
Abstract
Background
Aortic dilatation and pregnancy are major concerns in women with aortopathy (AOP). This single-centre retrospective analysis focuses on the evolution of aortic diameters during and after pregnancy in women with Marfan syndrome (MS), Turner syndrome (TS) and bicuspid aortic valve (BAV) aortopathy.
Methods and results
Thirty-eight women who had one or more single pregnancies were included. The ascending aorta was measured during pregnancy and postpartum. During pregnancy, a significant increase of diameters of the sinus aortae (median 1.4 mm; [−1.3; 3.8]) and ascending aorta (median 2.1 mm; [0.0; 4.0]) was noted. Systemic hypertension gives dilation of the aorta, but it did not influence the overall trajectory during pregnancy.
Conclusion
Significant aortic dilatation is noted during pregnancy in women with underlying AOP, even persisting in the long term. Pre-existing systemic hypertension is associated with larger aortic diameters prior to pregnancy. More research on a larger study population however is needed.
Keywords
Introduction
Due to better standards of care, in particular reduced haemorrhage and infection, global maternal mortality has declined. However, an increase in maternal heart disease associated with pregnancy has been observed, due to a delay in motherhood, rise in comorbidities and improved survival of women with congenital heart disease (CHD). 1 Maternal heart disease complicates 1% to 4% of the pregnancies, and accounts for up to 15% of maternal deaths, half of it caused by aortic dissection. 2 In a large cohort-crossover analysis aortic dissection affected 5.5 per million patients during pregnancy and postpartum compared with 1.4 in a non-pregnant population. 3 A much higher incidence was found in those with connective tissue disease (4960 per million pregnancies compared to 4.9 per million pregnancies in the general population). Of women with an aortic dissection during pregnancy or postpartum, 62% were diagnosed with an underlying aortopathy (AOP). 4
The registry of pregnancy and cardiac disease (ROPAC) is an international prospective observational registry of pregnant women with CHD, valvular heart disease (VHD), cardiomyopathy (CMP) and ischaemic heart disease. 5 Since 2013 also women with pulmonary arterial hypertension (PAH) and aorta pathology (AOP) have been added to this registry. The primary endpoint was to assess maternal mortality and/or development of heart failure during pregnancy and up to 1 week after delivery. The registry contained 5739 pregnancies from 138 centres in 53 countries. The most important complication seen in this population was heart failure (in 11% of patients) of which 7% occurred in the first week postpartum. Overall maternal mortality was around 0.6%. Patients with PAH, CMP with reduced ejection fraction (less than 30%), dilated CMP and VHD turned out to be at the highest risk. 5
The impact of aortic dilatation and pregnancy related risks is a major concern in women with syndromic or congenital AOP. Patients known with Marfan syndrome (MS), Turner syndrome (TS) and a bicuspid aortic valve (BAV) are at risk for progressive aortic dilatation, aneurysm formation and dissection; the risk for these complications is even higher when being pregnant and this due to haemodynamic changes and hormonal influences on connective tissues. As such pregnancy carries an 8- to-10-fold risk of aortic dissection in MS women compared to non-pregnant MS females, regardless of the aortic size. 6 In MS, most of dissections occur in the ascending aorta and the risk can be as high as 10% if the aortic size exceeds 40 mm.7–10 The highest risk is in the third trimester and peripartum, but also years after due to an accelerated aortic growth during pregnancy.11–14 Overall, it is estimated that there is about a 1% risk of fatal complication rate during pregnancy in Marfan patients. 13
Cardiovascular defects associated with TS include hypoplastic left heart, aortic coarctation and/or aortic valve disease. Systemic hypertension is also commonly seen in these patients. 15 On top of this, aortic dilatation may be underestimated, because of their small stature; TS patients with aortic size index of more than 2.5 cm/m² are reported to be at highest risk of dissection. 16 In women with TS, maternal mortality is estimated at 2%.15,17 The risk of aortic dissection seems to be 1.25% and the risk of severe hypertension after oocyte donation (ART-OD) seems to be significantly higher than in spontaneous pregnancies (this is also seen in non-TS patients with ART-OD).18,19 A possible explanation lies in the fact that women with spontaneous pregnancies tend to be younger and are probably less affected than women requiring assisted reproductive technologies. Another explanation points to the possible negative impact of the hormonal treatment used to prepare the womb on the already existing vascular dysfunction in these patients.
A BAV is the most common congenital cardiac malformation with a prevalence of 1% to 2% in the general population and is complicated by progressive aortic stenosis and/or regurgitation, infective endocarditis and aortic dissection. 20 The risk of aortic dissection is 5- to 18-fold higher in the presence of a BAV. Different hypotheses for these risk are put forward ranging from haemodynamic effects of flow over fused cusps to inherent AOP.21,22 The type of bicuspid valve morphology, aortic dilatation and associated conditions such as aortic coarctation determine the risk of BAV aortopathy and the risk of aortic dissection. Overall the risk of dissection during pregnancy in BAV seems smaller when compared to other conditions. 23
In the ROPAC registry, the rate of dissection in patients with aorta pathology turned out to be 1.8%. However, little is known about the degree of dilatation and associated risk factors during pregnancy in this specific population. 5
In this retrospective analysis, data of pregnant women with MS, TS or BAV were analysed. The primary question was whether there was a significant increase of aortic diameters in this population during pregnancy and in a follow-up period of 5 years if available. Furthermore, the impact of the presence of cardiovascular risk factors and use of medication on the diameters of the aorta were evaluated.
Materials and methods
Patient selection
All women who visited the cardiovascular department between January 2000 and December 2020 who had either MS, TS or a BAV and a first-single pregnancy, were included in this retrospective analysis. One woman with TS and a BAV was excluded due to surgical intervention of a dilated aorta prior to pregnancy. If available, aortic dimensions were considered 5 years after delivery to evaluate a late increase of diameters. Cases were compared with a control group of healthy young women with first pregnancies after a routine obstetric visit confirming a single-viable pregnancy.
Baseline, echocardiographic and outcome characteristics
Thirty-eight first pregnancies were included. Twenty-two women were known with a BAV, nine with MS and seven with TS. The use of assisted fertilisation was documented. Each woman was screened for cardiovascular risk factors: systemic hypertension, diabetes mellitus, smoking, familial history and obesity. Systemic hypertension was defined as a blood pressure more than 140 mmHg in systole or more than 90 mmHg in diastole, obesity as a BMI before pregnancy of more than 25 kg/m². The use of cardiovascular and other medication was considered.
The ascending aorta was measured using transthoracic echocardiography in systole at the annulus, sinus, and ascending aorta leading edge to leading edge in millimetre in a parasternal long axis 2D view. It was measured during the first, second, and third trimester, as well as postpartum by the same echographer. The first trimester echocardiography was defined as an examination between 12 and 16 weeks of gestation, the second between 20 and 24 weeks and the third between 30 and 34 weeks. Postpartum echocardiographic examination was performed between 5 and 7 months after delivery. If available, the aortic dimensions were considered 5 years after delivery to evaluate a late increase.
Statistical analysis
Continuous baseline characteristics were reported by mean and standard deviations and categorical data were summarised by frequencies and percentages. Wilcoxon test is used to assess the differences of continuous variables both for paired and independent groups, Chi-squared test is applied to compare the categorical variables between groups. Results were reported as median with a range since the distribution is not normal. All tests were two-sided and assessed at a significance level of 5%.
Linear mixed effects models were performed to assess changes over time for the repeated measurements of aortic diameters. 24 Linear mixed effects models account for variability between subjects and variability between repeated measurements in the same subject simultaneously. The intercept and slope effect were included as random effects; age of pregnancy, assisted fertilisation and cardiovascular risk factors as fixed effects. For the case–control study, an interaction effect of time and group variables were included. The variance–covariance structure was fixed to an unstructured matrix and the random effects and error terms were assumed to have a normal distribution. A two-sided p-value < 0.05 was considered statistically significant.
The nonlinear mixed effect models package of R-project (version 3.5.0, Vienna, Austria) was used to estimate all the linear mixed effects models.
Results
Thirty-eight pregnancies in women with MS (n = 9), TS (n = 7) or a BAV (n = 22) were analysed. Patient characteristics can be found in Table 1. Mean age at pregnancy was 29.0 ± 4.4 years. A total of 8 pregnancies (MS n = 4, TS n = 4) were achieved using assisted fertilisation. Twelve women were obese, three were smokers, thirteen had systemic hypertension, four had a family history of cardiovascular disease and one had diabetes mellitus type 2 before the start of the pregnancy.
Patient characteristics.
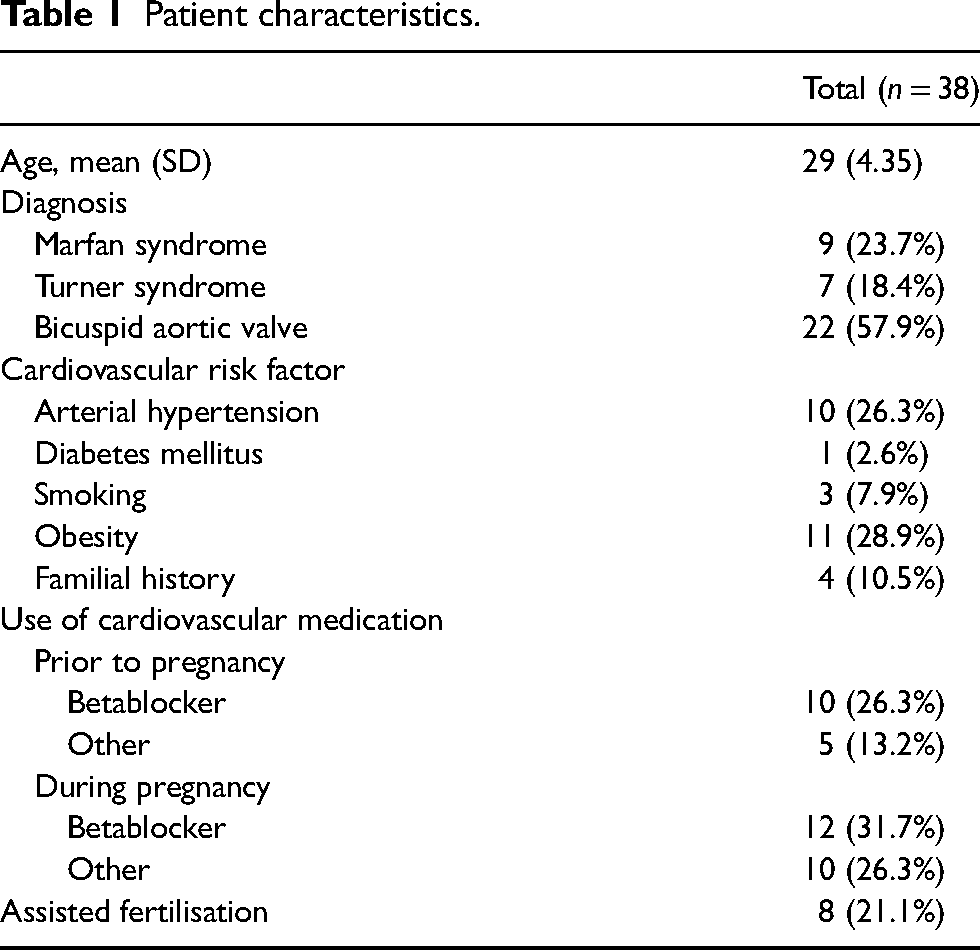
Betablockers were used frequently, before pregnancy 26.3% (n = 10) and during 31.7% (n = 12). The indication for starting during pregnancy was systemic hypertension. Of the nine MS women, seven were already on betablockade before pregnancy to prevent cardiovascular complications and aortic dilatation according to current guidelines. 23
During pregnancy, a significant increase of diameters of the sinus aortae and ascending aorta up to the postpartum was observed; median increase was 1.4 mm [−1.2; 3.8] and 2.1 mm [0.0; 4.0] at the level of the sinus and ascending aorta, respectively (p < 0.001). The annulus aortae showed a significant increase in diameter (median 2.0 mm [1.3; 3.5]) up to the third trimester of the pregnancy, with a significant decrease postpartum (median 1.3 mm [−1.1; 2.9]) (Figure 1).
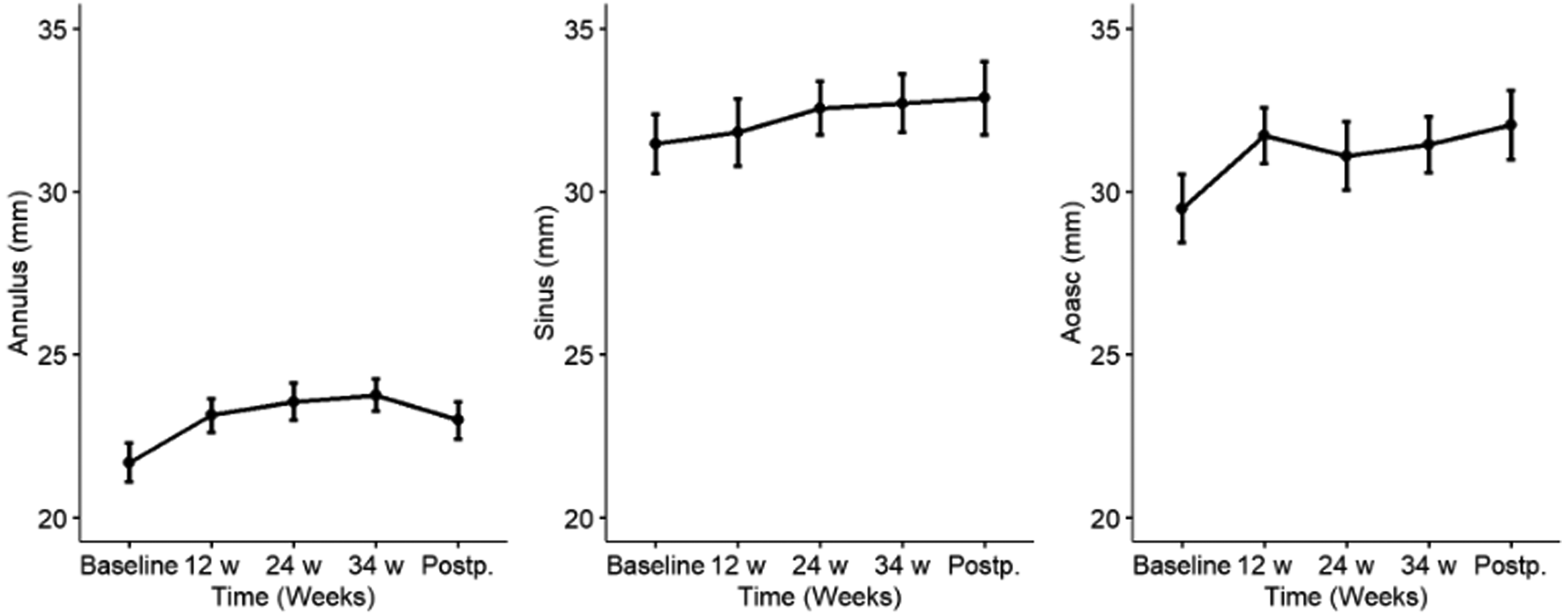
Diameters of respectively the annulus aorta, sinus aortae and aorta ascendens (Aoasc) during pregnancy and postpartum. Represented as mean and standard deviations for each time point.
In 47.4% of the 38 pregnancies (n = 18), sufficient data were available on aortic diameters 5 years postpartum. The paired Wilcoxon test to evaluate differences between baseline and 5 years showed a trend towards persistent dilation of the diameters (median 2.7 mm [−1.5; 6.2]) (Figure 2).
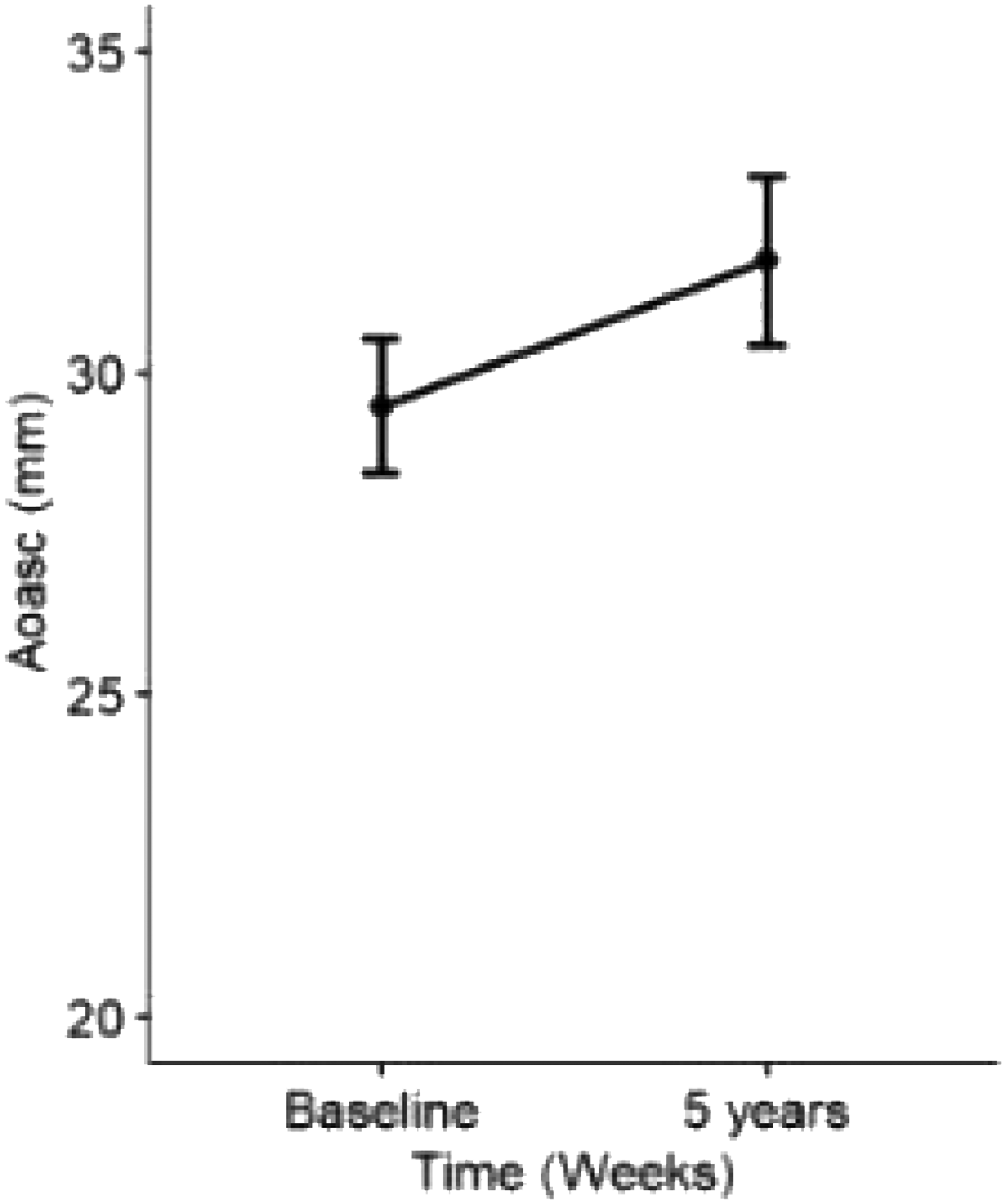
Diameters of aorta ascendens at baseline and 5 years postpartum. Represented as mean and standard deviation for each time point.
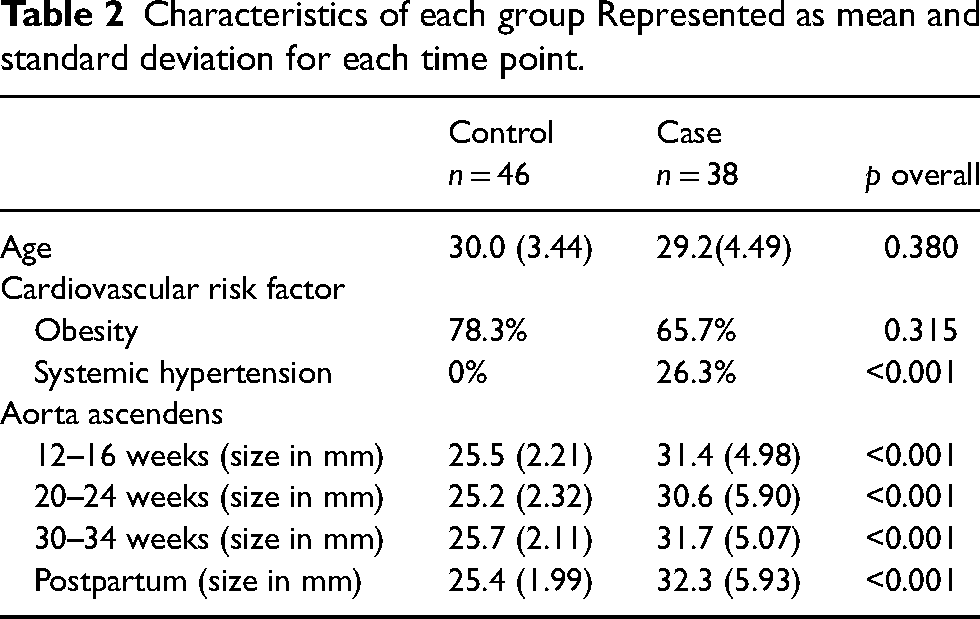
Comparing the aortic diameters with a control group of healthy individual women during pregnancy (data derived from a database) showed statistically significant intercepts for the aorta ascendens. However, linear mixed effects models’ results showed that the trajectories for both groups have not a significant change over time. Patient characteristics and comparison of the cases and controls can be found in Table 2.
Characteristics of each group Represented as mean and standard deviation for each time point.
There were no complications such as aortic dissection or rupture noted during or after pregnancy. However, one woman with MS died 4 days postpartum, possibly due to malignant arrhythmia as post-mortem macroscopic and microscopic autopsy could not reveal any other cause. Another woman with a BAV died 1 year postpartum because of suicide.
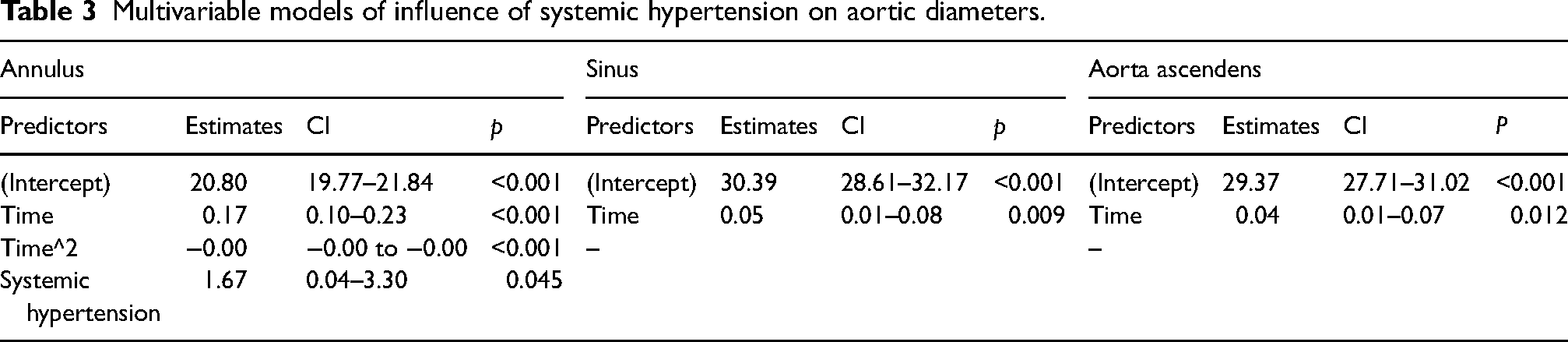
Multivariable models showed that systemic hypertension was the only risk factor for increasing aortic diameters (β = 1.67, 95% CI = 0.04–3.30, p = 0.045) (Table 3). The presence of systemic hypertension had an influence on the diameters of the aorta before pregnancy but did not influence the overall trajectory during pregnancy. No influence was found of the presence of multiple risk factors, analysed with multivariable models after a variable selection. There was a trend to a smaller increase in the annulus aorta and the sinus aortae when using betablocker.
Multivariable models of influence of systemic hypertension on aortic diameters.
Discussion
The main finding of this retrospective analysis was that significant aortic dilatation is observed during pregnancy in women with underlying AOP, even persisting in the long term.
A total of 38 first pregnancies were studied in patients with an AOP, such as MS, TS and a BAV. All these AOP are known to have a higher life-time risk of aortic dilatation, dissection, or rupture. Complications occur typically at a younger age (<40 years). 4
Except one, all Marfan pregnancies in our analysis had extensive pre-pregnancy counselling in our outpatient clinic with echocardiography; one woman was referred during the second trimester from a large peripheral hospital. Of these patients, four women had diameters of the sinus greater than 40 mm prior to pregnancy and were already treated with betablockers (if not already taken). None of these patients developed an aortic dissection during pregnancy nor in the early postpartum. One woman died in the early postpartum possibly due to malignant arrhythmia. Of note is that almost all Marfan women were already on preventive betablocker treatment prior to conception, according to European and American guidelines. 23 Also our pregnant Turner women were strictly monitored for gestational systemic hypertension if not already known and treated before pregnancy.
A retrospective observational study by Toprak et al. analysed the risks of pregnancy in women with MS or a BAV. 25 During pregnancy itself and up to 6 months postpartum, women with MS but not BAV showed an increased risk of aortic dissection. In the long term (i.e. more than 6 months postpartum up to maximum 13 years), however, they did not find an association between ever-pregnant and never-pregnant women and an increased risk of aortic dissection or surgery. Our results showed a significant increase of diameters of the sinus aortae and ascending aorta up to the postpartum. Even 5 years after pregnancy, we found a trend to a persistence in the dilatation of the aortic diameters. Those findings are consistent with the findings of Donnelly et al. who found an increased aortic growth rate in patients with MS who did not return to baseline values even after 5 years. 11 In patients with a BAV this evolution is less clear.25,26 Due to the small number of patients enrolled, a subanalysis of patients with MS, TS or a BAV was not done in this retrospective analysis.
None of the women in this analysis experienced an aortic dissection during pregnancy nor in the postpartum but this can be due to the small number of patients and the short follow-up period as well as a bias of selected patients in a tertiary care centre.
On top of major haemodynamic changes to meet the need of increased cardiac output, connective tissue changes take place as well. The complex interaction between the haemodynamic and connective tissue changes contributes to the increase of aortic diameters, even in a population of healthy pregnant women. 27 The results of this analysis confirmed a very mild dilatation of the aorta in healthy pregnant controls during pregnancy however with rapid recovery in the postpartum period.
Since the known increased risk of aortic dilatation and dissection occurring during pregnancy, current European and American guidelines suggest an aortic root replacement if aortic diameter exceeds 45 mm in MS, 50 mm in BAV and 27 mm/m² in patients with TS. It is important to adjust to body surface area in women with TS, since absolute values may seem small due to their short stature. 23 We did not correct for body surface area in women with TS, since we looked at the overall evolution of the aortic diameters during pregnancy. Pre-pregnancy counselling is therefore vital, and imaging of the aorta (with either computer tomography or magnetic resonance imaging) is strongly suggested. Follow-up should be performed every 4 to 12 weeks and 6 months after delivery. Echocardiographic evaluation remains the golden standard, since its availability and safe use during pregnancy. When needed, magnetic resonance imaging is also an option.
Besides the risk associated with the disease itself, the number of pregnancies, uncontrolled systemic hypertension and a family history of thoracic aneurysm/dissection also increases the risk of aortic dilatation and dissection. Also smoking, aortic size and rapid growth increases the risk for aortic pathology during pregnancy.7,28 Analysis of the presence of standard cardiovascular risk factors (obesity, smoking, systemic hypertension, family history or diabetes) revealed a significant association in our study of systemic hypertension and larger aortic diameters before pregnancy. The overall trajectory of the diameters did not differ however between women with AOP and systemic hypertension and women with AOP without systemic hypertension.
Some reports show evidence for the use of beta blockers to prevent aortic growth especially in patients with MS.7,9 This would be due to a decrease in blood pressure as well as the reduction in the shear forces on the aortic wall. However, evidence remains limited and controversial. A meta-analysis, performed by Gersony et al. could not reveal any statistical significance of reduced aortic growth or complications in patients with MS. 29 It is important to note that this analysis contained only one randomised control trial. 30 Nevertheless, guidelines still advise to consider the preventive use of betablockade during pregnancy since the possible benefits and the relatively small risk of adverse fetal outcome.1,23 This analysis also found a trend towards a smaller increase in aortic diameters in women using betablockade. However, these findings could partially reflect better blood pressure control during pregnancy. Angiotensin-converting enzyme inhibitors and angiotensin receptor blockers could also have a reduction in aortic growth in MS; however, this medication is contra-indicated in pregnancy due to possible adverse effects on the fetus. 31 Overall, tight control of all cardiovascular risk factors and rigorous blood pressure control should be strongly advised in these women to ameliorate both maternal and fetal outcome.
Limitations
This analysis has several limitations. First, there is the limitation of the retrospective design, single-centre analysis, the small study population (although in line with other analyses performed) and the limited follow-up time.
Secondly, there is an important selection bias of women. At one hand, women included in this analysis are women with a good follow-up in a specialised tertiary centre. On the other hand, it could be that only less affected women made the choice of becoming pregnant (such as women with MS with less complications).
To avoid the effect of multiple pregnancies on aortic diameters, only the first pregnancy of each woman was evaluated. However, in the follow-up period of 5 years, multiple pregnancies during this period were not considered (given the already small study population).
Every echocardiography was performed by the same investigator. However, intraobserver variability was not tested and the known limitations of echocardiographic measurements remain.
In the control group of healthy pregnant women, pre-pregnancy values were absent since these women were enrolled after confirmation of a single-viable pregnancy. The population did not match with our cases for the presence of systemic hypertension.
Finally, this analysis contains a heterogenous population of women with AOP. Since investigations confirmed that the anatomic site of major aortic pathology was distinct (a BAV gives more dilatation of the ascending aorta where MS tends to affect the more proximal segments of the aortic root), this could affect the analysis and minimise aortic growth in for example patients with a BAV.
Conclusion
In this retrospective analysis we examined the presence and impact of aortic complications in pregnant women with MS, TS or a BAV. Significant aortic dilatation is noted during pregnancy in women with underlying AOP, even persisting in the long term. No aortic dissection during pregnancy or in the postpartum period was reported. Pre-existing systemic hypertension is associated with larger aortic diameters prior to pregnancy. Tight control of cardiac risk factors and rigorous blood pressure control is therefore advised in this subset of women. The advantages of beta blocker use during pregnancy in selected women outweigh the fetal risks of lower birth weight. More research on a larger study population however is needed to provide patients-tailored advice.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Ethical approval
This study was approved by the Ethical Committee of UZ Leuven (MP013636).
Informed consent
Informed consent was not sought for the present study because of the retrospective nature of the study.
Guarantor
ET
Contributorship
AC and ET wrote the first draft of the manuscript after an extensive research in the literature and a thoroughly retrospective analyses. All authors reviewed and edited the manuscript and approved the final version of the manuscript.