
Abstract
Background
Cardiovascular symptoms in pregnancy may be a clue to psychological distress. We examined whether electrocardiogram testing in pregnant women is associated with an increased risk of subsequent postpartum depression.
Methods
We conducted a population-based cohort study of pregnant women who delivered in Ontario, Canada comparing women who received a prenatal ECG to women who did not.
Results
In total, 3,238,218 women gave birth during the 25-year study period of whom 157,352 (5%) received an electrocardiogram during prenatal care. Receiving an electrocardiogram test was associated with a one-third relative increase in the odds of postpartum depression (odds ratio 1.34; 95% confidence interval 1.29–1.39, p < 0.001).
Conclusion
The association between prenatal electrocardiogram testing and postpartum depression suggests a possible link of organic disease with mental illness, and emphasizes that cardiovascular symptoms may be a clinical clue to the presence of an underlying mood disorder.
Introduction
Postpartum depression affects 1 in 10 women in the year following childbirth.1,2 Classic features include decreased mood, disturbances of sleep, excessive fatigue, weight changes, and feelings of worthlessness that can be particularly problematic for new mothers who are adjusting to life with a new baby.3–5 Postpartum depression can interfere with breastfeeding, impair infant bonding, and potentially effect neurocognitive development for a child.6–8 In 2017, the total societal cost of untreated perinatal mood and anxiety disorders in the US was $14.2 billion. 9 In addition, suicide is a major cause of postpartum mortality with rates of 1 to 5 per 100,000 in high income countries.10–12
Electrocardiograms (ECGs) are simple diagnostic tests that pose no real immediate physical risks to a pregnant woman. Guidelines suggest ECGs can be indicated for pregnant women presenting with chest pain, shortness of breath, or unexplained palpitations. 13 However, such symptoms are often due to normal physiologic changes of pregnancy rather than serious pathology. The heart rate increases substantially during pregnancy and ectopic beats with a non-sustained arrhythmia are detected in over half of pregnant women. 14 Furthermore, one-in-seven pregnant women have nonspecific ECG waveform changes that completely resolve following delivery. 15 These ECG abnormalities rarely indicate cardiovascular disease.
Mood disorders frequently manifest with somatic symptoms, and women with depression have a high prevalence of sinus arrhythmias. 16 In addition, simple medical tests may be distressing to some women, particularly if results are equivocal and more investigations are pursued. 17 In the general adult population, ECG testing is associated with a fivefold risk of additional cardiovascular procedures. 18 Moreover, pregnant women may be less accustomed to extensive medical testing and ECGs are not part of routine prenatal assessments. Whether cardiovascular testing in pregnancy can predict postpartum depression is unknown. We examined whether ECG testing of women during pregnancy was associated with an increased risk of subsequent postpartum depression.
Methods
Study setting
We performed a population-based cohort study of postpartum women in Ontario, Canada to examine the association between ECG testing in pregnancy and postpartum depression. Ontario is Canada’s largest province with a population of 12,160,282 and 135,595 live births in 2006 (study midpoint).19,20 In Ontario, women have access to universal health insurance coverage with no out-of-pocket costs for medical services including prenatal care, ECG testing, and psychiatric services. In addition, health care records can be tracked through established database analyses. 21 The study protocol was approved by the Research Ethics Board at Sunnybrook Health Sciences Centre, including a waiver for individual’s consent.
Patient identification
We identified women 14–55 years old who had a live birth in Ontario, Canada between 1 April 1993 and 31 March 2018 (enrolment interval of 25 years). This interval was selected to cover all available data and provide a minimum follow-up of one-year after delivery. To identify eligible women we linked maternal–newborn pairs using the MOMBABY database, which identified more than 98% of all Ontario births. 22 We excluded women with a missing health card as they were ineligible for healthcare coverage under the Ontario Health Insurance Plan (OHIP). Different pregnancies (by the same mother) were coded as separate occurrences so that each delivery was included for each woman (no statistical adjustments for possible clustering). Pregnancies resulting in a stillbirth were excluded.
Electrocardiogram testing
The primary analysis compared women who had received an ECG during pregnancy to those who had not. ECGs are readily available diagnostic tests in Ontario, with 4.7 million ECG diagnostic tests ordered in 2014 alone. 23 Less than a quarter of adult women in Ontario who have an annual health examination receive a routine ECG. 18 The technical and professional components have fees of $6.60 and $4.45, respectively. 24 We identified ECGs performed during pregnancy through claims in the OHIP database using the specific procedure codes during the 40 weeks before delivery (G310 and G311). These codes have been used in prior studies to reliably identify physician claims for the procedure. 18 We also used these codes to additionally identify earlier ECGs during the year prior to conception.
Additional characteristics
We defined additional baseline individual characteristics at the time of delivery by linking administrative healthcare databases. We obtained basic maternal demographic information including age, socioeconomic status, and home location using the Registered Persons Database, which is the registry of individuals eligible for provincial health insurance.25,26 We obtained hospitalization data from the Canadian Institute for Health Information Discharge Abstract Database. 27 We obtained data on outpatient clinic visits using the OHIP database. 28 We obtained further data about pregnancy and delivery for the maternal-newborn pair using the MOMBABY database. The date of conception was estimated by subtracting the gestational age at delivery from the date of delivery (index date).
Postpartum depression
The primary outcome was a physician diagnosis of postpartum depression (ICD-9 code 311) during the year after delivery determined through the validated OHIP database. This definition excluded psychotic disorders, substance abuse, or other psychiatric diagnoses. To minimize false-positive results, we required physician contact for a diagnosis of depression on two separate occasions in the first postpartum year. Using this stringent definition of two separate depression claims has a specificity of 94% and sensitivity of 61% (positive predictive value of 70%, negative predictive value of 92%). 29 Other studies have used similar approaches to ascertaining postpartum mental health diagnoses.30,31 We assumed that women without an ICD diagnosis code for depression did not have postpartum depression. The baseline incidence of postpartum depression among Canadian women with no history of mental illness is approximately 45 per 1000 when based on broader definitions of mental illness. 32
Additional diagnostic procedures
We used OHIP claims to identify five other non-invasive procedures in addition to an ECG ordered in pregnancy: echocardiogram, Holter monitor, chest X-ray, leg Doppler, and abdominal ultrasound.18,33–36 We also used OHIP claims to identify routine screening tests for pregnant women: urinalysis, glucose tolerance testing, and anemia. Information on prescription drugs was not available for women in our study due to the absence of universal drug coverage. Social services and psychology assessments were not available in the health services databases.
Statistical analysis
We used logistic regression to examine the incidence of postpartum depression within one year (binary outcome), comparing women who received an ECG during pregnancy to women who did not receive an ECG during pregnancy. Statistical testing examined associations before and after adjusting for measured baseline characteristics (Table 1) to assess for robustness in our risk estimates. Results based on proportional hazards analysis instead of logistic regression analysis yielded almost identical results and are shown as an additional test of robustness. Odds ratios were represented with 95% confidence intervals and a two-tailed type 1 error rate of 0.05 defined the threshold for statistical significance. All analyses were performed using SAS statistical software (v 9.4; SAS Institute, Cary, NC).
Baseline characteristics.
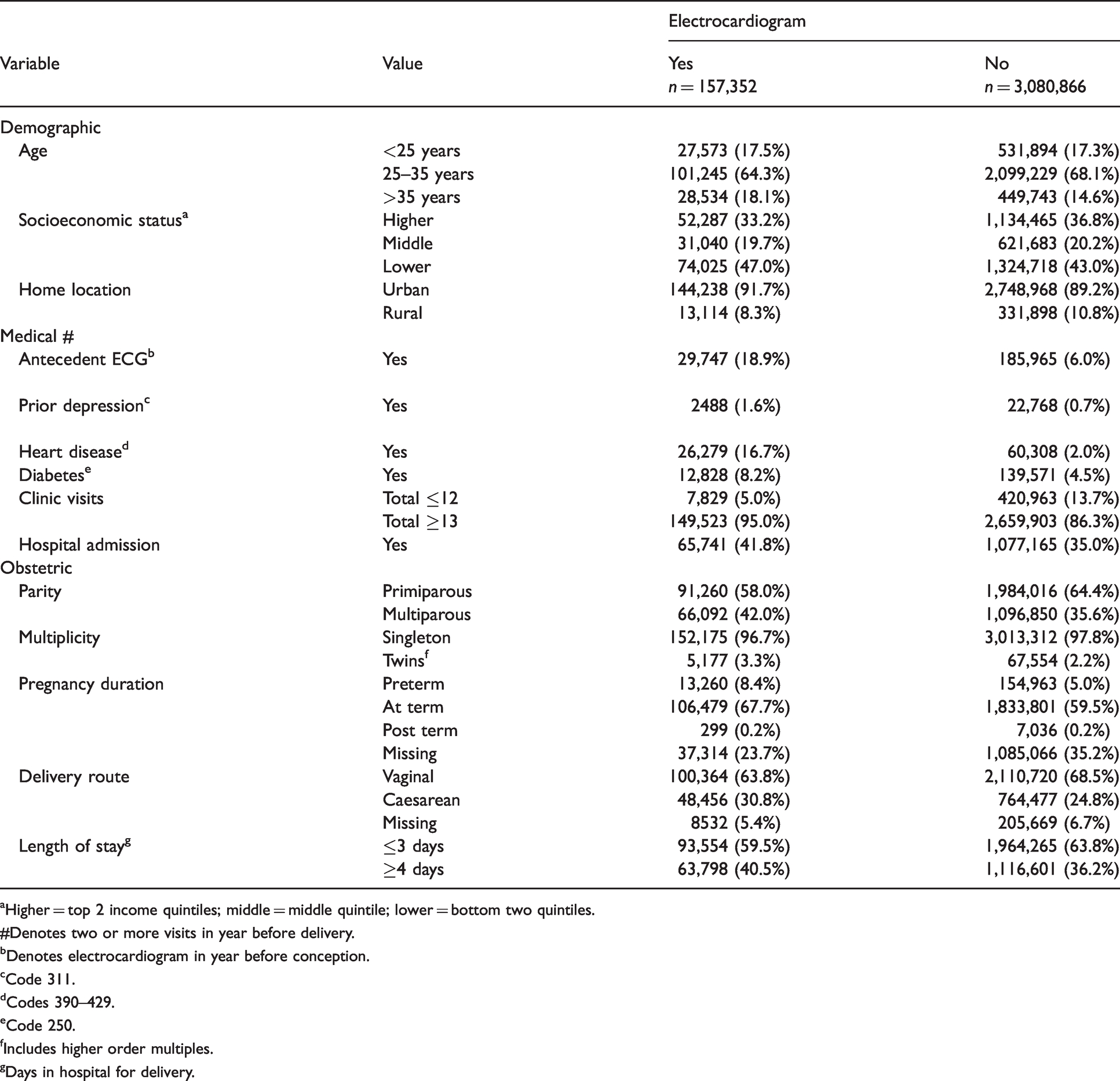
aHigher = top 2 income quintiles; middle = middle quintile; lower = bottom two quintiles.
#Denotes two or more visits in year before delivery.
bDenotes electrocardiogram in year before conception.
cCode 311.
dCodes 390–429.
eCode 250.
fIncludes higher order multiples.
gDays in hospital for delivery.
To test the robustness of our findings we explored how an association between prenatal ECG testing and postpartum depression might extend across a spectrum of severity. First, we performed a sensitivity analysis restricted to women with a term delivery, a normal hospital stay, no history of depression, heart disease, diabetes, no prior ECG, and no hospitalization in the previous year. Second, we performed an analysis where greater numbers of outpatient clinic visits for postpartum depression were required to meet criteria for a severe postpartum depression. Third, we examined the more stringent outcome of depression leading to a hospital admission (depression was listed as a contributing diagnosis but not necessarily the most responsible diagnosis). Fourth, we examined a broader outcome by including other mental health disorders in the year after delivery (codes 300–304, 305, 309, 311) (Appendix 1).
We also performed analyses to explore the frequency of depression in postpartum women who received additional other cardiovascular procedures: echocardiogram, Holter monitor, chest X-ray, leg Dopplers, and abdominal ultrasound. We assessed for dose response by examining the apparent impact of multiple rather than a single ECG test on the risk of postpartum depression. We examined the cascade of test ordering by evaluating the likelihood of women receiving subsequent diagnostic tests (e.g., echocardiogram) following an initial ECG. We performed a counterfactual specificity analysis examining the association between routine screening ordered in pregnancy (urinalysis, glucose, anemia) and postpartum depression.
Results
Descriptive overview
In total, 3,238,218 women gave birth during the 25-year study period. Overall, 157,352 (nearly 1-in-20) received an ECG during prenatal care. Women spanned a wide range of socioeconomic status and the median age was 30 years (Table 1). The majority lived in a city and had no history of depression or heart disease. Most gave birth at term with a vaginal delivery and stayed in hospital less than four days. As expected, women who received an ECG relative to those who did not receive an ECG were slightly older, more likely to have a past history of heart disease, and more likely to have received an additional ECG in the year prior to pregnancy. The majority of women in both groups had more than a dozen prenatal care visits before delivery. The overall frequency of heart disease was 2.7%. Most ECG tests were in the first two trimesters (75%).
Subsequent depression
The women in our cohort accounted for 3,205,649.6 patient-years of subsequent follow-up (mean: 0.99 years). Women who received an ECG during prenatal care accounted for 3932 cases of subsequent depression over 154,597.6 patient-years of follow-up (mean: 0.98 years), equal to an incidence of 25 per 1000 annually. Women who did not receive an ECG during prenatal care accounted for 44,115 cases of subsequent depression over 3,051,052 patient-years of follow-up (mean: 0.99 years), equal to an incidence of 14 per 1000 annually. Together, receiving an ECG was associated with a 1.76 increased odds of subsequent depression (95% confidence interval 1.71–1.82, p < 0.001). About half of the postpartum cases of depression occurred after the first three months (Figure 1).
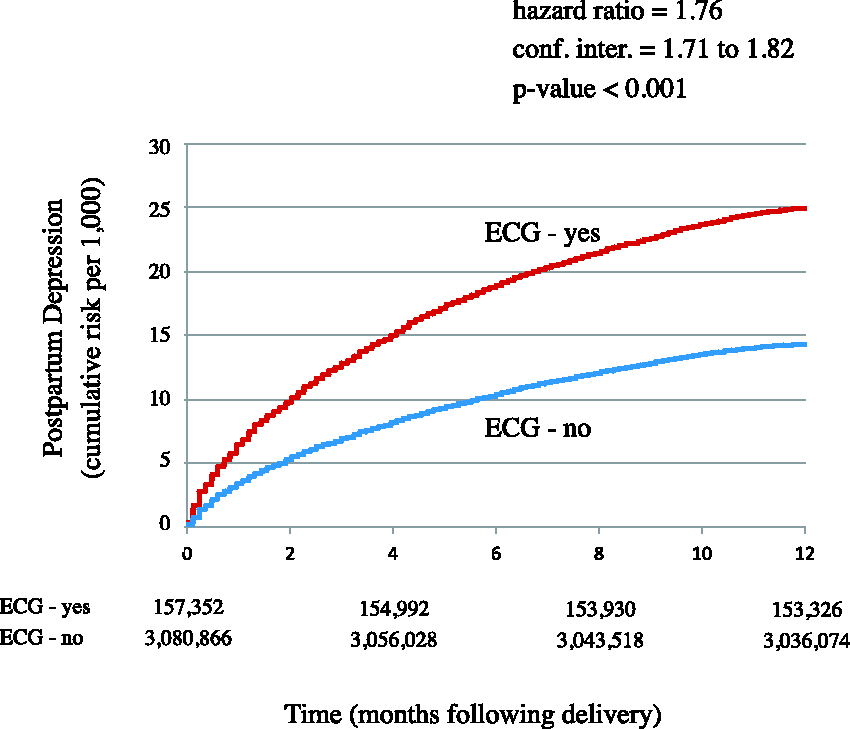
Risk of postpartum depression. Cumulative incidence plots of absolute risk of postpartum depression. X-axis shows time following delivery spanning first year. Y-axis shows cumulative incidence of depression per 1000 individuals. Numerical counts show proportion of women with no depression at corresponding time. P value and hazard ratio based on Fine and Gray model. Results show substantial incidence of depression, particularly for women who received an ECG during prenatal care.
Other factors associated with depression
The risk of postpartum depression was also related to individual characteristics. Younger age, a rural home location, an ECG prior to conception, and a history of heart disease were each associated with increased odds of postpartum depression (Table 2). The strongest risk factor was a past history of depression. Additional predictors included an increased number of prenatal care visits, a prior hospital admission, being multiparous, a preterm delivery, and a longer hospital length of stay (perhaps each as indirect measures of comorbidity). Conversely, socioeconomic status was not a significant predictor after accounting for other factors. Adjustment for all measured women factors suggested that receiving an ECG test was associated with a 1.34 increased odds of postpartum depression (95% confidence interval 1.29–1.39, p < 0.001).
Predictors of depression in year following delivery.
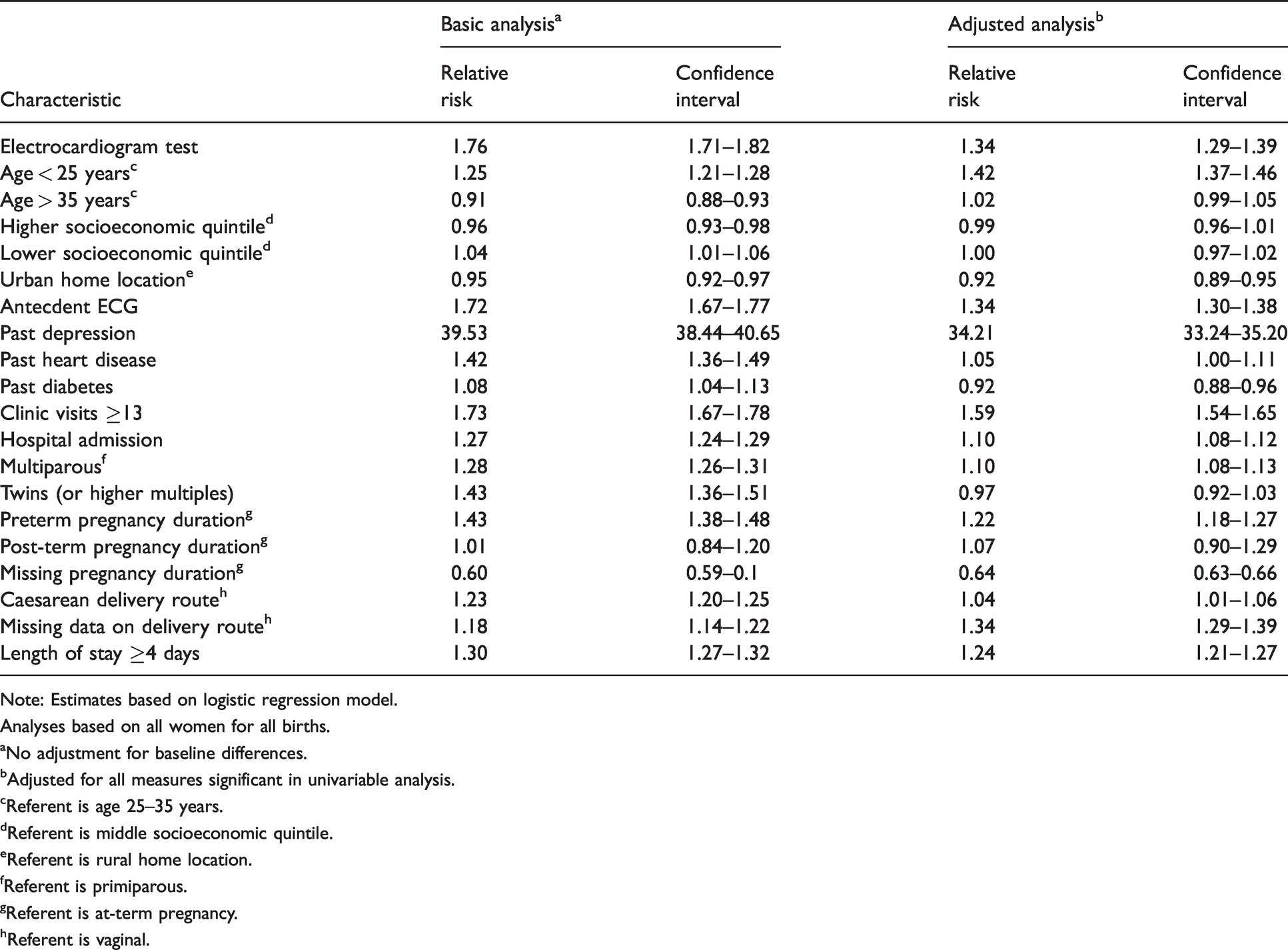
Note: Estimates based on logistic regression model.
Analyses based on all women for all births.
aNo adjustment for baseline differences.
bAdjusted for all measures significant in univariable analysis.
cReferent is age 25–35 years.
dReferent is middle socioeconomic quintile.
eReferent is rural home location.
fReferent is primiparous.
gReferent is at-term pregnancy.
hReferent is vaginal.
Subgroup analyses
We conducted a further check for confounding by replicating the analysis for women who had a term delivery; hospital stay ≤3 days; no history of depression, heart disease, diabetes; no prior ECG; and no hospitalization in the past year. This resulted in a subgroup of 911,762 women of whom 34,054 (3.7%) received an ECG during prenatal care. Those who received an ECG accounted for 593 cases of postpartum depression over 33,666.8 patient-years of follow-up, equal to 18 per 1000 annually. Those who did not receive an ECG accounted for 10,238 cases of postpartum depression over 871,116.3 patient-years of follow-up, equal to 12 per 1000 annually. Together, this subgroup suggested receiving a prenatal ECG was associated with a 1.50 increased odds of postpartum depression (95% confidence interval 1.38–1.63, p < 0.001).
Secondary analyses
We conducted two further analyses to examine the validity of the association between receiving a prenatal ECG and risk of postpartum depression. The first analysis assessed a dose–response gradient by comparing women who received exactly two ECG tests to women who received exactly one ECG test and observed a further increase in depression (31 vs. 24 per 1000, p < 0.001). Analyses based on higher numbers of ECG tests yielded no further increases in risk (Figure 2). The second analysis assessed counterfactual specificity by comparing women who received a screening urinalysis (n = 2,969,795; 92%) to women who did not (n = 268,423; 8%) and observed only a slight increase in depression (15 vs. 14 per 1000, p < 0.001). Additional assessments based on glucose screening (15 vs. 14 per 1000, p = 0.001) or anemia (15 vs. 14 per 1000, p < 0.001) screening yielded similar patterns.
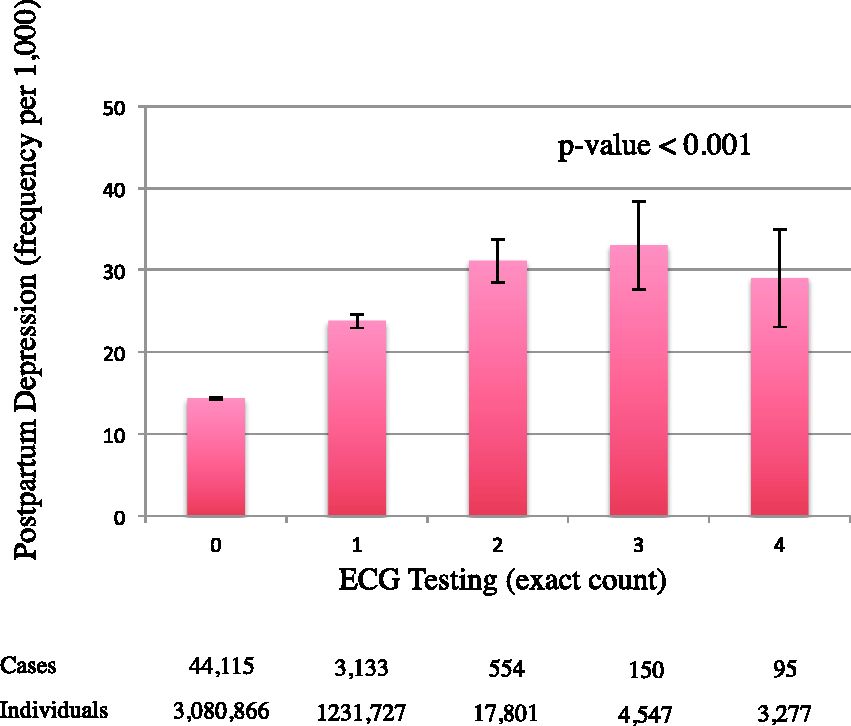
Dose response gradient. Frequency of postpartum depression stratified by number of ECG tests in prenatal interval. X-axis shows specific number ranging from 0 to 4 (final category also includes those with ≥4). Y-axis shows cumulative risk of postpartum depression expressed per 1000 women. Vertical lines denote 95% confidence interval for each analysis. P value indicates test for trend. Numerical counts show total number of women in corresponding subgroup. Results show trend where greater number of ECG tests in prenatal care associated with greater frequency of postpartum depression.
Additional cardiovascular testing
We conducted further supplementary analyses to examine how receiving a prenatal ECG might lead to additional prenatal cardiovascular diagnostic procedures. Overall, we found a significant increase for each procedure comparing women who received a prenatal ECG test to women who did not receive a prenatal ECG test. The results were particularly striking for the likelihood of receiving a prenatal echocardiogram, Holter monitoring, and chest X-ray (Figure 3). In addition, the combination of prenatal ECG plus an additional prenatal cardiovascular diagnostic procedure compared to a prenatal ECG alone was associated with a further increased risk of postpartum depression (28 vs. 22 per 1000, p < 0.001).
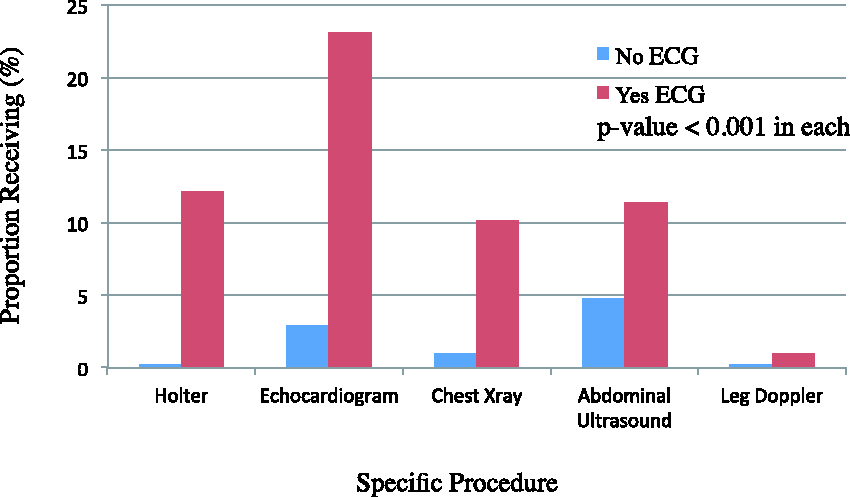
Additional diagnostic procedures. Absolute frequency of receiving additional prenatal diagnostic procedures among women who do or do not receive an ECG during prenatal care. X-axis shows specific diagnostic procedure of Holter monitor (codes G648 to G659, G682–G689), echocardiogram (G570, G571, G574, G575), chest X-ray (X090, X091, X092), abdominal ultrasound (J128, J135), and leg Doppler (J198). Y-axis shows proportion as percentage. Women who received an ECG during prenatal care indicated by red bar and remaining women indicated by blue bar. P value based on comparison of proportions in each procedure. Results show substantial frequency of additional prenatal diagnostic procedures for women who received an ECG during prenatal care.
Severity of outcome
We conducted additional analyses to examine the spectrum of postpartum depression by assessing indirect measures of disease severity. We found the association of ECG testing with postpartum depression extended to cases with many (>6) outpatient visits for depression treatment (5.5 vs. 2.7 per 1000, p < 0.001). Similarly, the association extended to cases with very many (>12) outpatient visits for depression treatment (1.4 vs. 0.7 per 1000, p < 0.001) and for cases with an acute care hospital admission for depression (4.2 vs. 1.9 per 1000, p < 0.001). The association also extended to a broader definition including other mental health diagnoses (159 vs. 103 per 1000, p < 0.001). In addition, the association extended to those who had a diagnosis of postpartum depression and died in the year following delivery, but the results were not statistically significant.
Discussion
We studied over three million pregnant women to assess whether an ECG test in pregnancy was associated with an increased risk of postpartum depression. The overall rate of ECG testing was about 1-in-20 and thereby far exceeded the baseline prevalence of heart disease in this demographic group.37,38 Compared to women who were not tested, women who received an ECG were at a one-third increased odds of postpartum depression after accounting for baseline predictors. The increased risk was further accentuated among pregnant women receiving additional cardiovascular procedures. In contrast, routine screening tests during pregnancy were not associated with a major increase in subsequent postpartum depression. Together, these findings suggest a possible link between physical and mental health.
One plausible explanation for the observed pattern of findings may be that somatic symptoms are a diagnostic clue to depression.39–42 For example, palpitations, dyspnea, and chest discomfort often prompt cardiovascular testing but can also be symptoms of a mood disorder.43–45 Adults who have underlying structural heart disease may also be prone to subsequently developing a secondary depression.46–48 Physicians, for example, may anticipate the prospect of a mood disorder and decide to obtain an ECG before initiating formal psychiatric care. This means the association does not necessarily indicate causality and, instead, signals the presence of a baseline predilection to depression.
A second explanation could be that ordering a cardiovascular test in pregnancy creates a form of anchoring bias in clinicians who, in turn, become distracted from inquiring about mood symptoms or psychosocial stressors. Instead, prenatal care thereafter focuses on cardiovascular concerns and further diagnostic assessments may dominate the clinical agenda. This interpretation suggests that some women may be suffering in silence, leading to a delay in referral to appropriate mental health services. 49 This is an important reminder for clinicians to consider mental health diagnoses in pregnancy, particular when workup for cardiac conditions reveals no specific diagnosis.
A further explanation is that diagnostic tests during pregnancy are prone to false positive findings or ambiguous results (as occurs with screening mammography).50–52 Cardiovascular disease may be present in 0.2 to 4% of women during pregnancy.37,38 Therefore, ECG testing is sometimes indicated for appropriate prenatal care, including for women with preexisting heart disease, anesthetic planning, work-up for chest pain, and evaluation of palpitations. However, ECG irregularities are common and ectopic abnormalities appear in over half of pregnant women investigated for palpitations.53,54 Unfortunately, normal results are not always reassuring and cascades of diagnostic procedures might ensue, as observed in our study.18,55 Together, the implication is that fallible diagnostic test results could be distressing for individuals who expect a normal pregnancy and are not accustomed to extensive medical investigations. 56 Furthermore, the process of investigating a false positive test result can be stressful for women.
Our study also supports past research on the psychologically mediated effects of medical testing. Diagnostic tests are sometimes ordered to satisfy individual expectations or strengthen a therapeutic relationship.57–60 However, qualitative studies have sometimes shown the opposite. 59 Individuals can become distressed while waiting for results or from a cascade of ensuing tests.59,61–66 A systematic review and meta-analysis of studies suggested that diagnostic tests for symptoms with a low risk of serious illness do not reassure all individuals or reduce anxiety.65,67 Moreover, some women may suffer damaged self-identity by being labeled with an illness.68,69
Our study has important limitations that merit emphasis. The study was not a randomized trial, and cannot establish how much of the association may reflect confounding from the indication for testing. To this end we have applied statistical analyses to adjust for variables such as preexisting heart disease, hypertension, and diabetes that might affect both the risk of postpartum depression and the likelihood of receiving an ECG.70–73 Regardless, the possibility of unmeasured confounders remain which might include tobacco smoking, alcohol consumption, substance misuse, domestic violence, and situational stress. This means an ECG could be a correlate or a marker of underlying comorbid illness, but not a contributor or cause of the increased risk of postpartum depression.
The lack of additional clinical information is important because our study detected only a modest association with ECG testing, far smaller than the association with a positive past history of depression.74,75 We also lacked information on other risk factors for postpartum depression including marital status, 76 intimate partner violence,70,77,78 breastfeeding challenges,79,80 psychological stress,81,82 and genetics.83,84 Furthermore, we did not have data on the concurrent management of depression including prescription medications, cognitive behavioral therapy, and prior electroconvulsive therapy. These uncertainties remain topics for future research.
Another further set of limitations in our research is that we may have failed to identify many women suffering from postpartum depression. The incidence of postpartum depression was measured using validated definitions that have imperfect specificity and sensitivity. The prevalence of postpartum depression is approximately 9% in North America, which is much higher than detected in our cohort. 85 This means our stringent definition may have missed many women who had a depressed mood, subclinical symptoms, or other psychiatric conditions. In addition, our study is based on one region in a high-income country that has free access to prenatal care and the findings may not apply elsewhere.
Conclusions
Our study identifies an association between prenatal ECG testing and postpartum depression, thereby highlighting a potential connection between physical symptoms and mental health in pregnancy. Physicians should be aware that cardiovascular symptoms may be a clinical clue to the presence of an underlying mood disorder in pregnant women that may become apparent postpartum.
Supplemental Material
sj-pdf-1-obm-10.1177_1753495X211012502 - Supplemental material for Prenatal electrocardiogram testing and postpartum depression: A population-based cohort study
Supplemental material, sj-pdf-1-obm-10.1177_1753495X211012502 for Prenatal electrocardiogram testing and postpartum depression: A population-based cohort study by Jonathan S Zipursky, Deva Thiruchelvam and Donald A Redelmeier in Obstetric Medicine: The Medicine of Pregnancy
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: JSZ has received fees for medicolegal opinions unrelated to the published work.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported by a Canada Research Chair in Medical Decision Sciences, the Canadian Institutes of Health Research, the University of Toronto, Department of Medicine Clinician Scientist Training Program, the Canadian Institute of Health Research Banting and Best Doctoral Award. The views expressed are those of the authors and do not necessarily reflect the Ontario Ministry of Health & Long-term Care. This study was supported by ICES which is funded by an annual grant from the Ontario Ministry of Health.
Ethical approval
The study protocol was approved by the Research Ethics Board at Sunnybrook Health Sciences Centre, including a waiver for patient consent. Parts of this material are based on data and information compiled by CIHI.
Informed consent
Written consent was obtained from the patient(s) for their anonymized information to be published in this article.
Guarantor
DAR
Contributorship
JSZ and DAR contributed to the concept and design of the study. Data extraction and statistical analysis were performed by DT and DAR. JSZ and DAR drafted the manuscript. All authors performed revision of the manuscript.
Acknowledgments
We thank the following individuals for insightful comments on specific points: Maria Cusimano, Allan Detsky, Michael Fralick, Cindy Kao, Fizza Manzoor, Sheharyar Raza, Raffi Rush, Sophie Grigoriadis, Sacha Bhatia, Wendy Levinson, and Steve Shumak.
Appendix 1. Mental health ICD9 codes.
300: Neurotic disorders (e.g., anxiety, hysteria, obsessive-compulsive disorders)
301: Personality disorders (e.g., paranoid personality disorder, affective personality disorder)
302: Sexual deviations and disorders (e.g., pedophilia, exhibitionism)
303: Alcohol dependence syndrome
304: Drug dependence (e.g., cocaine dependence, cannabis dependence, opioid dependence)
305: Nondependent abuse of drugs (e.g., alcohol abuse, cannabis abuse, cocaine type abuse)
309: Adjustment reaction (e.g., brief depressive reaction, prolonged depression reaction)
311: Depressive disorder, not otherwise classified
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.