
Abstract
Keywords
The incidence of febrile convulsions in Europe is 2% to 5%. Febrile seizure typically happens between the ages of 6 months and 5 years. The first febrile convulsion typically occurs in the first 3 years in 90% of the cases. The febrile convulsion is simple in two-thirds of the cases whereas the other one-third is complicated. The development of status epilepticus is rare (5%). Febrile convulsions occur most often in connection with influenza, adeno-, parainfluenza, and herpes virus infections, but they can also occur because of bacterial infections or after vaccinations.
SARS-CoV-2 infection occurs 20 times less in childhood than in the adult population. COVID-19 infection in children is typically asymptomatic or causes mild symptoms only. A Chinese Study investigated the data of 72,314 patients; only 1% of them infected with SARS-CoV-2 was younger than 10 years, and another 1% belonged to the age group of 10-19 years. The data published by Stafstrom et al 1 show that only 2% of children require hospital admission, and the mortality rate is below 1%, especially in children with serious underlying disease. However, higher mortality was found in SARS-CoV-2–infected adults with epilepsy aged <50 years compared with the population aged >80 years. 2
With the spread of the Omicron variant, the number of infections and hospitalizations in the age group younger than 18 years gradually increased. A meta-analysis involving 3707 children examined the neurologic manifestations of coronavirus infection. Nonspecific neurologic symptoms (headache, muscle pain, fatigue) were found in 16.7% of the children, and only 0.3% had a seizure with or without fever.
In February 2020, the Wuhan Children's Hospital 3 found that none of the children developed neurologic symptoms in the case of 171 infections confirmed by positive polymerase chain reaction polymerase chain reaction test. According to Garazzino, 4 convulsions occurred only in 4.1% of 82 children between age 5 days and 18 years who were infected with SARS-CoV-2. In a multicenter Italian study, among 168 children aged 1-17 years with a positive polymerase chain reaction test, 5 had nonfebrile convulsions (2.9%) and 2 had febrile seizures (1.2%). Karaszi et al 5 investigated 545 patients aged 0-18 years infected with SARS-CoV-2 and only 1 child had generalized tonic-clonic convulsions, but she had an underlying neurologic disease. None of them had febrile convulsions. Cloete et al 6 found that between October 31 and December 31, 2021, 99% of tested pediatric patients in South Africa were positive for the Omicron variant. Among them 25 of 139 children (17.9%) had convulsions (exact data on the nature of the convulsions were not provided). It was found that in 6 cases, simple febrile convulsions appeared outside the characteristic age (younger than 6 months and older than 5 years). Cho et al 7 conducted a multicenter study and found that febrile or nonfebrile convulsions occurred in 5.2% of 2365 children hospitalized for SARS-CoV-2 infection between January 2020 and May 2021. In their opinion, seizure is the only neurologic manifestation of COVID-19 infection that is more common in children than in adults (children 5.2%, adults 1.1%).
According to data, the frequency of febrile convulsions associated with SARS-CoV-2 infection changes relatively widely (0.5%-13%). In a retrospective study, Dilber et al 8 collected data on 382 children aged 0-17 years with a positive polymerase chain reaction test between March 2020 and January 2021 and found febrile convulsions in 9 patients only (2.3%). All these children had their first febrile seizure. Cadet et al 9 examined patients aged 0-5 years, and only 0.5% (44) of the 8854 children with polymerase chain reaction–confirmed coronavirus infection had febrile convulsions. Salleh et al 10 observed febrile convulsions in 13% of children (29 of 219) infected with coronavirus during the Omicron variant; none of their patients had febrile convulsions in the period before this variant occurred. Hanlon et al 11 found febrile convulsions in 2.7% of children (189 of 6923) infected with SARS-CoV-2. Han et al 12 reported febrile convulsions in 9.2% of children (64 of 476) infected with SARS-CoV-2.
Another study 13 revealed that in a patient population under the age 18 years admitted because of SARS-CoV-2 infection, neurologic manifestations occurred in 7% of the cases (1060 of 15 137), and febrile convulsions developed in 3.9% of the children.
Aim of Our Study
The aim of our retrospective study was to investigate whether the incidence of febrile convulsion changed in connection with the COVID-19 pandemic compared to the period prior to the pandemic.
Methods
We reviewed the clinical data of children aged 0-6 years who presented at our university hospital due to febrile convulsions from February 2020 to February 2022. The data were collected from the electronic database based on the diagnosis of febrile convulsion (International Classification of Diseases code R5600). Age of the patients and the type of febrile convulsion (simple or complicated) were examined. Simple febrile seizure was defined as a seizure that occurs with high fever, affects both sides of the body, lasts for a short time (2-5 minutes), happens only once during a febrile illness, and is not associated with residual neurologic symptoms. We considered febrile seizures as complicated if the seizure occurred with subfebrility, it was focal, it took more than 5 minutes, occurred several times in addition to a febrile illness, and/or was associated with residual neurologic symptoms. We paid special attention to the perinatal data, the course of any previous seizures, as well as the family history of a neurologic disease. In addition to clinical symptoms, SARS-CoV-2 infection was confirmed with the Panbio-Abbott or GENEDIA W (Green Cross Medical Science Corp) COVID-19 rapid antigen tests and/or reverse transcriptase–polymerase chain reaction method.
Children who were treated for febrile convulsions at the same university clinic between January 2018 and January 2020 comprised the control group. This is the only university children hospital in our region. All children with COVID-19 infection from this region were admitted to our hospital during the pandemic. The denominator is the number of children who had febrile convulsions during the pandemic, and the numerator is the number of children who had both febrile convulsions and positive COVID test.
All statistical analyses were performed using the SPSS version 28.0 statistics software (IBM, Armonk, NY) and all of them were reviewed by a statistician (L.M.). Mann-Whitney test was used because the criteria using t test were not suitable. First, the normality of data distribution was checked with Q-Q plot and/or box plot, as well as conducted the Shapiro-Wilk test. Mann-Whitney U test was used to determine any differences among the 2 groups according to gestational week and age at onset of convulsions without the assumption of normality. The P values less than .05 were considered to be significant. Each box-plot contains outlier or extreme outlier data, so the normality condition is not satisfied in either case. The median and interquartile range values is given in Table 1. Logistic regression analysis was performed to ascertain the effect of COVID infection on the febrile convulsions.
Occurrence and Characteristics of Febrile Seizure Before and During the Coronavirus Pandemic.a
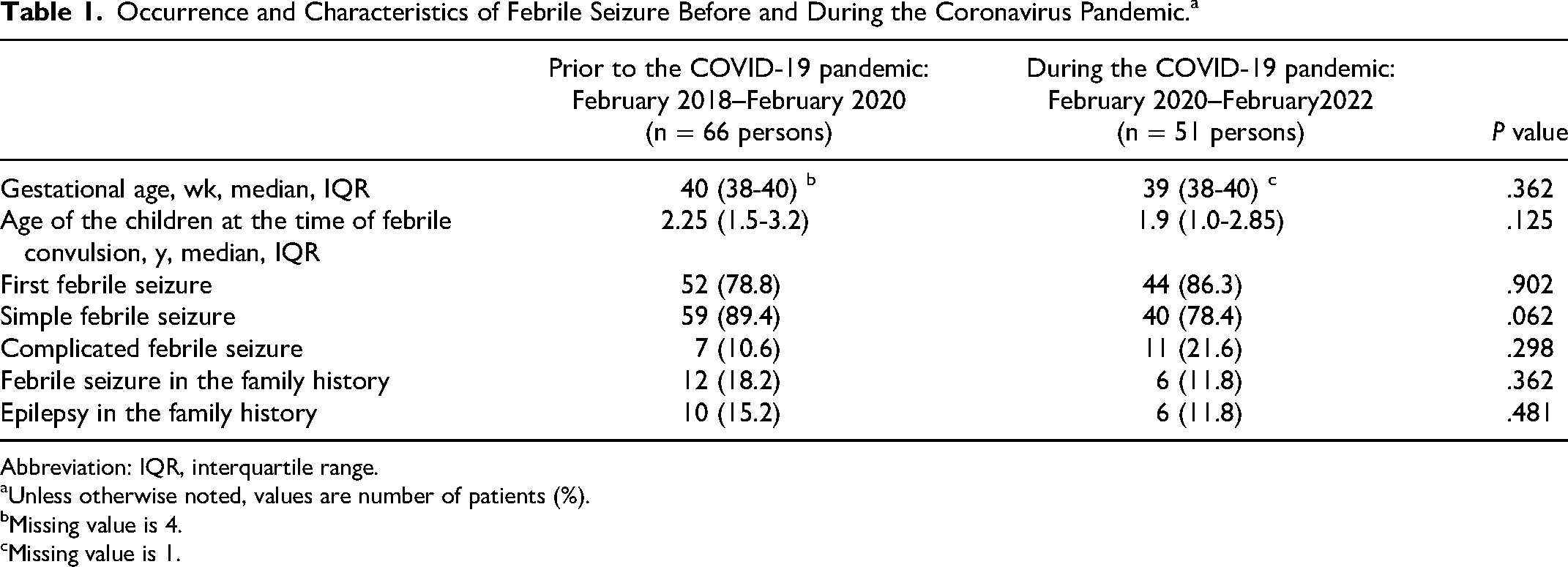
Abbreviation: IQR, interquartile range.
Unless otherwise noted, values are number of patients (%).
Missing value is 4.
Missing value is 1.
Results
From February 2020 to February 2022, a total of 11 318 children, and during the control period a total of 15 375 children were admitted to our university hospital. Overall, 113 children aged <6 years had laboratory-confirmed SARS-CoV-2 infection. In this period, 51 patients were treated with febrile convulsions, but only 4 of them (7.8%) had laboratory-confirmed SARS-CoV-2 infection (Figure 1). Three cases were observed during the Omicron variant period. In 3 children, the results of both the rapid COVID-19 antigen test and the polymerase chain reaction test were positive; in 1 case, only the rapid COVID-19 antigen test was positive. Three patients had their first febrile convulsion, and 1 child had a history of 2 previous febrile seizures. Simple febrile convulsion was registered in 3 cases; only 1 child had complicated febrile seizure.
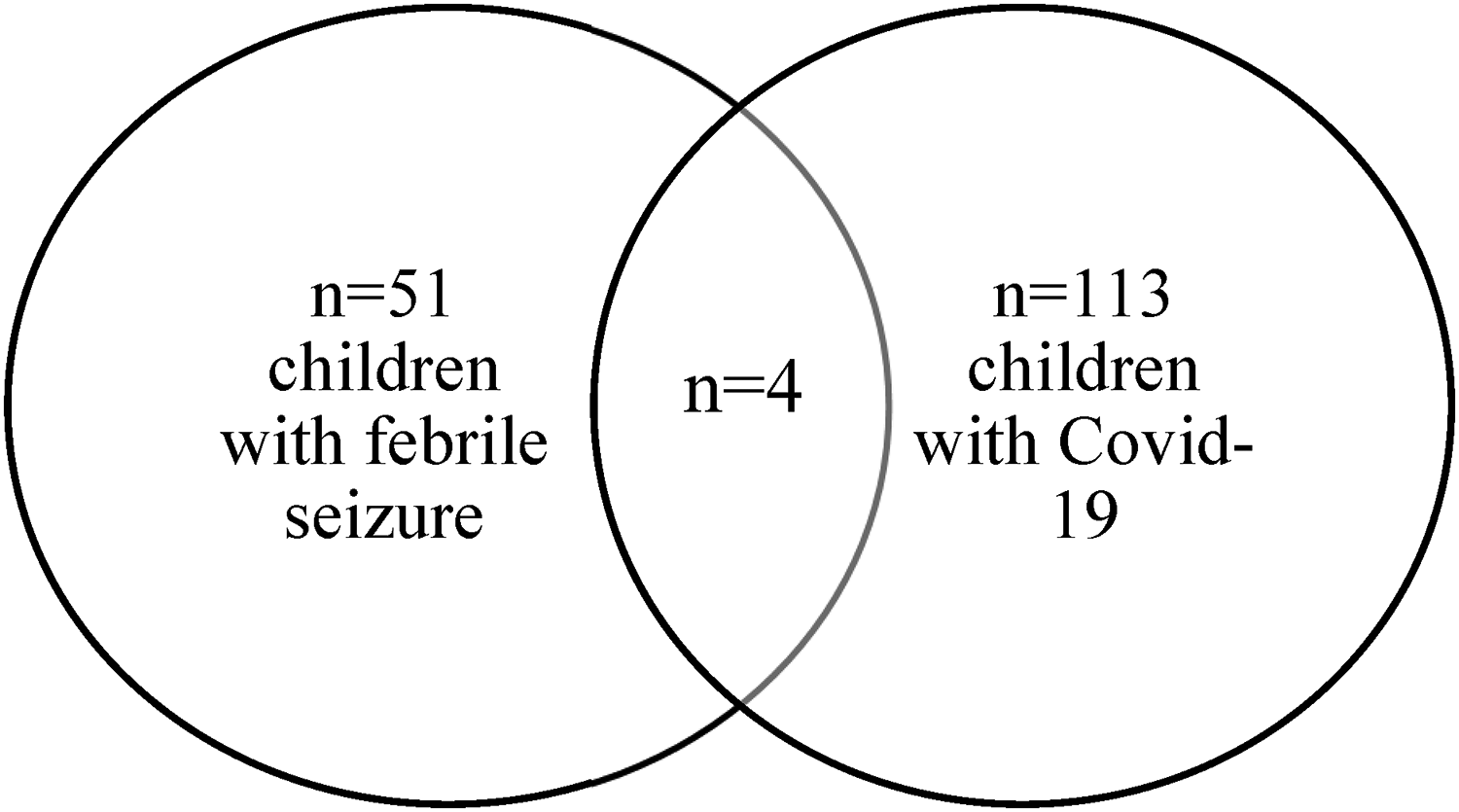
The number of children with febrile seizure, with COVID-19 infection and with febrile seizure and COVID-19 infection during the COVID pandemic February 2020-February 2022.
In the 2-year period before the pandemic, 66 children were treated in our university hospital because of febrile convulsions.
In both the control and pandemic periods, 0.4% of the admitted children were hospitalized because of febrile convulsions (66 of 15 375 children and 51 of 11 318 children).
The age and gestational age of the 2 examined groups were compared using Mann-Whitney U test. Chi-square test was performed for the statistical analysis of the types of febrile seizures and family history.
None of the children had an underlying neurological disease. No statistically significant difference was found between the data of the 2 periods. During the pandemic period, complicated febrile convulsions occurred at a higher rate than simple seizures, but no statistically significant difference could be confirmed (Table 1).
Binary logistic regression model was performed to ascertain the effect of COVID-19 infection on the prevalence of febrile convulsions, on the age and the gestational age of the child during the COVID-19 pandemic (2020-2022). The results of the model were not found statistically significant, χ2(3) = 2.072, P = .557. The model explained 9.5% (Nagelkerke R2) of the variance considering febrile convulsions by covariate and correctly classified 92.0% of cases. The association was not statistically significant (P = .190). Although the test is not significant on checking the odds ratio, in this case it was found that those with positive COVID-19 test results are 4.222 times more likely to experience complicated febrile convulsion than those with negative test results.
We studied the effect of COVID infection on the prevalence of febrile convulsions in the period 2020-2022 and the period 2018-2022. Considering the 2 time periods, statistically nonsignificant (P = .082) association was found. Although the binary logistic regression test was not found statistically significant by checking the odds ratio, it was found that those with a positive COVID-19 test result are 6.062 times more likely to experience complicated febrile convulsion than those with a negative COVID-19 test result. We subsequently examined the effect of COVID infection on the prevalence of febrile convulsions, age of the seizing child, and his or her gestational age during the COVID pandemic (2020-2022) and during 2018-2022 years. The results of the logistic regression model were not found statistically significant, χ2(3) = 3.175, P = .365 in the years 2018-2022.The model explained 10.5% (Nagelkerke R2) of the variance considering febrile convulsions by covariate and correctly classified 96.4% of cases. The results of the logistic regression model were found not statistically significant, χ2(3) = 2.072, P = .557 in the years 2020-2022. The model explained 9.5% (Nagelkerke R2) of the variance considering febrile convulsions by covariate and correctly classified 92.0% of cases. The association values including the odds ratio Exp(B), 95% CI for Exp(B), and P values can be seen in Table 2.
Characteristics of Febrile Seizure Before and During the Coronavirus Pandemic With Binary Logistic Regression Model.
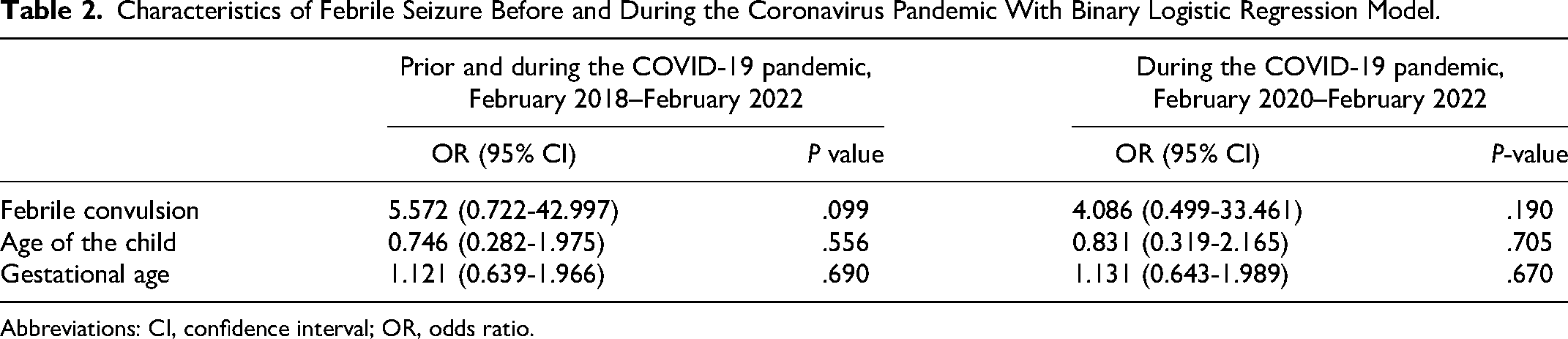
Abbreviations: CI, confidence interval; OR, odds ratio.
It is important to note that although the odds ratio provides some insight into the relationship between a positive COVID-19 test result and febrile convulsions, the nonsignificant P value indicates that the strength of this association may be weak or not statistically reliable because of low sample size.
Discussion
It is well known that the SARS-CoV-2 infection can cause acutely occurring neurologic symptoms (headache, dizziness), but long-lasting neurologic complaints are not uncommon as well.
Reports are controversial regarding whether fever-associated SARS-CoV-2 infection increases the incidence of febrile convulsions in children aged 0-6 years. During the different waves of the coronavirus pandemic, different information was available regarding the occurrence of febrile convulsions. 14
In our study, only 4 (3.5%) of 113 confirmed SARS-CoV-2–infected children under the age of 6 years had febrile convulsion during the pandemic period. This value is a little higher than the 0.5% value obtained by Cadet et al, 9 which can be explained by the much larger patient size in their study. Our 4 children had no family history of febrile convulsions or epilepsy.
Smarrazzo et al 15 observed 56 children with febrile convulsions, of which 2 (3.5%) were confirmed to have coronavirus infection. During the pandemic, we were able to confirm SARS-CoV-2 infection in only 4 (7.8%) of the 51 children who produced almost the same number of febrile convulsions. In 3 cases, simple febrile convulsion, and in 1 case, complicated febrile convulsion were observed. Similar to the data of Hanlon et al, 11 simple febrile convulsions were predominantly diagnosed among our patients.
Our data harmonize with the internationally reported ones that the prevalence of febrile convulsions increased during the period of the Omicron variant. In our study, 3 of 4 children had febrile convulsions during the Omicron variant.
Iijima et al 14 experienced febrile convulsions in 14.6% (22 of 151) of febrile children during the Omicron variant and only 1.7% (2 of 115) of patients in the preceding period. Joung et al 16 also observed statistically significant increase in the period before and during the Omicron variant (0.5% and 62.9%).
We found no statistically significant difference in the age of children with febrile convulsions in the period before and after the coronavirus pandemic (2.4 and 2.2 years) either. In both time periods, most children (78.8% and 86.3%) had their first febrile convulsion.
According to the published data, statistically significantly fewer children were hospitalized during the coronavirus pandemic than prior to it. The most probable explanation for this is that children did not attend the communities (nurseries, kindergartens, schools) and hygiene rules were strictly followed; thus, the rate of diseases spread by droplet infection, mainly of viral origin, decreased. Our data are harmonizing with the results of Chiu et al 17 in that fewer children were examined with the diagnosis of febrile convulsions during the pandemic than before, but contrary to the results of Smarrazzo et al 15 as we did not notice an increase in the incidence of febrile convulsions during the pandemic period.
Strengths and Limitations
Although the number of cases in our study is small, we think an advantage was that we could collect the data of patients from the same admission area of the same university hospital during a 2-year period before and during the pandemic.
Summary
Based on our study, we can conclude that during the pandemic caused by the SARS-CoV-2 infection, we did not experience more frequent febrile convulsions than in the period before the pandemic. We also found no difference in the age of the children at the onset of the first febrile convulsion, and most febrile convulsions were simple type seizures. Looking at the different periods of the coronavirus pandemic, it seems that more febrile convulsions occurred during the Omicron variant than in previous periods. Our observation harmonizes with the international data.
Footnotes
Author Contributions
All authors have agreed to this final version of the paper being submitted to the journal and all contributed equally.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The present study was approved by the local ethics committee (Prot. 1110-0/2021/KK/PTE).