
Abstract
McArdle disease is an autosomal recessive disorder affecting skeletal muscle glycogen metabolism. Limited data are available regarding pregnancy outcomes with this genetic condition. We present a recent case of a woman with McArdle disease, along with a scoping review of all published literature regarding pregnancy and delivery outcomes for women with McArdle disease. A total of 35 cases are summarised. Overall, pregnancy does not worsen or increase the risk for disease flare. Women can successfully deliver vaginally, with consideration of an assisted second stage recommended to reduce the risk of postpartum rhabdomyolysis.
Introduction
McArdle disease, glycogen storage disease type V, is an autosomal recessive disorder affecting glycogen metabolism within skeletal muscles. 1 The most common mutation is a nonsense mutation at pArg50X (previously known as R49X) within the myophosphorylase gene (PYGM) on chromosome 11q13. 1 Individuals are usually diagnosed before the age of 20 based on symptoms and an elevated serum creatine kinase (CK). Diagnosis is often confirmed with a muscle biopsy and/or PYGM genetic testing. 2
Affected individuals have no detectable or reduced glycogen phosphorylase activity and, therefore, are unable to break down glycogen into glucose subunits during muscle activity. 3 , 4 During periods of strenuous exercise, individuals with McArdle disease experience fatigue, muscle stiffness, and myalgias. If the exercise continues despite symptoms, painful cramping and contractures can occur. In severe instances, rhabdomyolysis, myoglobinuria, and renal failure can occur from muscle breakdown. 5 Many women experience a ‘second wind phenomenon’ where exercise become less painful as muscles switch to alternative sources of energy such as fatty acid oxidation. 6
The prevalence of McArdle disease is estimated around 1:100,000 live births, with rates in the literature varying from 1:350,000 to 1:7650. 5 , 7 Data on the effect of this condition on pregnancy, and labour and delivery are extremely limited. Here we describe a recent case along with a scoping review of all published reports of pregnancy outcomes in women with McArdle disease.
Case
A 34-year-old woman in her first pregnancy was referred to our joint Maternal-Fetal Medicine/Internal Medicine clinic for prenatal care at seven weeks of gestation. Her height was 157.5 cm and pre-pregnancy weight was 120 kg, giving a body mass index of 48 kg/m2.
As an adolescent, she was diagnosed with McArdle disease following an admission to hospital with severe rhabdomyolysis. Muscle biopsy confirmed elevated glycogen, and genetic testing confirmed a homozygous mutation in the PYGM gene (homozygous for the pArg50X mutation). Incidentally, she was also positive for myoadenylate deaminase deficiency (AMPD1 mutation). Prior to her pregnancy, she had been admitted to hospital seven times with severe rhabdomyolysis. Her baseline CK was roughly 2000–4000 U/L.
Her medical history was significant for primary hypertension (diagnosed age 27, treated with perindopril and nifedipine XL), gastroesophageal reflux, irritable bowel syndrome, chronic pain secondary to McArdle disease (treated with buprenorphine patch), dyslipidaemia (treated with rosuvastatin), and underlying proteinuria (baseline urine protein to creatinine ratio (uPCR) of 0.035 g/mmol). Prior to her planned pregnancy, the perindopril and rosuvastatin were discontinued.
At the first prenatal visit, blood pressure was well controlled on nifedipine XL 90 mg daily. Booking serology was unremarkable, TSH was 1.15 mIU/L, haemoglobin was 116 g/L, platelets were 434 × 109/L, and 75 g oral glucose tolerance test was consistent with early onset gestational diabetes mellitus.
She was admitted to hospital at 10 weeks’ gestation with an episode of rhabdomyolysis secondary to an upper respiratory infection (URTI), treated with intravenous (IV) 5% dextrose for three days. During that hospitalization, her CK rose to a peak of 35,763 U/L. Otherwise, her pregnancy was uncomplicated. She achieved good glycaemic control with dietary modification and her blood pressure was well controlled (<140/90 mmHg) throughout the pregnancy. Fetal growth at 36 weeks demonstrated an estimated fetal weight of 3138 g (82nd percentile).
At 37 weeks and 5 days of gestation, she presented to hospital with worsening home blood pressure readings. Her proteinuria was worsening (uPCR 0.089 g/mmol), uric acid was elevated at 442
Our aim was for a trial of vaginal delivery. Given that coughing had caused her rhabdomyolysis during her URTI, we felt maternal pushing should be avoided and therefore an assisted second stage was planned. A Foley catheter was inserted for cervical ripening and oxytocin was started. At the initiation of induction, her CK was 1045 U/L. An early epidural was placed for labour analgesia. Despite intravenous oxytocin administration at a rate of of 66 mU/min with an intrauterine pressure catheter in situ displaying adequate contractions (Montevideo units greater than 200), her cervix remained arrested at 5–6 cm dilated. A low transverse caesarean section was performed delivering a live female weighing 3660 g. Postpartum, her CK rose to a maximum (max) on postpartum day 3 of 9716 U/L. She remained asymptomatic, creatinine remained stable, and urine remained clear. She was discharged home on postpartum day 6. By one week postpartum, her CK returned to her baseline of 1338 U/L (Figure 1).
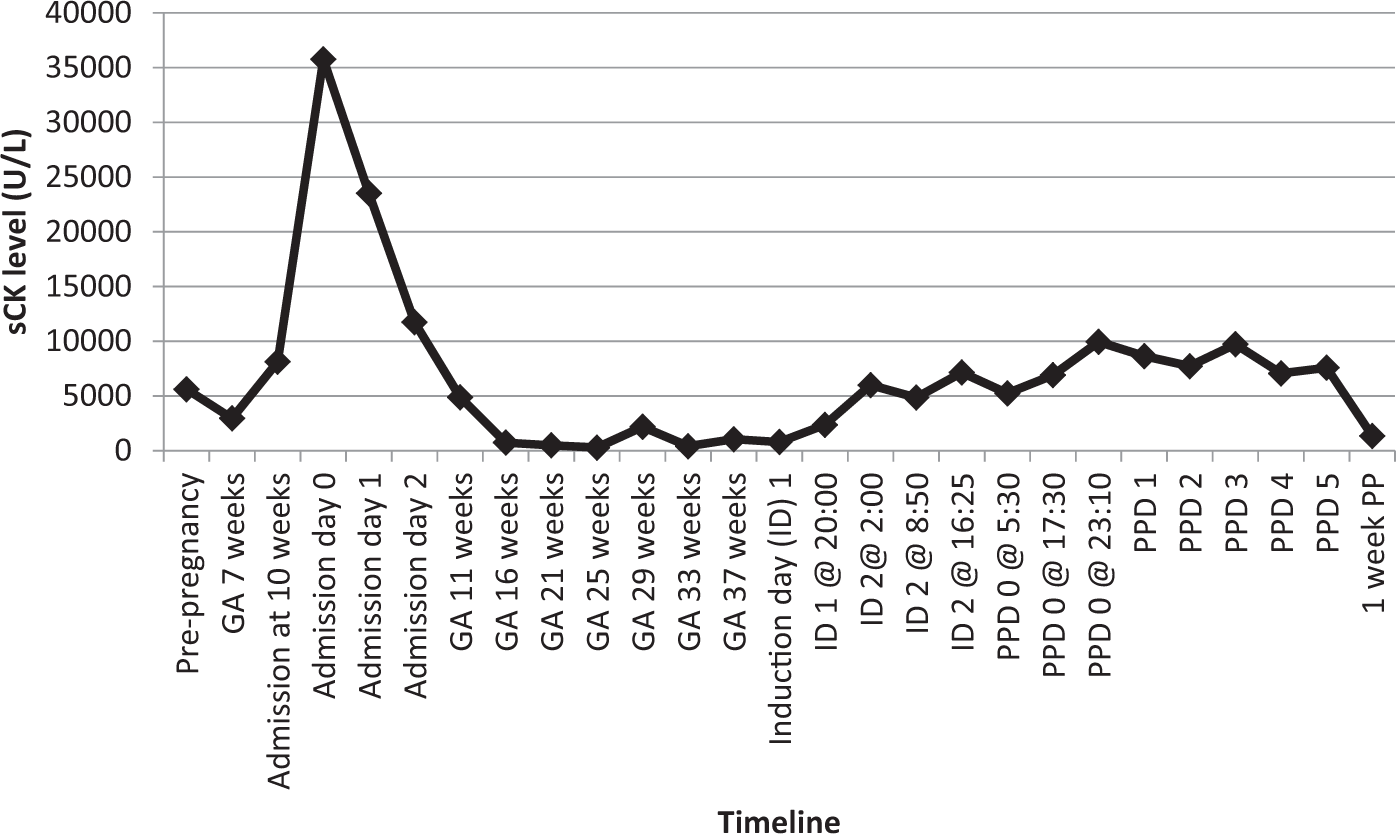
Antepartum and peripartum CK (U/L) levels in a pregnant woman with McArdle disease. GA: gestational age; ID: induction day; PPD: postpartum day.
Methods
A literature search of PubMed, Embase, Cochrane Library, and Web of Science databases was performed using key words: McArdle disease, glycogen storage disease type V, pregnancy, and pregnancy complications. The search had no language or publication type limitations. A total of 15 papers were identified; five articles were excluded after review of abstracts. 7–16 One article was on glycogen storage disease type IV, and the other four were not in English or French language.
Results
Table 1 demonstrates a summary of published cases. A total of 35 cases (including ours) were identified.
Summary of published case reports of pregnant women with McArdle disease.
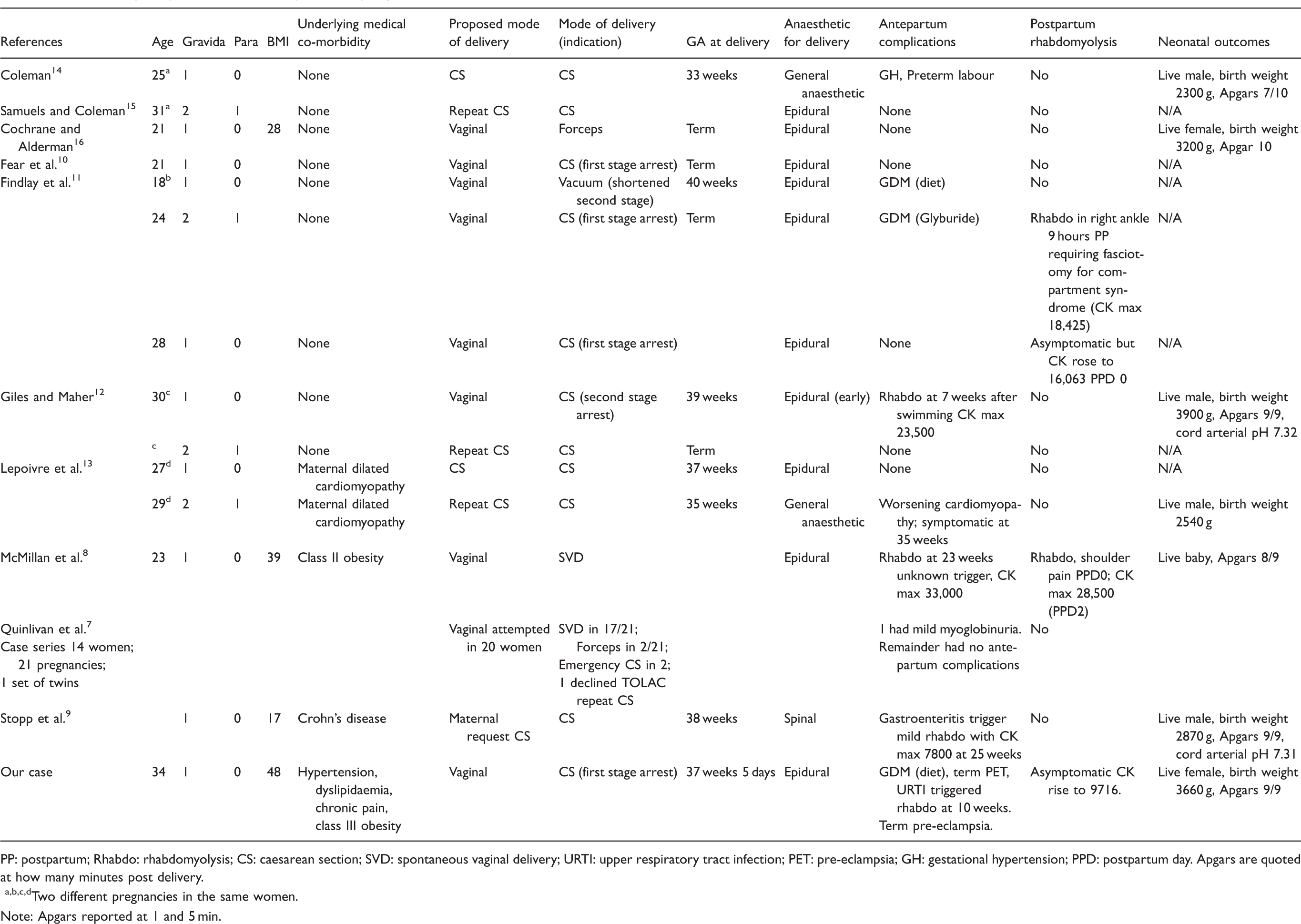
PP: postpartum; Rhabdo: rhabdomyolysis; CS: caesarean section; SVD: spontaneous vaginal delivery; URTI: upper respiratory tract infection; PET: pre-eclampsia; GH: gestational hypertension; PPD: postpartum day. Apgars are quoted at how many minutes post delivery.
a,b,c,dTwo different pregnancies in the same women.
Note: Apgars reported at 1 and 5 min.
Antepartum complications included two cases of gestational hypertension, one case of superimposed pre-eclampsia, and three cases of gestational diabetes (two diet-controlled and one treated with an oral agent). One preterm birth was documented. Although these cases represent a small sample size, no incidence of fetal loss, intrauterine fetal demise, placental abruption, or preterm premature rupture of membranes was reported.
Four cases of antepartum rhabdomyolysis were reported. Case 1 occurred at 7 weeks after swimming with a CK max of 23,500 U/L; case 2 occurred at 23 weeks after no known trigger with a CK max of 33,000 U/L; case 3 occurred at 25 weeks with a diagnosis of gastroenteritis, with a CK peak of 8000 U/L; and our case occurred at 10 weeks after a URTI with a CK max of 35,763 U/L. 8 , 9 , 12 All cases were treated supportively with IV hydration without further adverse outcomes.
The recommended mode of delivery was vaginal for 29 of the 35 reported cases, with 25 of 35 proceeding with a vaginal delivery: 22 spontaneous vaginal deliveries (SVDs) and 4 assisted vaginal deliveries. Seven women elected for caesarean section, and five required an intrapartum caesarean section. All women who laboured had an epidural for labour analgesia (not reported in case series by Quinlivan et al.). 7 No cases of postpartum haemorrhage, 3rd or 4th degree tears, shoulder dystocia, or postpartum VTE were reported.
Postpartum complications included three cases of rhabdomyolysis. Case 1 occurred following a SVD with 149 min of pushing. 8 Her CK max was 28,500 U/L day 2 postpartum, and she was treated with IV fluids with a return to baseline CK of 9708 U/L three days later. This woman had also had an antepartum episode of rhabdomyolysis. Case 2 occurred following a caesarean section for first stage arrest and manifested as right ankle pain with a CK max of 18,425 U/L. 11 She was initially treated with IV fluids, but subsequently developed compartment syndrome and required fasciotomy at 36 h postpartum. Case 3 also occurred following a caesarean section for first stage arrest with a CK max of 16,063 U/L and was treated supportively with IV fluids. 11 The series by Quinlivan et al. mentioned one woman who had mild myoglobinuria; however, no further details were available. 7
Few cases reported CK levels throughout pregnancy or immediately postpartum. Apart from the above-mentioned rhabdomyolysis cases, CK levels reported intrapartum and immediately postpartum remained unchanged in three women. 9 , 11 , 12 These women all had different modes of delivery: one caesarean section for second stage arrest, one booked caesarean section, and one planned vacuum to shorten second stage.
Apart from our case, the case study by Stopp et al. 9 is the only reported case of monitoring CK levels through pregnancy. The trend was similar between the two cases: apart from each pregnancy being complicated by a case of antepartum rhabdomyolysis, CK levels remained stable or slightly lower than baseline throughout the antepartum period. Both cases noted asymptomatic rise in CK levels from pre-labour baseline with delivery. Stopp et al. noted a rise from baseline of 1051 U/L to 3420 U/L CK on PPD 2 following elective caesarean section. Our case’s intrapartum had a rise from baseline pre-labour CK of 1046 U/L to 9946 U/L and a postpartum maximum CK of 9716 U/L (Figure 1).
Discussion
McArdle disease is a rare metabolic condition with limited published data regarding pregnancy outcomes. A total of 35 pregnancies from 24 women with McArdle disease were identified in this scoping review. Given the rarity of McArdle disease and the small population of pregnancy cases, no definitive conclusions can be made on rates of pregnancy complications including preterm birth, hypertensive disorders of pregnancy, GDM, and intrauterine death.
McArdle disease itself appears to remain stable in the majority of women throughout the pregnancy. In four reported cases of rhabdomyolysis, triggers appeared to be related to known triggers outside of pregnancy rather than the pregnancy itself. 8 , 9 , 12 Management reported was similar to outside of pregnancy, and those with rhabdomyolysis had similar pregnancy outcomes to those without antepartum episode of rhabdomyolysis. It remains unclear if fetal outcomes are affected by maternal episodes of rhabdomyolysis. Rizzardi et al. have demonstrated that human placentas are not permeable to maternal myoglobin, which may explain these reassuring findings. 17
Both the woman reported by Stopp et al. and our woman noted improvement in the CK from baseline throughout the pregnancy. 9 This improvement in CK may be due to improved muscle blood flow in pregnancy, which leads to higher oxygen supply and less need for anaerobic glycolysis, along with other metabolic changes due to pregnancy physiology. 5 , 16 Insulin resistance of pregnancy also reduces lipolysis, resulting in elevated serum free fatty acids, which provide an alternative source of energy for skeletal muscle in pregnancy. 18 Insulin resistance in pregnancy rises significantly in the second and third trimesters, which may explain why all the reported cases of antepartum rhabdomyolysis occurred prior to 23 weeks and why CK levels improved throughout the third trimester. 19 An alternative theory to the improvements in CK is that during pregnancy women are motivated to protect their developing fetus from potential harm, and are more vigilant in preventing activities, such as exercise, that may trigger rhabdomyolysis.
Optimal mode of delivery remains unclear. We feel McArdle disease itself should not be considered an indication for caesarean section. The disease itself does not affect uterine smooth muscle and therefore contractions themselves are not altered in this condition. Adequate and early analgesia in labour is important as skeletal muscle exertion and emotional stress in labour may potentially trigger rhabdomyolysis. 20 Similarly, the majority of cases ran 4–5% dextrose during labour as it is believed that this glucose supply may prevent myopathy by reducing the need to breakdown glycogen stores during labour. 8 , 12 , 14 , 16 An assisted second stage should be considered after a shortened period of pushing, as the repetitive abdominal muscle contraction required for maternal pushing effort may trigger rhabdomyolysis. One case of postpartum rhabdomyolysis occurred after a prolonged active second stage of 149 min. 8
The optimal surveillance for rhabdomyolysis in McArdle disease remains uncertain. The majority of women did not have a symptomatic episode. Both our woman and one other had asymptomatic rises in CK, therefore it may be prudent to monitor postpartum CK levels until trending downward to ensure that there is no evidence of rhabdomyolysis.
We felt that a scoping review of the published case reports was an appropriate model rather than a systematic review. This method allowed for a narrative review of all types of available studies, and permitted the broad research question of all pregnancy outcomes in this rare condition. 21 Limitations of this method include no assessment of bias within the published case reports. Similarly, pregnancy risks may be minimised due to a publication bias in the available case reports. This paper does allow for identification of pregnancy complication themes within this rare metabolic disease.
In conclusion, outcomes from the available 35 cases demonstrate relatively uneventful pregnancies. The disease may flare antepartum and/or postpartum; however, this does not appear to worsen overall pregnancy outcomes.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
None required for a scoping review.
Informed consent
Written informed consent was obtained from the patient for the publication of this case report.
Guarantor
CN.
Contributorship
CN wrote the first draft. All authors reviewed and edited the manuscript and approved the final version.
Acknowledgements
We thank Darlene Chapman for designing and performing the search for published case reports used in this study.