, fever, and vomiting for 1 day. She tested positive for COVID-19 at another medical facility and transferred to us for further management. At presentation, she was found to be hypertensive with bilateral pitting pedal oedema. Her oxygen levels were satisfactory. She was initiated on antihypertensives. She received betamethasone injections for fetal lung maturity. She was administered magnesium sulphate for seizure prophylaxis and fetal neuroprotection. Her lab investigations were remarkable for mildly elevated transaminases and down trending thrombocytopenia. On HD-3, she underwent emergency CS in view of partial HELLP syndrome and delivered a live male baby. After 2 days in the ICU, she was transferred to the ward and discharged home on HD-7.
Case 6
A 39-year-old woman in her third ongoing pregnancy presented at 22 weeks and 3 days of gestation with a 11 day history of fever, 7 day history of cough and 2 day history of breathlessness. She was initially managed in another healthcare facility where she tested positive for COVID-19 and subsequently transferred to our hospital. She was hypoxic (SpO2 89% on RA) on arrival and was initiated on oxygen via HFNC, empirical antibiotics, remdesivir, dexamethasone (COVID-19 dose), and anticoagulants. Fetal scan was unremarkable. Blood investigations revealed elevated inflammatory markers. Over the next 24 h, respiratory distress worsened requiring IMV. Her hypoxemia (P/F 148.33) became refractory warranting prone ventilation for the next 16 h, done with adequate precautions and, in consultation with the obstetrician. On day 4 of ICU, she became febrile requiring antibiotic escalation. Repeat cultures were sterile and antibiotics were de-escalated. She improved clinically and was liberated from the ventilator after 5 days. She was transferred out of the ICU on HD-9 and discharged home on HD-11. On follow-up, we learned that she delivered a full term male baby through CS.
Case 7
A 21-year-old woman in her first pregnancy presented at 35 weeks and 1 day of gestation in the 2nd week of her COVID-19 infection. She was initially admitted to another hospital with a history of fever, cough, and breathlessness for 2 days. Nine days following admission, she complained of chest pain, following which echocardiography revealed global hypokinesia with severe left ventricular (LV) dysfunction, grade III LV diastolic dysfunction, moderate to severe mitral regurgitation, and mild tricuspid regurgitation. Her troponin I levels were within normal limits while NT-proBNP was markedly elevated (14,257 pg/ml). She was referred to our hospital for further management.
After the initial evaluation and multidisciplinary meeting, it was decided that she would need an emergency CS. She underwent an emergency CS delivering a live male baby and was extubated on the table. In the ICU, she was initiated on remdesivir, baricitinib, cabergoline, anticoagulants, diuretics, sacubitril-valsartan, dexamethasone, antibiotics, and oxygen supplementation of 6 L/min via facemask (SpO2 100%). High-resolution computed tomography (HRCT) done on postoperative day 1 revealed multifocal diffuse nonsegmental ground glass opacification, consolidation with interstitial thickening seen in all lobes of both lungs with a CT severity index of 20/25. 21 Blood investigations were remarkable for elevated inflammatory markers. Echocardiography repeated after one week revealed findings similar to the previous study. Her further clinical course was uneventful with transfer to ward on HD-5 and discharge to home on HD-8.
Case 8
A 37-year-old woman in her first pregnancy (twin pregnancy) presented at 26 weeks and 2 days of gestation with a history of cough for 5 days and breathlessness for 3 days, and was admitted to another medical facility. She was treated for COVID-19 pneumonia with remdesivir, COVID-19 dose of dexamethasone, anticoagulants, and respiratory support with non-invasive ventilation (NIV). With worsening respiratory failure, she was transferred to our hospital for further care after 4 days. At presentation, she was in respiratory distress requiring IMV. We continued treatment with remdesivir, anticoagulants, dexamethasone (COVID-19 dose), and empiric antibiotics.
Hypoxia (P/F 123.3) remained refractory warranting prone ventilation. After a multidisciplinary meeting involving intensivists, obstetricians, and neonatologists, the family was explained the need for emergency bedside hysterotomy to facilitate prone ventilation and, regarding the care of the pre-term twin. On the same evening, she underwent an uneventful bedside emergency hysterotomy and delivered two live female babies. She was then prone ventilated for 18 h following which she improved clinically. Her initial blood culture grew Klebsiella pneumoniae and antibiotics were rationalized. She was gradually weaned and liberated from the ventilator after 1 week. However, she had an extubation failure requiring reintubation the same evening. Repeat blood culture grew Acinetobacter baumannii and tracheal culture grew Klebsiella pneumoniae. Antibiotics were tailored accordingly. She underwent tracheostomy the next day to facilitate weaning.
Over the next 10 days, she was weaned off the ventilator and transferred to the ward. She was decannulated after 14 days following tracheostomy. She was discharged home on HD-24. On follow-up, we learned that one of the female babies died after 6 weeks while the other baby is on antiepileptics.
Case 9
A 31-year-old woman in her second ongoing pregnancy, presented at 37 weeks and 6 days of gestation, to another hospital with a history of cough and fever for 2 days. Her past medical history was significant for diabetes mellitus. She underwent emergency CS the following day in anticipation of worsening COVID-19 disease and, delivered a live male baby. Two days following CS, she became hypoxic requiring oxygen supplementation via NRBM. HRCT revealed multiple patchy and confluent areas of ground glass opacities with interspersed areas of dense consolidation in the left lung and anterior segment of right upper lobe with a CT severity index of 7/25. She was treated with remdesivir, dexamethasone, and anticoagulant. After one week, her respiratory failure worsened and was transferred to our hospital for further management.
NIV was attempted but not adequate so she required IMV. She was treated with remdesivir, dexamethasone, anticoagulants, and diuretics. Echocardiography revealed global hypokinesia with mild LV systolic dysfunction and right ventricular dysfunction with mild pulmonary arterial hypertension. She remained hypoxic (P/F 118.33) requiring prone ventilation for 18 h. Her urine culture grew Enterococcus sp requiring tailoring of antibiotics. With improvement in her respiratory parameters, weaning trials were initiated after 4 days of ventilation and eventually extubated after 1 week of ventilation. Over the next 24 h, she remained stable and was transferred to the ward. She was discharged on HD-11.
Discussion
The management of pregnant women with COVID-19 requires an individualized approach owing to the risks to the maternal and fetal health posed by the physiological changes of pregnancy. The pregnant state leads to an increased oxygen demand as a result of increased metabolism but this may be compensated by an increase in the tidal volume. However, during the late phase of pregnancy, the gravid uterus splints the diaphragm by elevating it, which in turn reduces the functional residual capacity.22,23 This subset of the population is also predisposed to develop ARDS as a result of reduced albumin and increased capillary permeability. 24 Also, the profound inflammatory state generated by SARS-CoV-2 infection promotes thrombosis involving multiple mechanisms and has been associated with poor outcomes.25–27 This is further compounded by the hypercoagulable state of pregnancy, creating a prothrombotic milieu, and thus increasing the risk of thrombotic complications. 28
This case series shows the diverse presentation and challenges involved in the management of COVID-19 in pregnant women. Zohra et al., in their meta-analysis, involving 31,016 pregnant women with COVID-19, found cough and fever to be the most common presenting symptoms, with the risk of developing severe COVID-19 being higher in women who presented with fever, cough, shortness of breath, chest pain, myalgia, diarrhoea, and fatigue. 29 Villar et al. found that women with shortness of breath and fever were at higher risk of developing severe maternal and neonatal complications. 30 In the current series, most common presentation was cough and fever, with majority requiring mechanical ventilation. The risk factors for severe COVID-19 infection include women aged more than 35 years, smoking, pre-eclampsia, obesity, diabetes, and pre-existing cardiac and respiratory diseases. 29 One patient with diabetes mellitus developed severe disease requiring mechanical ventilation and prone ventilation but eventually recovered. Another patient, who was admitted primarily for management of HELLP, developed no significant respiratory manifestations of COVID-19 disease.
The role of HRCT in COVID-19 not only lies in its diagnostic ability but also in grading the severity. 31 Studies have found that CT of the chest shows features typical of COVID-19 with multiple ground glass opacities in more than 90% of this patient population.7,8,11 One patient in this case series had a higher CT severity score (20/25) but recovered without a stormy course while another patient who had a low CT severity score (7/25) worsened progressively to develop severe ARDS requiring IMV and prone ventilation.32,33 Favourable outcomes have been reported in pregnant women with COVID-19 disease developing cardiomyopathy.34–37 A retrospective observational study by Mercedes et al. observed 154 patients, of whom 15 developed myocardial dysfunction and 86% of these patients required mechanical ventilation, and 2 of them eventually died secondary to arrhythmias. 38 In the current series, of the two patients who developed cardiomyopathy, the patient with COVID-19-related cardiomyopathy required mechanical ventilation. Both patients responded to medical management leading to discharge from the hospital.
The INTERCOVID study, involving a total of 2130 patients from 18 different nations, found an increase in maternal morbidity and mortality in pregnant women with COVID-19 disease. They reported an increased risk of developing hypertensive disorders of pregnancy, infections, preterm birth, and consequently low birth weight. They demonstrated a 22-fold increase in maternal mortality in pregnant women with COVID-19 in under-developed regions suggesting the paucity of adequate healthcare infrastructure. 30 A subsequent meta-analysis further strengthened this evidence by demonstrating adverse maternal and fetal outcomes in pregnant women with COVID-19 disease. 18 Of the five patients who underwent CS at our institution, four patients delivered preterm by CS with their neonates requiring intensive care. Two of these preterm deliveries were in view of refractory hypoxemia with one patient warranting prone ventilation. Studies on the effect of prone ventilation on maternal and fetal hemodynamics have demonstrated its safety. However, the data on prone ventilation in pregnant women with ARDS is limited to case reports and expert recommendations. 39 Three of the five patients on IMV required prone ventilation. One gravid woman was successfully prone ventilated, while another patient with preterm twin pregnancy underwent CS in view of refractory hypoxemia to facilitate prone ventilation. While prone ventilation is safe in pregnant women, delivery of the fetus should be considered an option in the management of refractory hypoxemia following a multidisciplinary deliberation involving intensivist, obstetrician, neonatologist, and anaesthesiologist, and such decisions are best individualized as the benefit may not be universal. 40
Infective complications were observed in four of our patients with one of them developing a multidrug-resistant infection, however, all of them responded to the treatment. As described earlier, pregnancy and COVID-19 predispose patients to develop thromboembolic complications and warrant thromboprophylaxis.25,26 All our patients received pharmacological or mechanical thromboprophylaxis as indicated with none developing any thromboembolic complications. Our institute, being a quaternary healthcare centre, was well equipped to successfully manage these patients avoiding mortality.
Conclusion
Current evidence is sufficient to suggest that pregnant women are at risk for developing severe manifestations of COVID-19. The challenges in managing this group of patients are unique and require an individualized approach. It is imperative for developing nations to improve healthcare infrastructure to provide quality care for better maternal and neonatal outcomes. With a wide variety of vaccines in use across the world and variations in the COVID-19 virus, the clinical presentation, course, and outcome of this disease are bound to change. More evidence needs to be generated for a better understanding of the disease with newer variants in the post-vaccination era.
Footnotes
Acknowledgements
We would like to thank Ms. Sandhya who helped us with collecting the data and the patients who agreed to be part of the study.
Contributorship
PM conceptualized the study. PM and AK supervised the progress of the study. Data acquisition was done by DS and SM. DS prepared the manuscript. AK contributed to drafting the manuscript. AK and VG critically revised the article. All the authors reviewed and approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Ethical committee approval was waived off as this is a retrospective observational study.
Informed consent
Written informed consent was obtained from patients for their anonymized information to be published in this article.
Guarantor
DS.