
Abstract
Pregnancy-associated haemophilia A is an uncommon, acquired bleeding disorder which usually presents post-partum; very rarely it may present during pregnancy. No consensus guidelines exist on the management of this condition in pregnancy and very few cases have been reported in the literature. Here we describe the case of a woman presenting with acquired haemophilia A during pregnancy and outline the management of her bleeding disorder. We contrast her case with that of two other women, presenting to the same tertiary referral centre, with acquired haemophilia A presenting post-partum. These cases highlight the heterogeneous management of this condition and how it may be successfully managed in pregnancy.
Introduction
Acquired haemophilia A (AHA) is a rare bleeding disorder caused by autoantibodies against factor VIII (FVIII). 1 Fewer than 5% of AHA cases are associated with pregnancy, affecting 1:350 000 births and typically occurring 1–4 months postpartum. 2 It is even rarer for AHA to present during pregnancy; the largest case series of post-partum AHA women described only 1 case diagnosed in pregnancy (2% of cases in the EACH2 registry). 2 We present a woman with AHA diagnosed in pregnancy and compare this with two women diagnosed postpartum presenting to a single haemophilia centre in a 6-month period.
Case 1: AHA diagnosed in pregnancy
A 24-year-old woman, at 9 weeks' gestation with her third child, presented with a 12-week history of easy bruising and a prolonged activated partial thromboplastin time (APTT) 47.4 s (normal range 20–30 s). This pregnancy occurred 10 weeks after the birth of her second child. The prior pregnancy was uncomplicated; she gave birth by spontaneous vaginal delivery with a postpartum haemorrhage of 700 mls; the infant had no bleeding symptoms. In her first pregnancy, neither she nor her child had issues with bleeding.
Tests confirmed AHA with a low FVIII level and a positive FVIII inhibitor screen (Table 1). She started prednisolone 0.5 mg/kg once daily, a reduced dose to minimise side effects. Retrospective review of an 8-week scan revealed a small retroplacental bleed. A repeat scan at 10 weeks demonstrated semi-resolution, and intervention was not required. FVIII levels normalised 4 weeks after starting treatment. Her prednisolone was weaned from 20 weeks’ gestation and she continued low dose throughout pregnancy. Routine CTG monitoring at 38 weeks identified pathological abnormalities and an emergency caesarean delivery was therefore required. This was performed without complication and no excessive blood loss. Her FVIII levels pre-delivery were 4.46 IU/ml with an undetectable inhibitor level. She did not require any additional haemostatic support. The baby had no haemorrhagic complications and weighed 2.81 kg (9th centile). Cord blood confirmed the newborn's FVIII 1.22 IU/ml with no detectable inhibitor. The woman completed her steroid wean 35 weeks after diagnosis and remains asymptomatic 11 months post-delivery.
A comparison of the three women at presentation.
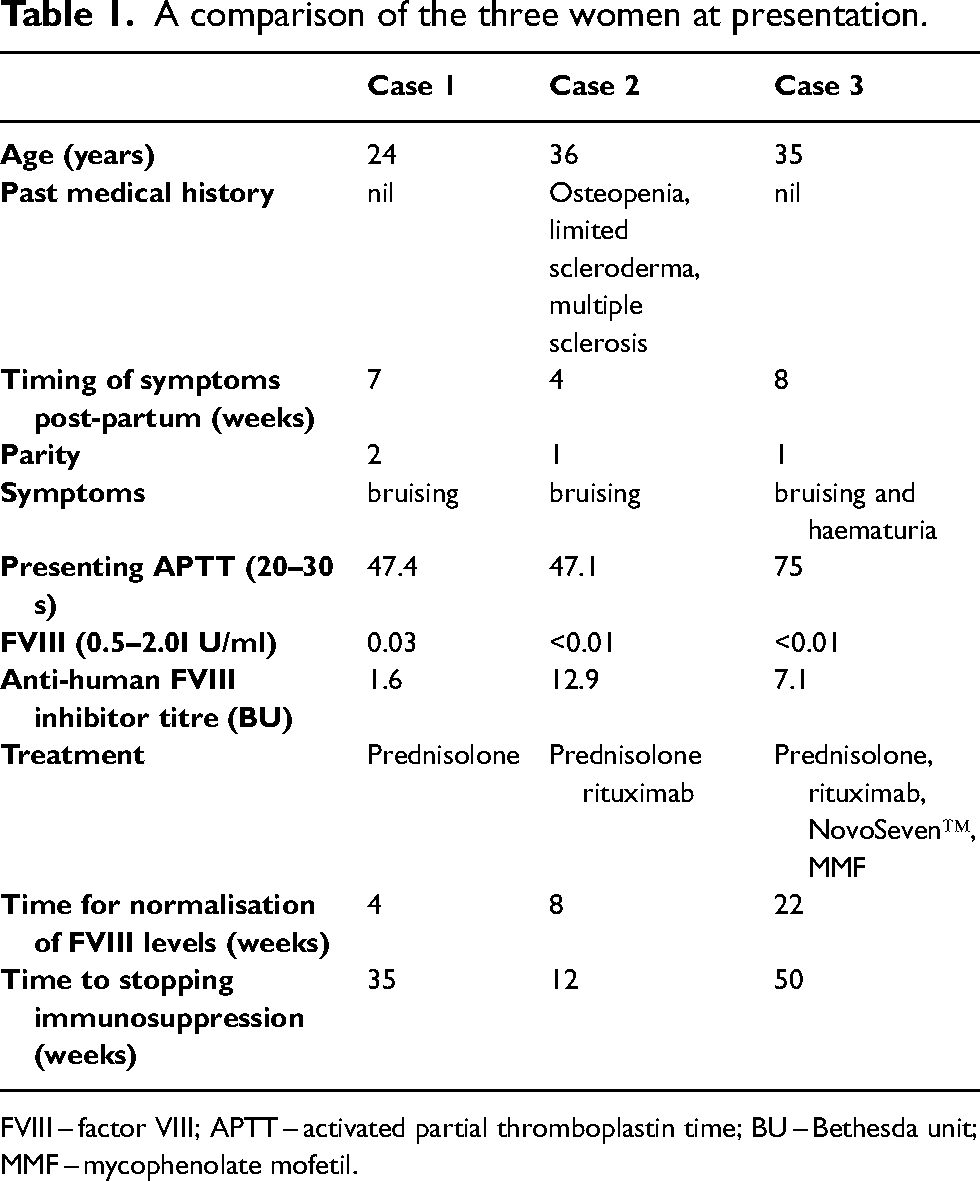
FVIII – factor VIII; APTT – activated partial thromboplastin time; BU – Bethesda unit; MMF – mycophenolate mofetil.
Cases 2: AHA diagnosed post-partum
A 36-year-old woman had an uncomplicated pregnancy and gave birth to her first child by vaginal delivery. Four weeks postpartum she noticed bruising. Tests confirmed AHA (Table 1). She had a past history of osteopenia, limited scleroderma and multiple sclerosis. She was treated with 1 mg/kg prednisolone, calcium/vitamin D and bisphosphonates (she was not breastfeeding). After five weeks FVIII remained 0.01 IU/ml, and she was diagnosed with a vertebral fracture. She was started on rituximab (375 mg/m2) weekly for four weeks and her steroids were rapidly weaned. Her FVIII levels responded well to rituximab and normalised 8 weeks after starting treatment. She did not receive any factor VIII replacement. She remains in complete remission 18 months after completing immunosuppression.
Case 3: AHA diagnosed post-partum
A 35-year-old nulliparous woman had an uncomplicated vaginal delivery. She had an episiotomy and bled, requiring a transfusion. Two months postpartum she developed a painful forearm bruise. Blood tests confirmed AHA (Table 1). She was treated with prednisolone 80 mg (1 mg/kg) daily. After 6 weeks she developed spontaneous bruising. She commenced rituximab (375 mg/m2) weekly for four weeks and weaned her prednisolone. Five weeks after finishing rituximab she developed loin pain and frank haematuria. She was treated with a bypassing agent, recombinant FVIIa, (NovoSeven™, 90 mcg/kg). Her haematuria resolved. FVIII remained low (0.02 IU/ml) and so mycophenolate mofetil was started (500 mg twice daily, increased to 1 g twice daily). After 17 days the bruising had resolved (FVIII 0.23 IU/ml). FVIII levels normalised 22 weeks after starting treatment. She stopped immunosuppression 50 weeks after diagnosis. She remains in remission (FVIII 0.70 IU/ml, with no detectable FVIII inhibitor).
Discussion
This case series describes AHA management during pregnancy and post-partum. Case 1 was diagnosed at 9 weeks' gestation in third pregnancy (and 19 weeks post-partum for second pregnancy). Given she had a 12-week history of easy bruising at diagnosis, this most likely represents post-partum AHA diagnosed in a subsequent pregnancy. The case highlights the nuances of treating AHA in a pregnant woman and, compared to other cases, this woman had a shorter disease course with rapid achievement of remission and no requirement for second-line immunosuppression.
There are few published cases of AHA diagnosed and managed in pregnancy. A recent systematic review included data on 174 pregnancy-associated AHA cases, with only 10 cases diagnosed antepartum (5.7%). 3 Retrospectively, an additional 14 women had evidence of AHA on antepartum blood tests but were diagnosed and started on treatment post-partum. The review showed that outcomes were similar between those diagnosed post-partum and those diagnosed antepartum. 3 There is a paucity of data on the management of antepartum AHA, with the evidence largely based on small numbers in published cohorts and case studies.4–6
Women with AHA are typically treated intensively to reduce bleeding risk. Case 1 showed a rapid improvement in FVIII levels with 0.5 mg/kg prednisolone. This can be considered for other women with AHA during pregnancy. 3 Consideration must be given to potential harm to the infant. Steroids can be found in breastmilk, although at concentrations unlikely to affect the infant. 7 Concurrent vitamin D and calcium supplementation is vital in pregnancy/lactation 8 and monitoring for hypertension and gestational diabetes is also advised. 3
Second-line options in pregnancy are limited. Fortunately, our patient responded to steroids alone. Rituximab given during pregnancy is associated with fetal lymphopenia and neonatal infections. 9 However there is growing evidence that rituximab can be safely used in pregnancy where the benefits outweigh the potential risks. 10 Women can safely breastfeed while receiving rituximab as secretion into breastmilk is low and oral bioavailability poor. 11
In conclusion, this case series describes the rare case of AHA presenting in pregnancy and compares this with two postpartum cases. The postpartum cases had slow recovery of FVIII requiring additional lines of immunosuppression. Although pregnancy-related AHA is rare, it is an important diagnosis to consider in pregnant and post-partum women presenting with bleeding.
Footnotes
Acknowledgements
We would like to thank our women. We would also like to thank Peter Baker, James Beavis and Sarah Harper for running the laboratory assays, and Sayma Raza-Burton and Vicky Minty for their nursing care of the patients.
Author contributions
A. Ejaz, F.A. Sharpley, and C. O’Doherty co-wrote the manuscript. M. Desborough revised the manuscript. M. Desborough, N. Curry, S. Shapiro were involved in management decisions and provided critical input to the manuscript. All authors approved the final version. Susan Shapiro receives funding support from the Medical Research Council (MR/T024054/1). Nicola Curry receives funding support from the Medical Research Council (MR/ T023961/1). The views expressed are those of the authors and not necessarily those of the NHS, nor, of the Department of Health.
Informed consent
Verbal informed consent obtained.
Guarantor author
The author who will guarantee the manuscript's accuracy and the contributorship is Dr Michael J R Desborough.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: MD has received speaker fees and/or consultancy from Takeda, Portola and Pfizer. SS has received meeting sponsorship, speaker fees and/or consultancy from Bayer, Pfizer, NovoNordisk, Sobi. Chugai/Roche and Shire/Takeda. NC has received two CSL Behring investigator led grants, educational advisory board fees from LFB and Bayer; conference support from Bayer, NovoNordisk, CSL Behring, and Sobi; speaker fees from Sobi. The other authors have no disclosures to declare.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.