
Abstract
Scant literature is available regarding pregnancy outcomes in women with Swyer-James-MacLeod syndrome, a rare obstructive lung disease. We present a case of a woman with this syndrome in pregnancy. Her baseline pulmonary function tests (PFT) demonstrated moderate airflow obstruction however she had excellent functional status and exercise tolerance. Her disease remained clinically stable in pregnancy. PFTs demonstrated slight worsening of her obstruction with forced expiratory volume in one second (FEV1). 59% and FEV1/FVC ratio 64%. She was diagnosed with gestational diabetes requiring metformin and insulin. Her labor and delivery was uncomplicated with vaginal delivery of a live male at term with no maternal respiratory complications. She did have a delayed postpartum hemorrhage requiring a D&C procedure. This case report demonstrates women with Swyer-James-MacLeod syndrome can have a successful pregnancy and need not avoid pregnancy if desired.
Introduction
Swyer-James-Macleod syndrome (SJMS), or unilateral hyperlucent lung syndrome, is a rare condition often arising from a childhood pulmonary infection, resulting in post-infectious obliterative bronchiolitis and obstructive lung disease. 1 Patients may be asymptomatic but more commonly present with recurrent pulmonary infections, bronchiectasis and symptoms of obstructive lung disease. 2 At a pathological level, this condition causes bronchiolitis and associated small airway obliteration, creating an emphysematous pattern with alveolar destruction and dilated lung parenchyma and a reduction of peripheral pulmonary vascularization in the affected area. 2 Chest imaging typically demonstrates lobar or unilateral hyperlucent lungs and pulmonary function tests show obstructive lung disease. There is a paucity of literature regarding cases of SJMS in pregnancy making counseling of pregnancy in these women challenging. We present a case of a successful pregnancy in a woman with this syndrome.
Case
A 29 year old woman in her first pregnancy was referred to our Maternal-Fetal Medicine/Internal Medicine joint clinic for prenatal care. Her pre-pregnancy Body mass index (BMI) was 28 kg/m2.
She was diagnosed with SJMS at age 22 by a respirologist. She had been admitted to hospital in her first year of life with a severe pneumonia, and subsequently was diagnosed with asthma. Throughout childhood, she had recurrent exacerbations of obstructive lung disease and respiratory infections requiring inhaled medications, antibiotics and systemic steroids. At age 22, her chest imaging demonstrated within the left lung patchy areas of mosaic attenuation consistent with SJMS. She was prescribed budesonide/formoterol and salbutamol inhalers, which she used infrequently pre-pregnancy. Her total IgE level and eosinophil counts were normal and therefore biologic therapy was not indicated. Her last chest infection was 2 years prior to pregnancy and resolved with antibiotics. Pre-pregnancy pulmonary function tests (PFTs) demonstrated oxygen saturation 97% on room air, FEV1 1.69L (54% predicted), and FEV1/FVC ratio 64%, consistent with moderate obstructive lung disease (Table 1).
Summary of pulmonary function tests throughout the pregnancy.
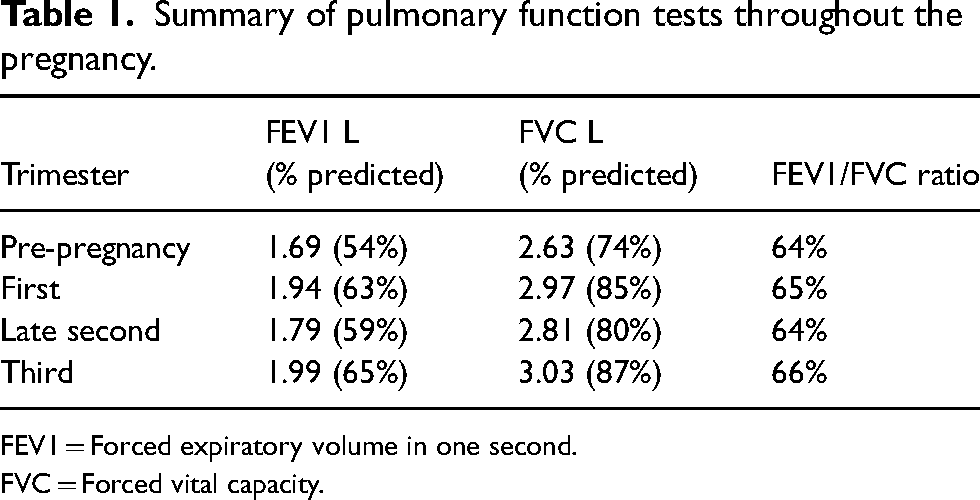
FEV1 = Forced expiratory volume in one second.
FVC = Forced vital capacity.
Her only other significant medical history was mild scoliosis, which has not required surgical intervention.
Her pregnancy progressed without complications. Baseline first trimester PFTs showed an of FEV1 1.94 L (63% predicted), and FEV1/FVC ratio 65% (Table 1). She reported improvement in her respiratory symptoms during pregnancy and did not require use of her inhalers. She was diagnosed with gestational diabetes (GDM) at 24 weeks and required metformin and insulin for glycemic control. Repeat PFTs at 29 weeks demonstrated FEV 1.79 L (59% predicted), and FEV1/FVC ratio 64% (Table 1). She remained asymptomatic from a respiratory perspective. Repeat PFTs at 34 weeks showed FEV1 1.99 L (65% predicted), and FEV1/FVC ratio 66% (Table 1).
She was encouraged to use her budesonide/formoterol and salbutamol inhalers regularly to optimize her respiratory status for the month prior to delivery. Ultrasound surveillance showed reassuring fetal status with estimated fetal weight of 2958 g (59th centile) at 36 weeks.
Due to the GDM, she underwent an induction of labor at 38 weeks of ARM and intravenous oxytocin. Given stability of her respiratory disease, we felt she was a candidate for vaginal delivery with no limitations on her second stage. We recommended an early epidural. She had an uncomplicated vaginal delivery of a live male with a birth weight of 3310 g and Apgars of at 8 and 9 minutes respectively. No maternal respiratory compromise occurred during her postpartum course.
At 2 weeks postpartum, she was readmitted with a delayed postpartum hemorrhage requiring a D&C to remove retained products of conception. No respiratory complications occurred during this procedure under a general anesthetic.
Discussion
SJMS is an acquired disease secondary to infectious bronchiolitis and pneumonitis in childhood.1,3 Patients may remain asymptomatic into adulthood and/or have been misdiagnosed with asthma similar to our patient. The incidence of SJMS in pregnancy is estimated at 1:2500. 4
There is a paucity of literature on SJMS in pregnancy with only one other available case report. 4 That woman was 30 years old with post-tuberculosis SJMS who similarly had moderate obstructive lung disease. Her pregnancy was complicated by pre-eclampsia requiring delivery at 34 weeks of gestation. Little is known of how physiologic changes to the respiratory system in pregnancy could affect individuals with SJMS. To develop our management plan, we extrapolated from published management of other obstructive lung diseases in pregnancy, in particular asthma.5,6 The majority of asthmatic women will have stable to improved control throughout a pregnancy; and pharmacotherapy is used to prevent acute exacerbations. 6 Literature about pregnant women with asthma supports monitoring for diminished pulmonary function, as this is associated with adverse pregnancy outcomes. 6 Thus, we obtained PFTs during each trimester. There was a slight drop in FEV1 in the second trimester of pregnancy with the FEV1/FVC ratio remaining stable in our patient; similar to how other obstructive lung diseases fair in pregnancy. 5
Complications of SJMS include recurrent pulmonary infections, lung abscesses, hypercapnia, pulmonary hypertension and pneumothorax. Fortunately, neither our case, nor the other reported case experienced infectious complications in pregnancy. 4 We postulate the relative stability of our patient‘s lung disease and symptoms through her pregnancy minimized the need for use of steroids and thus further mitigated the infectious risks of SJMS. Regardless, we recommend maintaining vigilant monitoring for symptoms of these complications in pregnancy. As she remained clinically stable, we did not perform routine blood gas sampling in our patient.
Pathological studies of chronic hyperlucent lung diseases have demonstrated SJMS patients have extensive pulmonary vascular damage. 7 Bronchiectasis itself has been demonstrated as a risk factor for placental disease.8,9 As lung damage from SJMS may contribute to maternal hypoxia thereby increasing the risk for placental insufficiency and pre-eclampsia, monitoring of maternal oxygenation through pregnancy is recommended, along with obtaining a third trimester growth scan for fetal surveillance.
In terms of delivery planning, similar to other moderate obstructive lung disease, it was felt vaginal delivery was a safe option. Early epidural for pain control in labor has been shown to reduce oxygen consumption and minute ventilation in the first and second stages of labor and is advocated for in women with respiratory disease. 10 Women with Obstructive lung disease typically would not have limitation on duration of valsalva; however it would be prudent to monitor for signs of maternal respiratory fatigue.
In summary, women with SJMS complicated by moderate obstructive lung disease can have a successful pregnancy without further deterioration in lung function. We recommend increased vigilance for respiratory infections, hypertensive diseases of pregnancy and fetal growth disturbances, along with a multidisciplinary approach to pregnancy care for optimal pregnancy outcomes for these women.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient for the publication of her case report.
Guarantor
CN.
Contributorship
OAB wrote the first draft. All authors reviewed and edited the manuscript and approved the final version.