
Abstract
Objectives:
This study examines alcohol consumption and smoking behaviors by pregnancy status and race/ethnicity in order to inform improved interventions designed to assist women of all races to avoid alcohol and tobacco use during pregnancy for their health and to prevent potential fetal exposure.
Methods:
This retrospective secondary data analysis utilized nationally representative National Health and Nutrition Examination Survey data between 2001 and 2018. Smoking and alcohol use were evaluated by race/ethnicity and pregnancy risk. Sexual behavior, reproductive health, and prescription drug use determined pregnancy risk, categorized as low pregnancy risk, at risk of becoming pregnant, and pregnant. Binary and multinomial multivariable logistic regression were used to examine associations.
Results:
The final sample consisted of 10,019 women of which 11.8% were Mexican American, 7.7% other Hispanic, 65.5% white, and 15% black (weighted percentages). White low pregnancy risk and pregnancy risk smoked most frequently in respective pregnancy risk groups (p < 0.001). Among pregnant women, smoking prevalence was highest among black women (14.0%, p < 0.01). Pregnancy risk women were more likely to smoke and pregnant women were less likely to smoke compared with low pregnancy risk. Low pregnancy risk and pregnancy risk Hispanics had a lower prevalence of binge drinking, but prevalence decreased less among pregnant Hispanics than other racial/ethnic groups. In adjusted analyses, pregnancy risk black women had more than 2 times the odds of combined smoking and alcohol consumption compared with low pregnancy risk black women.
Conclusion:
Women who may become pregnant need interventions and improved policy to prevent alcohol use and smoking. Culturally appropriate alcohol and smoking cessation interventions before pregnancy and improved contraception access are needed.
Introduction
In 2011, it was estimated that 45% of pregnancies in the United States were unplanned. 1 Unplanned pregnancies are an important consideration for maternal and child health and are more likely to occur among women who use substances, such as tobacco or alcohol.2,3 Alcohol consumption and smoking are common behaviors that contribute to poor maternal and newborn outcomes, which may result in health problems that persist across a lifetime. In utero alcohol exposure is the most common cause of nonheritable intellectual disability among children in the United States. 3 Smoking exposure contributes to stillbirth, premature birth, and low weight for gestational age. 2 Many studies have focused on alcohol use and smoking among pregnant women as a public health problem.
The Centers for Disease Control and Prevention (CDC) 4 recommended in 2016 that women of reproductive age refrain from consuming alcohol unless they are using effective contraception. The American College of Obstetricians and Gynecologists 5 also recommends that providers should strongly advise women at risk of becoming pregnant or who are pregnant to abstain from alcohol use, provide treatment if needed, and provide contraception for those who need assistance with abstaining. The U.S. Preventive Services Task Force 6 recommends screening for risky alcohol use in all adult patients and for providers to recommend alcohol abstention among women contemplating pregnancy and among pregnant women. More needs to be known about the use of alcohol or smoking among sexually active reproductive-aged women who are not using contraception, as they may be at risk of tobacco- or alcohol-exposed pregnancy. While many women stop using tobacco and alcohol when they become aware of their pregnancy, some may not know they are pregnant during the critical early weeks during which exposure may occur.
As of 2007, a national US survey on drug and alcohol use indicated that prevalence of alcohol use was higher among whites compared to Hispanics and blacks while Hispanics and blacks had similar rates of alcohol consumption in the past 30 days. 7 Despite overall lower rates of alcohol use in these groups, black and Hispanic women are less likely than white women to reduce alcohol consumption during pregnancy. 8 According to nationally representative data from the CDC, 9.9% of white women reported drinking alcohol in the past 30 days and 4% reported binge drinking in the same period while 13.7% of pregnant black women reported any alcohol use and 7.2% reported binge drinking in the past 30 days in the United States between 2015 and 2018.9,10 Black and Hispanic women have lower treatment completion rates during pregnancy, which may explain some differences between population averages and consumption among pregnant women. 11 Although treatment among those who consume tobacco or alcohol and become pregnant is important, prevention of tobacco and alcohol-exposed pregnancies during the pre-conception period is a preferable strategy to reduce risks associated with tobacco and alcohol use during pregnancy.
The purpose of this study is to examine differences in alcohol consumption and smoking behaviors by risk of pregnancy across time and by race/ethnicity. The results from this study may be used to evaluate how well national public health campaigns have worked in the past and to inform intervention efforts moving forward.
Methods
This retrospective secondary data analysis utilized National Health and Nutrition Examination Survey (NHANES) data, which is a nationally representative survey and in-person medical evaluation administered in 2-year cycles. NHANES data for this study were collected across nine cycles between 2001 and 2018. 12 These data were collected by the CDC through home interviews and mobile examination centers for biomedical data. Although other data sources have more detailed information about alcohol, tobacco, and other substance use, NHANES has detailed information about reproductive health and sexual behaviors. The survey was approved by the National Center for Health Statistics (NCHS) 12 ethics review board (protocol 2005–2006 and 2011–2017), and the data used for this study are publicly available. All participants provided consent at the time of survey.
Demographics
For this study, we selected all 20- to 44-year-old females who identified as Mexican American, Hispanic, white, or black. The category “Other Race” was excluded due to low sample size. We excluded women under the age of 20 because the sexual behavior data for those women were restricted from public use. Analyses on Mexican Americans were conducted separately from the Hispanic category as recommended by the NHANES study documents to appropriately use study sample weights. The original NHANES education level variable was recoded into three categories, less than a high school diploma/GED, received a high school diploma/GED, and attended some college or college graduate. The age variable was divided into five categories: 20–25, 26–30, 31–35, 36–40, and 41–44. A time variable that included 3 time points equal to three combined cycles, each representing a 6-year period, was developed to better observe shifts in behavior across time. We considered including parity, but this variable was not measured consistently across all cycles.
Smoking and alcohol use
Current smoking status was evaluated, with those who reported smoking 100 cigarettes in their lifetime and reported they currently smoked cigarettes counted as current smokers, consistent with previous research on smoking. Those who reported they were not a current smoker were considered non-smokers. A variable that estimated alcohol consumption was created to describe the level of alcohol use in the past year. Participants who reported consuming 0 to less than 12 alcoholic drinks per year were included in the category “infrequent.” Participants who reported consuming 12 to 52 alcoholic drinks per year were considered to have “moderate” alcohol intake, and those who reported consuming more than 52 alcoholic drinks per year were considered to have “regular” alcohol intake. Binge drinking was defined as women who reported consuming four or more drinks in 1 day during the past year.
A combined smoking and alcohol use variable was developed to examine the simultaneous use of both tobacco and alcohol. The first level of this variable included individuals who were not current smokers and drank < 12 servings of alcohol per year. The second level included individuals who were either current smokers or consumed ⩾ 12 servings of alcohol per year. The third level included individuals who were both current smokers and consumed ⩾ 12 servings of alcohol per year. We chose the cutoff of 12 servings per year for alcohol consumption as we wanted to examine the combination of even low levels of alcohol use in combination with smoking in order to capture even lower levels of alcohol use combined with smoking in each pregnancy risk category.
Pregnancy risk
Pregnancy risk was determined using responses to questions about sexual behavior, reproductive health, and prescription drug use. Individuals were considered currently sexually active if they reported having more than 0 sexual partners in the past year or if they reported having any kind of sex with a male in the past year. Current birth control use was determined using data from respondent prescription drug files. Those with no information in the prescription drug files indicating use of contraception, but who reported using contraception (not including condoms) in the reproductive health questionnaire were determined to be contraception users. To determine PR, we developed three categories. Participants who were not sexually active in the past year, had never had sex, were currently using birth control, or reported having a hysterectomy or oophorectomy were categorized in the “low pregnancy risk” (LPR) group. We categorized women with no risk and low risk together in this group (LPR group), as splitting these two groups would make them too small for comparison. Participants not currently taking birth control and who were sexually active in the past year were included in the “pregnancy risk” (PR) group. Women with positive urine pregnancy tests and those who did not take the urine pregnancy tests, but reported they were pregnant, were included in the “pregnant group.”
Statistical analyses
Data were weighted to account for non-response, and other techniques were used consistent with the NHANES documentation to develop estimates representative of the entire civilian non-institutionalized population of the United States. 12 The prevalence of smoking and drinking behaviors by race and time for each PR level was calculated. Rao Scott chi-square tests were done to determine the statistical significance of the relationship between substance use and race or time. Binary and multinomial multivariable logistic regressions calculated unadjusted and adjusted odds ratios (aORs). Moderation effects were determined by evaluating possible interactions between pregnancy status and ethnicity for alcohol use, current smoking status, and combined smoking and alcohol use with final models stratified if significant interactions were found. aOR were calculated after controlling for race, age, education level, and PR. All analyses were conducted using R (R Foundation for Statistical Computing, Vienna, Austria. URL https://www.R-project.org/).
Results
For this study, the final sample size was 10,019 (Table 1). Weighted prevalence of each racial/ethnic group was 11.8% Mexican American, 7.7% other Hispanic, 65.5% white, and 15% black. Most women in each age group were in the PR group (65.2% among 20–25-year-olds to 79.5% among 36–40-year-olds). The prevalence of women in the pregnant group decreased with increasing age, from 8.3% among 20–25-year-olds to less than 1% among 41–44-year-olds. The highest proportion of currently pregnant women were Mexican American, followed by 6.4% of black women. PR varied by education level. Only 70% of respondents with some college were in the PR group as compared to 78% of those with a high school education and 78% of those with less than a high school education (p < 0.001). Alcohol use was lowest among pregnant women. The proportion of women who reported regular alcohol consumption (> 52 drinks/year) was highest among the PR group (68.4%) followed by the LPR group (29.2%). However, the proportion of women reporting regular alcohol use in the LPR group was more frequent than women who reported infrequent alcohol use in the LPR group (21.5%). The alcohol use pattern was opposite among the PR (68.4% regular user versus 71.5% infrequent users) and pregnant groups (2.4% regular user and 7.0% in infrequent users). Only 2.4% of current smokers were pregnant, compared to 6.2% of non-smokers. A high frequency of current smokers was in the PR group (78.9%) compared to non-smokers (71.4%).
Characteristics of 20–44-year-olds, NHANES 2001–2018 (N = 10,019).

GED: general educational development.
w%: weighted percent; 95% CI: 95% confidence interval; LPR: participants who were not sexually active in the past year, had never had sex, were currently using birth control, or reported having a hysterectomy or oophorectomy; PR: participants not currently taking birth control and who were sexually active in the past year; Pregnant: women with positive urine pregnancy tests and those who did not take the urine pregnancy tests, but reported they were pregnant.
Total column calculated as column percents. **PR columns calculated as row percents.
Smoking prevalence
The prevalence of current smokers decreased overall among the LPR group and PR group (Figure 1). However, prevalence of smoking was stable, but had a very slight increase in prevalence of current smokers across time among pregnant women. Low alcohol use (< 12 drinks per year) decreased across time among both LPR and PR groups (Supplemental Figure 1). Pregnant women, however, had a strong increase in prevalence of infrequent alcohol use, from 51.6% in 2007–2012 to 67.1% in 2013–2018. The prevalence of women who reported moderate alcohol intake remained stable among women in the LPR and PR groups but decreased from 32.8% of pregnant women in 2001–2006 to 20.8% in 2013–2018.

Prevalence of current cigarette use by PR category across time (N = 10,019).
The frequency of smokers was highest among white women in the LPR (22.2%) and PR groups (29.7%, p < 0.001; Supplemental Figure 2). However, among pregnant women, smoking prevalence was highest among black women (14.0%, p < 0.01). After adjusting for potential confounders, black and Hispanic women had significantly lower odds of smoking compared to white women (Table 2). Those with less than a high school education had more than 4 times higher odds of smoking compared to women with some college. We found that women in the PR group were more likely to be smokers compared to women in the LPR group. However, pregnant women were much less likely to be smokers than the LPR group.
Multivariable binary logistic regression describing current cigarette use by PR by race/ethnicity (N = 10,019).

GED: general educational development.
Bolded values indicate significance at p < 0.05. aOR: odds ratio adjusted for all variables in table; 95% CI: 95% confidence interval; LPR: participants who were not sexually active in the past year, had never had sex, were currently using birth control, or reported having a hysterectomy or oophorectomy; PR: participants not currently taking birth control and who were sexually active in the past year; Pregnant: women with positive urine pregnancy tests and those who did not take the urine pregnancy tests, but reported they were pregnant.
Alcohol use prevalence
Among LPR and PR groups, the highest frequency of regular alcohol consumption occurred among white women (25.5% and 21.6%, respectively). A similar frequency of pregnant women from each racial/ethnic group was regular alcohol consumers (p > 0.05). After adjusting for confounding variables, non-white women had lower odds of moderate or regular alcohol consumption compared to white women (Table 3). Pregnant women had lower odds of reporting moderate or regular alcohol consumption compared to women in the LPR group. Women in the PR group had lower odds of moderate alcohol consumption. Although the aOR in the same group was less than 1 for regular alcohol consumption, it was not significantly different from LPR women.
Multivariable multinomial logistic regression describing alcohol intake by PR (N = 10,019).

GED: general educational development.
Bolded values indicate significance at p < 0.05. aOR: odds ratio adjusted for all variables in table; 95% CI: 95% confidence interval; LPR: participants who were not sexually active in the past year, had never had sex, were currently using birth control, or reported having a hysterectomy or oophorectomy; PR: participants not currently taking birth control and who were sexually active in the past year; Pregnant: women with positive urine pregnancy tests and those who did not take the urine pregnancy tests, but reported they were pregnant.
Comparison level is infrequent (< 12 alcoholic drinks per year) alcohol intake. Moderate intake = 12–51 alcoholic drinks/year. Regular intake = 52 + alcoholic drinks/year.
A high prevalence of women reported binge drinking in the LPR and PR groups (Supplemental Figure 3). The highest prevalence occurred among white women in LPR and PR groups (40.9% and 39.0%, respectively) which dropped to 25.7% among currently pregnant white women. However, although Hispanic women had a lower prevalence of binge drinking among LPR and PR groups, the prevalence dropped less among pregnant Hispanics and exceeded the prevalence of white women slightly (26.8% versus 25.7%, p < 0.05). The greatest decrease in prevalence of binge drinking behavior occurred among black LPR (17.9%) and black PR (22.2%) to 11.7% among pregnant black women.
Combined smoking and alcohol consumption prevalence
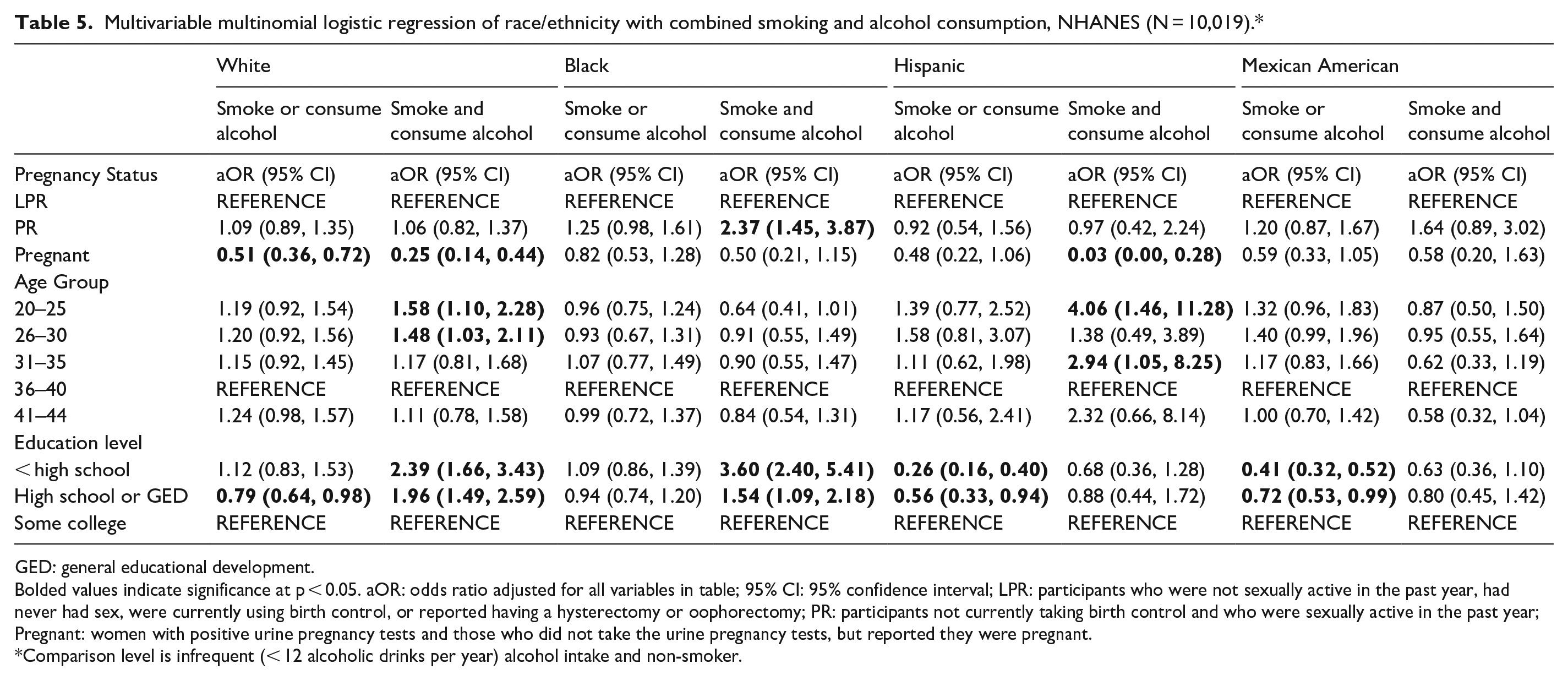
In an analysis of combined smoking and alcohol use by pregnancy risk category (Table 4), models were stratified by pregnancy risk category as interactions were significant in moderation analyses (results not shown). Black and Hispanic women in all PR categories were less likely to either smoke or consume alcohol compared to white women. Black and Hispanic women were also less likely to report combined smoking and alcohol consumption. Within each racial/ethnic category, pregnant women were significantly less likely to smoke and/or be moderate to regular alcohol consumers, except for pregnant black and Mexican American females (Table 5). The aOR for those two groups are in the expected direction-having lower odds of engaging in one or both behaviors, but they are not significantly different from women of their respective race/ethnicity in the LPR group. No significant differences in combined smoking and alcohol consumption between the PR and LPR groups were found within white and Hispanic ethnicities. However, black women in the PR group had more than 2 times the odds of both smoking and consuming alcohol compared to black women in the LPR group.
Multivariable multinomial logistic regression of PR with combined smoking and alcohol consumption, NHANES (N = 10,019).*

GED: general educational development.
Bolded values indicate significance at p < 0.05. aOR: odds ratio adjusted for all variables in table; 95% CI: 95% confidence interval; LPR: participants who were not sexually active in the past year, had never had sex, were currently using birth control, or reported having a hysterectomy or oophorectomy; PR: participants not currently taking birth control and who were sexually active in the past year; Pregnant: women with positive urine pregnancy tests and those who did not take the urine pregnancy tests, but reported they were pregnant.
Comparison level is infrequent (< 12 alcoholic drinks per year) alcohol intake and non-smoker. Moderate intake = 12–51 alcoholic drinks/year. Regular intake = 52 + alcoholic drinks/year.
Multivariable multinomial logistic regression of race/ethnicity with combined smoking and alcohol consumption, NHANES (N = 10,019).*
GED: general educational development.
Bolded values indicate significance at p < 0.05. aOR: odds ratio adjusted for all variables in table; 95% CI: 95% confidence interval; LPR: participants who were not sexually active in the past year, had never had sex, were currently using birth control, or reported having a hysterectomy or oophorectomy; PR: participants not currently taking birth control and who were sexually active in the past year; Pregnant: women with positive urine pregnancy tests and those who did not take the urine pregnancy tests, but reported they were pregnant.
Comparison level is infrequent (< 12 alcoholic drinks per year) alcohol intake and non-smoker.
Discussion
Although racial and ethnic minorities have lower prevalence of alcohol consumption and smoking overall, the prevalence does not decrease as much during pregnancy compared to white women who are currently pregnant. These results, in combination with other findings, indicate there may not be adequate support for cessation among ethnic minorities during pregnancy in the United States. A previous study found that pregnant black and Hispanic women were less likely to complete treatment programs for alcohol consumption than white women. 11 Due to the fact that black and Hispanic women are prosecuted for substance use at disparately higher rates compared to white women, these results possibly reflect the fear of loss of child custody as a result of treatment during pregnancy. 13 Another possible cause of treatment cessation is a lack of culturally tailored programs that work for women from various ethnic or socioeconomic backgrounds. One program focused on prevention of alcohol-exposed pregnancy was successful at preventing pregnancy among Hispanic women who were proficient in English but was less successful among those who preferred study materials in Spanish. 14
Trends over time show an important decrease in cigarette use by women at low risk and at risk of pregnancy. However, more prevention focused on smoking cessation during pregnancy is needed to reduce stagnating prevalence rates among pregnant women across time. Important targets for interventions include women with high school education or less, in addition to women from minority ethnic backgrounds. Our study showed that black and white women were more likely to engage in both smoking and alcohol consumption if they had a high school degree or less, which is reversed from the association observed among Hispanic and Mexican American women. Health literacy and culture may play a role in these observations. However, there are likely more considerations that could impact smoking cessation, such as psychological health and socioeconomic status, 15 which may also be associated with education level.
Although non-pregnant women from historically marginalized ethnic groups have lower prevalence of smoking, smoking prevention should be offered to those who do smoke during pregnancy. Women in these groups are at higher risk of poor outcomes associated with smoking, such as increased risk of premature labor and small for gestational age babies, regardless of smoking status.16–18 Furthermore, black women may be less likely to quit smoking spontaneously compared to white women after becoming pregnant, even if they perceive a risk to their fetus. 19 Women need a strong individualized support system with a variety of non-judgmental options to support smoking cessation during pregnancy. 20 Resources to support these needs may be particularly difficult for marginalized communities to access. The situation may be further complicated by the need for postpartum smoking interventions to improve abstinence, such as continued support and counseling for smoking cessation for postpartum women and programs for partners who smoke. 21 In particular, depression is associated with increased risk of smoking and less support for cessation among black women. 22 Pregnant black women experience increased levels of stress and depression compared to white women. 23 Without addressing these factors in addition to providing smoking cessation services, it is possible that efforts will be less effective in this group.
Alcohol use was much lower among pregnant white women compared to other PR groups. Although black, Hispanic, and Mexican American women had lower prevalence of alcohol consumption in LPR and PR groups compared to white women in the same groups, alcohol consumption in these ethnic groups was similar to white women during pregnancy. Mexican American women did not experience a decrease in alcohol use when pregnant compared to those at low or risk of pregnancy. Programs such as CHOICES Plus, a program developed to prevent alcohol and tobacco exposed pregnancies by the CDC, may reduce the risk of alcohol and tobacco exposed pregnancy through reducing alcohol and tobacco consumption in addition to offering effective contraceptive choices among women at risk of unintended pregnancy. 24 However, more work needs to be done to improve the ability of successful programs to be adapted to different cultures to improve their ability to address these topics among minority women.
Particularly concerning results of this study were the increased odds of combined smoking and drinking among women at risk of pregnancy compared to those with low risk of pregnancy. This was most notable among black women, who had more than 2 times the odds of combined smoking and alcohol use if they were in the PR group compared to black women in the LPR group. Combined smoking and alcohol use are particularly harmful, as they affect different mechanisms important for a healthy pregnancy and the combined effects may have a synergistic effect on risk of poor pregnancy outcomes. 25 The combination of smoking and alcohol use may be associated with increased odds of preterm birth, low birth weight, and fetal growth restriction compared to the use of either alcohol or tobacco use alone. 25 However, some research indicates that the effects of both substances are not synergistic. 26 Polysubstance cessation treatment should still be offered to these women in order to leverage the motivation women have to reduce tobacco and alcohol use and continuing support to help reduce the risk of relapse should also be part of any successful program. 27
Limitations
Our estimates of women who were at risk for pregnancy are higher than estimates of 57.4% to 76.8% of women in much of the United States who were considered at risk for unintended pregnancy in 2016. 28 However, we were unable to determine whether some participants wanted to become pregnant, which had been removed from previously published analyses. This may have contributed to more conservative estimates in this study. NHANES questions for determining sexual activity asked about behaviors in the past year and were not specific to vaginal sex. All behaviors were self-reported and may have reflected a social desirability bias among respondents. This could have made our estimates more conservative.
Conclusion
Women who may become pregnant need more public health efforts to prevent alcohol use and smoking, particularly those from historically marginalized ethnic groups and those without a college education. Considerations for prenatal cessation treatment should include partner cessation programs, postpartum support, and social support groups that aim to reduce relapse and decrease stress. Increasing culturally appropriate alcohol and smoking cessation interventions before pregnancy as well as improving access to contraception to reduce unintended pregnancies are likely to contribute to reducing some poor maternal and neonatal outcomes experienced as a result of prenatal exposure to alcohol and tobacco. In addition, reducing punitive policy to eliminate repercussions for seeking prenatal and postnatal cessation treatment should be considered to improve success in decreasing disparities in prenatal exposure to smoking and alcohol.
Supplemental Material
sj-docx-1-whe-10.1177_17455057221112188 – Supplemental material for Racial/ethnic variations in alcohol and cigarette use by pregnancy status among 20- to 44-year-old women, NHANES 2001–2018
Supplemental material, sj-docx-1-whe-10.1177_17455057221112188 for Racial/ethnic variations in alcohol and cigarette use by pregnancy status among 20- to 44-year-old women, NHANES 2001–2018 by Jacqueline M Hirth, Catherine Valadez, Sandra Gonzalez, Alicia Kowalchuk, Judith A Gutierrez and Roger Zoorob in Women’s Health
Footnotes
Author contribution(s)
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Department of Health and Human Services, Health Resources and Services Administration (Grant number T32 HP10031).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.