
Abstract
Background
Isolated sixth nerve palsy is a rare neurologic manifestation of preeclampsia suggesting severity. The purpose of this article is to describe a case of recurrent sixth cranial nerve palsy in the setting of preeclampsia and to highlight its clinical significance, management considerations, and prognosis.
Case
A 28-year-old woman presented with recurrent left sixth nerve palsy in the setting of preeclampsia at 36 weeks’ gestation. No alternative diagnosis was found in laboratory investigations and cerebral imaging. Symptoms resolved spontaneously within 5 days of delivery.
Conclusion
A case of recurrent isolated sixth cranial nerve palsy as a manifestation of preeclampsia is described. This rare finding must be recognized by those caring for pregnant individuals.
Introduction
Preeclampsia, a multisystem disorder characterized by hypertension and end-organ dysfunction occurring during pregnancy, remains a leading cause of maternal and perinatal morbidity and mortality. 1 Neurologic findings of preeclampsia can range from headaches and blurry vision, to more severe manifestations such as stroke and seizures. 2 Preeclampsia can also present with a wide range of atypical neurologic complications. Among these, cranial nerve palsies are uncommon but should be recognized as clinical markers of severity. 3
We describe a case of recurrent isolated sixth cranial nerve palsy in the setting of recurrent preeclampsia with severe features. We aim to shed light on the clinical significance of sixth nerve palsy as a manifestation of preeclampsia, highlighting diagnostic challenges, management considerations, and the need for heightened vigilance among healthcare providers caring for pregnant individuals.
Case
A 28-year-old woman in her second pregnancy presented to the Obstetric Medicine clinic at 36 + 3 weeks’ gestation. Her past medical history included chronic hypertension, migraines, and persistent proteinuria with a pre-pregnancy urine protein–creatinine ratio (UPCR) of 1.24 g/g. Her previous pregnancy, at the age of 25, was complicated by preeclampsia manifesting with headache, hypertension, horizontal diplopia, and nephrotic-range proteinuria up to 8.1 g/g. She developed left sixth cranial nerve palsy at 32 + 3 weeks’ gestation which was attributed to preeclampsia and resolved within 6 weeks postpartum.
In the clinic, she described a 1-week history of frontal headache, increasing leg edema, and worsening hypertension. On physical examination, her blood pressure was 142/102 mmHg; vital signs were otherwise unremarkable. Neurologic examination revealed decreased left eye abduction accompanied by diplopia, suggestive of left sixth cranial nerve palsy. Further neurologic examination demonstrated intact visual fields, and absence of other cranial nerve anomalies, nystagmus, internuclear ophthalmoplegia, ptosis, bulbar signs, nuchal rigidity, or other sensorimotor deficits. There was unsustained symmetric ankle clonus; the rest of her physical examination was within normal limits.
Laboratory investigations ordered included complete blood count, coagulation profile, fibrinogen, electrolytes, creatinine, and liver profile; which were normal. The UPCR was 0.71 g/g. The patient was referred to hospital for admission for preeclampsia with severe features. Magnesium sulfate infusion was initiated and labetalol was titrated targeting a diastolic blood pressure of less than 85 mmHg. Neurology was consulted and magnetic resonance imaging/magnetic resonance venography (MRI/MRV) of the brain with venous time-of-flight sequence was conducted, revealing no abnormality. Imaging was performed without a gadolinium-based contrast agent. The patient underwent uncomplicated planned caesarean section that day for a live baby of 2.9 kg. Her headache and diplopia gradually began to improve and by post-partum day #4, the sixth nerve palsy had resolved.
Discussion
Isolated sixth cranial nerve palsy is a rare, yet significant, clinical manifestation of preeclampsia. Previously described cases of sixth cranial nerve palsy as a manifestation of hypertensive disorders of pregnancy are hereby summarized (see Table 1).3–9 None of these cases represented a recurrent sixth nerve palsy along with preeclampsia. Most cases presented with preeclampsia or severe preeclampsia at the time of diagnosis and about one-third of cases occurred in the early post-partum period. All cases had normal cerebral imaging and time-to-resolution of sixth nerve palsy varied from 2 days to 6 months. 6
Reported cases of sixth cranial nerve palsy due to hypertensive disorders of pregnancy.
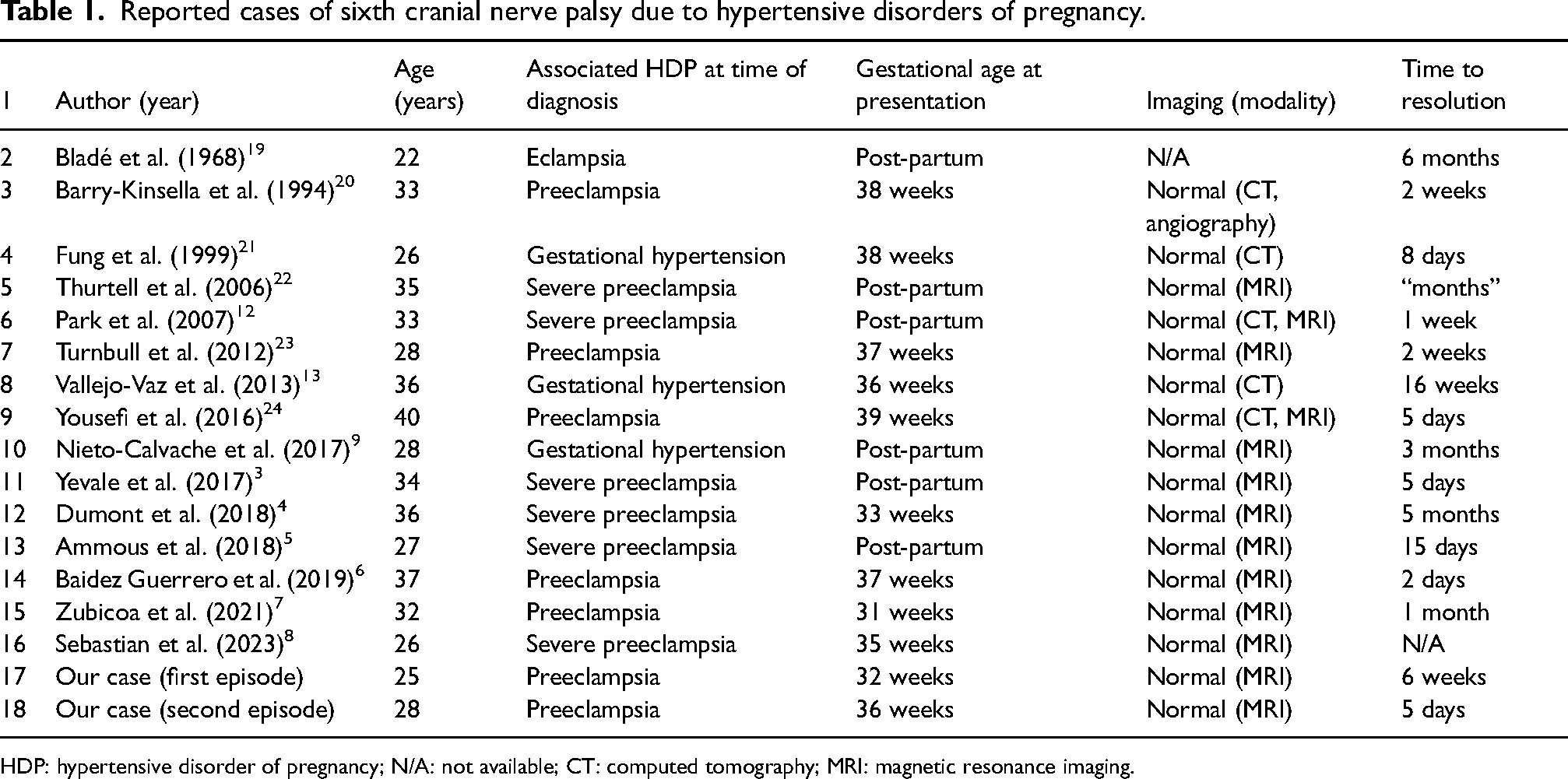
HDP: hypertensive disorder of pregnancy; N/A: not available; CT: computed tomography; MRI: magnetic resonance imaging.
The sixth cranial nerve follows an extensive intracranial route from the abducens nucleus in the pons to its innervation of the ipsilateral lateral rectus muscle. It has the longest subarachnoid course of all cranial nerves and is the most exposed nerve that traverses the cavernous sinus. 10 This lengthy intracranial trajectory renders it susceptible to a variety of intracranial pathologies, including inflammation, ischemia, and raised intracranial pressure, all of which may be caused by preeclampsia. 11
The pathophysiology of sixth cranial nerve palsy in preeclampsia is unknown. Downward displacement of the nerve due to cerebral edema, raised intracranial pressure, and nerve ischemia has been proposed. 12 However, it has been suggested that this mechanism would lead to other neurologic deficits, which are seldom reported. 13 Alternatively, sudden blood pressure changes in preeclampsia may disproportionately impact posterior cerebral structures due to regional heterogeneity in arteriolar sympathetic innervation.13,14 The posterior circulation may thus be slower to respond to sudden pressure rises. 11 This cerebral autoregulatory dysfunction may lead to vasospasm in the posterior and basilar cerebral circulations, causing transient ischemia of the nerve along its initial course. Moreover, impaired dynamic cerebral autoregulation is more pronounced in the early postpartum period, suggesting this may be a vulnerable time for pregnancy-related cerebrovascular complications, such as sixth cranial nerve palsy. 15
Sixth cranial nerve palsy due to preeclampsia is a diagnosis of exclusion. If a sixth nerve palsy is seen in the context of a horizontal gaze palsy, injury to the abducens nucleus in the pons should be suspected, which can be due to malignancy, infarct, hemorrhage, demyelinating plaque, granulomatous disease, or infection. 16 Elevated intracranial pressure can affect the nerve anywhere on its vulnerable trajectory, and venous sinus thrombosis should be excluded. 16 The inflamed meninges seen in infective or inflammatory meningitis can result in nerve entrapment. Ophthalmoplegia in the context of myasthenia gravis may mimic a sixth nerve palsy. Ophthalmoplegia seen in Wernicke syndrome or Miller Fisher syndrome can also occur. 16 Finally, epidural anesthesia may result in intracranial hypotension, traction, and subsequent ischemia of the sixth cranial nerve. 17
The investigations for sixth nerve palsy in pregnancy should be guided by the patient's clinical presentation. If preeclampsia is suspected, laboratory studies should be performed to assess for end-organ damage. All patients must undergo neuroimaging, preferably MRI/MRV to exclude space-occupying lesions leading to intracranial hypertension. Notably, MRI performed without intravenous contrast due to pregnancy may limit sensitivity in detecting pathology. Cerebrospinal fluid analysis may be considered in specific circumstances and, if pseudotumor cerebri is suspected, an opening pressure should be measured. However, lumbar puncture may increase the risk of cerebral herniation in the setting of raised intracranial pressure due to a space-occupying lesion. 18 We thus suggest that lumbar puncture be pursued in conjunction with neurological and neurosurgical input.
Preeclampsia was felt to be the most likely etiology of sixth nerve palsy in our patient, as she had manifested similarly in her prior pregnancy. Additionally, the clinical examination and normal brain MRI allowed us to exclude competing diagnoses. Ultimately, resolution of the palsy after delivery confirmed its association with preeclampsia. Although the duration was widely variable, complete recovery of sixth nerve palsy was seen in all reported cases in the literature, including our patient. Therefore, while close surveillance should be undertaken, patients and providers may be reassured of the expected benign prognosis.
Footnotes
Acknowledgments
The authors would like to extend gratitude to the patient described in this case report for allowing us to share their experience with the scientific community. IM is the guaranteeing author and affirms that this manuscript is an honest, accurate, and transparent account of the case being reported; and that no important aspects of the case have been omitted. All co-authors have read and approved the final version of the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article: This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Ethical approval
McGill University Health Centre does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from the patient for their anonymized information to be published in this article.
Guarantor
Isabelle Malhamé
Contributorship
DN wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.