
Abstract
Background/objectives:
There is limited research on the associated immediate and long-term outcomes of postpartum hemorrhage. Mothers with a pre-existing psychiatric disease prior to delivery may be especially vulnerable to postpartum hemorrhage outcomes but little is known on this topic. Barriers to studying this population exist and add to knowledge gaps. The goal of this study is to determine the clinical characteristics and frequency of complications within 1 year of a postpartum hemorrhage diagnosis and the psychiatric sequelae within 7 days of a postpartum hemorrhage diagnosis in mothers with a pre-existing mental health diagnosis prior to delivery versus those without.
Methods/design:
This is a multicenter retrospective observational cohort study using TriNetX, a de-identified electronic health record database. The following electronic health record data were collected and evaluated in postpartum females who were billed for either a vaginal or cesarean delivery: age, race, ethnicity, diagnostic codes, medication codes, and number of deaths.
Results:
We included 10,649 subjects (6994 (65.7%) no mental health diagnosis and 3655 (34.3%) pre-existing mental health diagnosis). Haloperidol administration (118 (3.2%) versus 129 (1.8%), p < 0.001) was more prevalent in subjects with a pre-existing mental health diagnosis. Adjusting for demographics, pre-existing mental health diagnoses were associated with complications within 1 year after postpartum hemorrhage diagnosis (OR = 1.39, 95% CI: 1.26–1.52, p < 0.001).
Conclusion:
Having a mental health disorder history is associated with a higher odds of developing subsequent complications within 1 year of postpartum hemorrhage diagnosis. Mothers with a pre-existing mental health disorder have a significantly higher frequency of certain severe postpartum hemorrhage sequelae, including acute respiratory distress syndrome, retained placenta, sickle cell crisis, and need for mechanical ventilation/tracheostomy up to 1 year after delivery. Medications such as haloperidol were ordered more frequently within 7 days of a postpartum hemorrhage diagnosis in these mothers as well. Further research is needed to understand and manage the unique consequences of postpartum hemorrhage in this vulnerable maternal population.
Introduction
Despite the fact that roughly 14 million women worldwide experience postpartum hemorrhage (PPH) each year, 1 much of PPH research focuses on risk factors, prevention, and management. 2 Less of an emphasis has been placed on the associated outcomes of PPH. A recent review noted that of 2210 papers on PPH, only 6 focused on outcomes and 1 focused on emotional sequelae. 2 The National Institute for Health and Care Excellence considers PPH to be physical birth trauma. 3 Reframing the understanding of PPH as an experience with both “in the moment” and “after-effects” may help highlight the significance of outcomes, both immediate and long term.3,4 The “in the moment” consequences include severe anemia, acute kidney injury, hepatic failure, adult respiratory distress syndrome, pituitary infarction, blood product transfusions, surgical procedures, or death.5 –8 The “after-effects” may include fear of dying or anxiety in subsequent pregnancies and may develop or continue many years after the PPH experience. 2 Although a large cohort study conducted in Sweden did not specifically show an association between PPH and postpartum depression, study design limitations may have influenced these results. 9 Research on birth trauma indicates that these experiences can have lasting emotional impacts, 4 such as postpartum depression, birth-related post-traumatic stress disorder, or anxiety from simply surviving a life-threatening event.10 –12 If not recognized or left untreated, these psychiatric sequelae can impact bonding, breastfeeding, or may result in infanticide or maternal death from suicide or substance overdose.10,13
Mothers with a pre-existing psychiatric disease prior to pregnancy or delivery may be especially vulnerable after experiencing PPH. These mothers can have poor obstetrical outcomes14,15 or have higher risks of postpartum psychiatric symptoms16 –18 and less is known about how PPH specifically affects this population. There may be barriers to studying mothers with pre-existing psychiatric conditions, such as under-diagnosis of peripartum psychiatric disorders 19 or the challenges associated with conducting research on patients with acute psychiatric emergencies, 20 which adds to the knowledge gap in this space. Scant treatment guidelines for severe psychiatric conditions after delivery, such as postpartum psychosis,19,20 may lead to management variations differentially affecting certain patients. Pharmacologic agents, such as haloperidol, can be used to treat both postpartum psychosis and acute delirium, aggression, or agitation.21,22 It is unknown whether there are differences in the use of these medications after PPH in patients with and without pre-existing psychiatric disease. Advancing the understanding of PPH outcomes in mothers with a pre-existing psychiatric diagnosis may enhance the clinical care of this vulnerable population and add to the limited literature available.
Given the large prevalence of PPH and reported birth trauma in addition to the sparse data on PPH outcomes as it relates to mothers with and without a pre-existing psychiatric diagnosis, we aimed to identify PPH outcomes in a large de-identified, multi-institutional longitudinal database. The objective of this study was to determine the clinical characteristics and frequency of obstetric and psychiatric complications within 1 year after PPH diagnosis in patients with a psychiatric diagnosis prior to delivery versus those without. We hypothesize that both of these complications would be greater in patients with a pre-existing psychiatric diagnosis. We also hypothesize that medications used in psychiatric emergencies, such as haloperidol, would be greater in patients with a pre-existing psychiatric diagnosis as compared to those without within 7 days postpartum.
Materials and methods
Study design
This is a retrospective observational cohort study that was conducted using the TriNetX® (https://www.trinetx.com) electronic health record (EHR) database of postpartum women aged 15–54 years with a PPH-related diagnostic code (International Classification of Diseases, 10th edition (ICD-10) code “O72”) and who were reported to have an inpatient encounter. TriNetX is a global federated health research network that provides researchers access to continuously update data elements on EHR from participating healthcare organizations, predominantly in the United States. TriNetX is certified to the ISO 27001:2013 standard and protects healthcare data by maintaining compliance with the Health Insurance Portability and Accountability Act (HIPPA) Security Rule. The EHR data elements are aggregated and de-identified, including demographic characteristics, diagnoses, procedures, medications, laboratory values, and genomics, all in compliance with the de-identification standard outlined in Section §164.514(a) of the HIPPA privacy rule. Because no protected health information is received by the user, we were provided a waiver from the Penn State Health Institutional Review Board to perform this study (STUDY00020794). Study design, conduct, and result reporting were constructed using the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. 23
Data collection
On 5 October 2021, we analyzed the available EHR data of 10,649 postpartum females who had a PPH-related ICD diagnostic code during or after the year 2012 and were also coded to have one of the following procedures: (1) vaginal delivery or (2) cesarean delivery. To avoid subjects with repeat deliveries, we excluded subjects with a delivery coded before PPH-related ICD-10 diagnostic code entry and 90–365 days after. In addition, to minimize potential selection biases of subjects who could be lost to follow-up (i.e. subjects could have changed health systems or moved out of state), we only included subjects who had at least one encounter up to 5 years before delivery and 1 year after delivery. We excluded subjects who did not meet the above criteria.
After the query, we obtained the following data: age, race, ethnicity, Center for Disease Classification (CDC)–related maternal morbidity diagnoses 24 and related common procedural terminology (CPT), and healthcare common procedure coding system (HCPCS) codes reported up to 1 year after PPH diagnosis (see Supplementary Table 1). We used a 1-year timeframe which is consistent with maternal mortality review committees which define obstetric complications as up to 1-year postpartum. 24 We then extracted all the mental health diagnosis categories, haloperidol presence, and other psychedelic medication (as classified by the Anatomical Therapeutic Chemical Classification) presence after the PPH diagnosis. The subjects were categorized based on prior history of mental health disorder.
Statistical analysis
By the presence or absence of mental health diagnostic history, we reported the demographic characteristics (Table 1), the obstetric complications detected within 1 year after the PPH diagnosis (Table 2), and several health conditions within 1 week after the PPH diagnosis (Table 3) for the included patients using the summary statistics. Two-sample t-test was applied to compare the age between the groups with and without pre-existing mental health disorders, Wilcoxon sum rank test was used to test the difference of the numbers of complications within 1 year after PPH diagnosis between the two mental health condition groups, and Pearson’s chi-square test and Fisher’s exact test were applied for comparing categorical factors, including race, ethnicity, delivery type, and presence of certain complication or other health conditions.
Demographic factors of subjects diagnosed with postpartum hemorrhage divided by the absence and presence of a mental health diagnosis history.

SD: standard deviation.
Complications 1 year after postpartum hemorrhage diagnosis divided by the absence and presence of a mental health diagnostic code history.
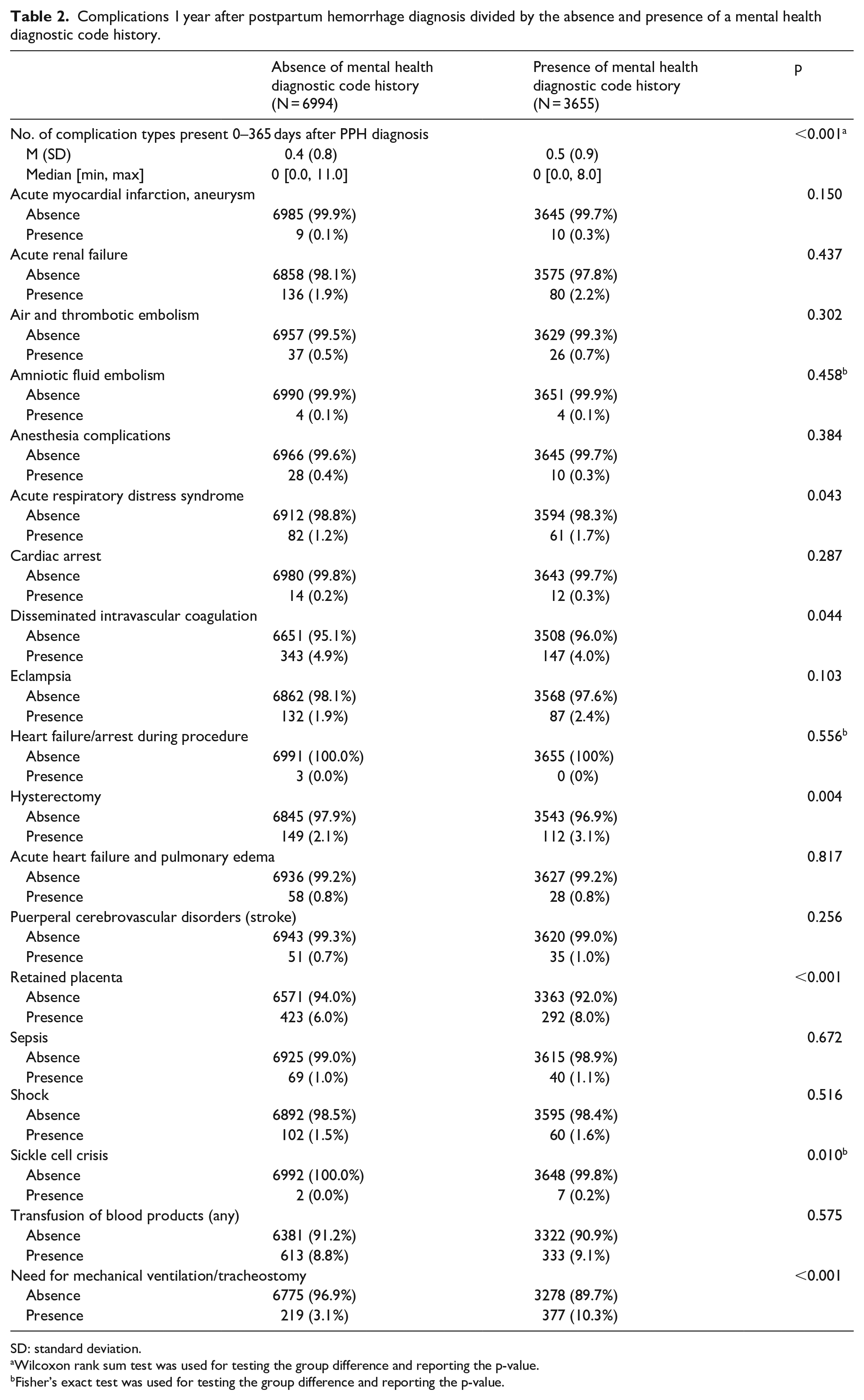
SD: standard deviation.
Wilcoxon rank sum test was used for testing the group difference and reporting the p-value.
Fisher’s exact test was used for testing the group difference and reporting the p-value.
Mental health diagnosis and psychiatric medications 0–7 days after PPH diagnosis.

PPH: postpartum hemorrhage.
We conducted univariable and multivariable logistic regression analyses to investigate the association between the presence of any complications within 1 year of PPH diagnosis and the mental health disorder history. In the analyses, we combined “Asian,” “American Indian or Alaska Native,” and “Native Hawaiian or Other Pacific Islander” in “race” to the “Other” category due to their relatively small proportions in the data. We first fit univariable logistic regression models for mental health condition history, age, race, ethnicity, and delivery mode to estimate the unadjusted odds ratios (ORs) with 95% confidence intervals (CIs). We then fit a multivariable model including all covariates to explore the effects controlling for other factors. The adjusted ORs with 95% CIs were summarized in Table 4 in parallel to the univariable analysis result.
Univariable and multivariable analysis for the presence of any complications within 1 year after PPH and association with the history of mental health disorder, age, race, ethnicity, and delivery type.

PPH: postpartum hemorrhage; OR: odds ratio; CI: confidence interval.
Statistical software R v.4.2.2 was used to preprocess the data, conduct the statistical tests, and perform the logistic regression analyses. p-values of less than or equal to 0.05 were regarded as statistically significant.
Results
Patient characteristics
A total of 10,649 subjects were included in this study (6994 (65.7%) no mental health diagnosis history prior to PPH and 3655 (34.3%) mental health diagnosis history). Patient demographics were summarized in Table 1.
Mental health disorders
Mental health diagnosis categories were summarized in Table 5. The most common mental health diagnoses reported were depressive disorders (953 (26.1%)), anxiety disorders (869 (23.8%)), maternal mental illness or substance abuse during pregnancy, delivery, or postpartum (1692 (46.3%)), and substance-related and addictive disorders (584 (16.0%)).
Categorized mental health disorders of subjects diagnosed with PPH and a mental health diagnosis history.

Several maternal morbidity indicators 1 year after PPH diagnosis
Of the severe maternal morbidity indicators identified, a higher proportion of acute respiratory distress syndrome (61 (1.7%) versus 82 (1.2%), p = 0.043), retained placenta (292 (8.0%) versus 423 (6.0%), p < 0.001), sickle cell crisis (7 (0.2%) versus 2 (0.0%), p = 0.010), and need for mechanical ventilation/tracheostomy (377 (10.3%) versus 219 (3.1%), p < 0.001) was noted in the mental health diagnosis group. There was a higher proportion of disseminated intravascular coagulation (147 (4.0%) versus 343 (4.9%), p = 0.044) noted in the group with no mental health diagnosis history.
Haloperidol and psychedelic prescription up to 7 days after PPH diagnosis
A higher proportion of haloperidol (118 (3.2%) versus 129 (1.8%), p < 0.001) and psychedelic (1380 (37.8%) versus 1983 (28.4%), p < 0.001) was noted in the mental health diagnosis history group when compared to the group with no mental health diagnosis history.
Associations between the presence of complications in 1 year after PPH diagnosis and the patient demographic and mental health characteristics
Having a mental health disorder history was associated with a higher odds of developing obstetric long-term complications (OR = 1.44 (95% CI: 1.32–1.57)), or after controlling for other factors (OR = 1.39 (95% CI: 1.26–1.52)). In univariable analysis, increasing age was associated with a higher risk of having complications (OR = 1.03 for 1-year increase (95% CI: 1.02–1.03)). Those who identified as Hispanic or Latino tended to have lower risks of complications after PPH diagnosis compared to those non-Hispanic or Latino (OR = 0.80 (95% CI: 0.72–0.90)). Finally, those who experienced a cesarean delivery tended to have a higher odds to develop obstetric complications compared to those who had a vaginal delivery (OR = 2.10 (95% CI: 1.92–2.29)).
Discussion
Consistent with our hypothesis, this study demonstrates that having a mental health disorder history is associated with higher odds of developing subsequent complications within 1 year of PPH diagnosis (OR = 1.39 (95% CI: 1.26–1.52), p < 0.001). Specifically, a statistically significantly higher proportion of acute respiratory distress syndrome, retained placenta, sickle cell crisis, and need for mechanical ventilation/tracheostomy was noted in mothers with a pre-existing mental health diagnosis. Furthermore, a higher frequency of haloperidol and psychedelic medications ordered within 7 days of a PPH experience was noted in the mothers with a pre-existing mental health diagnosis.
During the study timeframe, approximately 40% of mothers with a PPH diagnosis also had a pre-existing mental health diagnosis. Previous literature has demonstrated associations between PPH and mental health disorders. 25 There are various explanations as to why mothers with a pre-existing mental health disorder may develop PPH. This patient population is at increased risk for metabolic issues, such as obesity, which may have a modest effect on PPH risk.26 –32 The serotonergic agents used in mental health disorders may interfere with platelet aggregation and adhesion, increasing the risk for hemorrhage.33,34 It is also possible that the mood disorder itself may impact serotonin transmission resulting in platelet dysfunction and subsequent bleeding. 33 Overall trends show that rates of PPH and associated risk factors may be increasing35,36 and the rates of mood disorders in pregnancy. 37 Although PPH is difficult to predict,8,35 it is a significant cause of maternal morbidity and mortality, 8 underscoring the clinical importance of recognizing additional risk factors, such as the possible associations between PPH and mental health diagnoses.
Consistent with the literature, we identified PPH-associated complications; 8 however, our analysis demonstrates that some of these sequelae (acute respiratory distress syndrome, retained placenta, sickle cell crisis, and need for mechanical ventilation/tracheostomy) were significantly higher in mothers who had a mental health diagnosis prior to delivery. Cesarean delivery has been associated with PPH risk 38 and severe maternal morbidities. 39 After controlling for other factors, cesarean section was significantly associated with increased odds of developing subsequent complications; however, as delivery mode did not significantly differ between our two groups, this alone does not account for the higher odds of complications in mothers with a pre-existing mental health diagnosis prior to delivery. It may be possible that mothers with pre-existing mental health disorders are more medically complicated in general,40 –42 thereby increasing overall risks for complications postpartum especially after PPH.43,44 As previously mentioned, these patients are at increased risk for obesity 45 which itself increases maternal risks due to cardiovascular diseases, thromboembolism, hypertension, and stroke.46 –48 Our study was unable to account for obesity as body mass index was not consistently available in the TriNetX® database. In addition, PPH associated outcomes may be impacted by health determinants, stigma, access to care, and patient trust with the health system.49,50 Further study may be needed to understand this possible phenomenon and potentially better care for mothers with a mental health diagnosis.
Our data also demonstrated significant differences in mental health diagnoses within 7 days of PPH in mothers with a pre-existing mental health disorder. Based on data constraints and availability, it is unclear whether the mental health diagnoses after PPH were new or demonstrated clinical worsening of their pre-existing mental health condition. Further research is needed to clarify this finding; however, it may suggest that these mothers are particularly vulnerable after experiencing a birth trauma, such as PPH, especially in the immediate postpartum timeframe. Notably, in the mothers without a mental health diagnosis prior to delivery, approximately 7% of these individuals acquired a mental health diagnosis within 7 days after experiencing PPH, suggesting that these mothers are not immune to the possible psychiatric sequela associated with this birth trauma. Close monitoring of all patients who experience PPH may be warranted given our study findings.
Finally, our results also demonstrated significantly higher rates of ordering haloperidol in the pre-existing mental health diagnosis group within 7 days of a PPH diagnosis. Haloperidol is a first-generation antipsychotic that is commonly used to manage agitation or aggression and delirium.51,52 It also may be prescribed to manage the positive symptoms of patients with schizophrenia. 53 Due to data constraints, our study was unable to identify the indications for which haloperidol was ordered; however, all of these reasons are plausible. Our data show that mothers with pre-existing mental health diagnoses experienced higher rates of certain severe PPH outcomes. Some of these critical outcomes could have resulted in delirium and agitation, potentially placing the patient at increased risk of self-harm36,54 necessitating the use of a pharmacological solution. Haloperidol does have side effects and can be associated with increased mortality in particular clinical situations.43,53 It is therefore important to assess the appropriate use in every clinical context. There is a lack of guidelines for prescribing antipsychotic medications in the postpartum state52,53 and the literature has noted that caregiver distress in acute situations can lead to medication overuse. 55 Understanding the indications for haloperidol use in patients with a pre-existing mental health diagnosis who experience PPH is clinically relevant and can identify possible opportunities for improvement.52,56
Limitations
There are several limitations to this study. Due to database limitations, diagnostic codes could not be validated with the clinical notes from providers and therefore determining the timing of certain events was not possible for each subject included in the study. We only included subjects where the patient was coded to have PPH; thus, this study may have excluded patients who did not have this diagnostic code but did experience PPH. In addition, we could not establish PPH by objective criteria, such as estimated blood loss (EBL) or drop in hematocrit/vital sign changes and the severity of the illness for each subject was unknown. Similarly, we depended on clinicians to enter diagnostic codes for mental health diagnoses. It is possible that subjects did have a mental health disorder and did not have a mental health diagnostic code entered. Furthermore, we could not account for the role that obesity may have played in PPH-associated outcomes.
Conclusion
Having a mental health disorder history is associated with a higher odds of developing subsequent complications within 1 year of PPH diagnosis. Mothers with a pre-existing mental health disorder have a significantly higher frequency of certain severe PPH sequelae, including acute respiratory distress syndrome, retained placenta, sickle cell crisis, and need for mechanical ventilation/tracheostomy up to 1 year after delivery. These mothers also have higher rates of psychiatric medications ordered, specifically haloperidol, within 7 days of a PPH diagnosis. Further research and public health efforts may be needed to identify and manage the unique consequences of PPH in this vulnerable maternal population.
Supplemental Material
sj-docx-1-whe-10.1177_17455057231211094 – Supplemental material for A retrospective analysis of complications associated with postpartum hemorrhage up to 1 year postpartum in mothers with and without a pre-existing mental health diagnosis
Supplemental material, sj-docx-1-whe-10.1177_17455057231211094 for A retrospective analysis of complications associated with postpartum hemorrhage up to 1 year postpartum in mothers with and without a pre-existing mental health diagnosis by Kodi Endres, Nina Razavi, Zizhong Tian, Shouhao Zhou, Conrad Krawiec and Sona Jasani in Women’s Health
Supplemental Material
sj-docx-2-whe-10.1177_17455057231211094 – Supplemental material for A retrospective analysis of complications associated with postpartum hemorrhage up to 1 year postpartum in mothers with and without a pre-existing mental health diagnosis
Supplemental material, sj-docx-2-whe-10.1177_17455057231211094 for A retrospective analysis of complications associated with postpartum hemorrhage up to 1 year postpartum in mothers with and without a pre-existing mental health diagnosis by Kodi Endres, Nina Razavi, Zizhong Tian, Shouhao Zhou, Conrad Krawiec and Sona Jasani in Women’s Health
Supplemental Material
sj-docx-3-whe-10.1177_17455057231211094 – Supplemental material for A retrospective analysis of complications associated with postpartum hemorrhage up to 1 year postpartum in mothers with and without a pre-existing mental health diagnosis
Supplemental material, sj-docx-3-whe-10.1177_17455057231211094 for A retrospective analysis of complications associated with postpartum hemorrhage up to 1 year postpartum in mothers with and without a pre-existing mental health diagnosis by Kodi Endres, Nina Razavi, Zizhong Tian, Shouhao Zhou, Conrad Krawiec and Sona Jasani in Women’s Health
Supplemental Material
sj-docx-4-whe-10.1177_17455057231211094 – Supplemental material for A retrospective analysis of complications associated with postpartum hemorrhage up to 1 year postpartum in mothers with and without a pre-existing mental health diagnosis
Supplemental material, sj-docx-4-whe-10.1177_17455057231211094 for A retrospective analysis of complications associated with postpartum hemorrhage up to 1 year postpartum in mothers with and without a pre-existing mental health diagnosis by Kodi Endres, Nina Razavi, Zizhong Tian, Shouhao Zhou, Conrad Krawiec and Sona Jasani in Women’s Health
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.